Article Text

Abstract
Introduction Periodontal disease is a prevalent pathology in military personnel worldwide. The objective is to analyse the methodological features of periodontal health research performed in military personnel in their home countries.
Methods A PRISMA systematic review of literature was carried out in PubMed, EMBASE and Web of Science databases on military periodontal health studies. Study design type, language, publication date, year, country, size and sample selection, age, sex, military, diagnostic procedure, examiners, periodontal, gingival and oral hygiene index were extracted.
Results Eighty-eight out of 5355 studies found were selected, published between 1921 and 2020, with samples ranging from 52 to 16 869 individuals, generally not randomised, and consisting mainly of men with a mean age of 25 years. Predominant studies were cross-sectional descriptive studies, carried out in the Army, on American military personnel, and in the English language. Most of the studies used the WHO periodontal probe handled by two or more examiners. The Löe and Silness gingival index and the Silness and Löe plaque index were the most used indexes to assess gingival condition and oral hygiene, respectively. Community Periodontal Index of Treatment Needs was the most widely used periodontal index.
Conclusions Research on periodontal health carried out in military populations from the 1920s to the present has been performed from an almost exclusively descriptive approach. Issues such as the characteristics and representativeness of the samples, the epidemiological design and the different gingival-periodontal indexes used may limit the comparability of the study results.
- oral medicine
- oral & maxillofacial surgery
- epidemiology
- preventive medicine
- public health
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
Periodontal disease is a common chronic non-communicable pathology and is one of the main causes of tooth loss.
The periodontal health studies conducted are mainly observational and cross-sectional, in non-randomised samples of highly variable size and in young men.
The studies mainly used the WHO probe, Community Periodontal Index of Treatment Needs, Löe and Silness gingival index and Silness and Löe plaque index.
The heterogeneity of the epidemiological design and variability in the measurement of periodontal health hinder the comparability and representativeness of the results.
Introduction
Periodontal disease is a common oral pathology with a global distribution and has been defined as ‘any disorder of the tissues surrounding and supporting the teeth, commonly referred to as bacteria-induced inflammatory disorders of the periodontium’.1
The prevalence of periodontal disease is assessed through epidemiological indexes that measure the periodontal health of the population, which also allow formulation of strategies for the prevention, control and reduction of the disease. The following three types of indexes are the most used in periodontology: oral hygiene indexes (estimates biofilm and dental calculus); gingival indexes (evaluates gum inflammation) and periodontal indexes (detect periodontal disease by measuring several parameters, such as probing depth and clinical attachment level, which are the most important clinical indicators used).
In military groups, gingival-periodontal pathologies are one of the main causes of oral morbidity after dental caries, both in their own countries and in deployments abroad.2–4 At this second geographical context, having good periodontal health in the operational areas is essential, as periodontal conditions may result in temporary discharge from duty, compromising the operability of military units. An example of this situation has been the necrotising periodontal disease5 identified during the First World War as ‘trench mouth or Vincent’s stomatitis’, which originated, among other factors, because of the stress to which the military personnel were subjected, which altered their immune response and predisposed them to this disease.
Prevention is an essential pillar that contributes to reducing the number of urgent periodontal interventions in military missions abroad. To prevent the exacerbation of gingivitis or periodontitis after deployment from a non-battle environment to a leading situation, it is necessary to study the periodontal health of the military personnel beforehand using an appropriate methodology, as well as encourage oral health promotion and care in national territory. The efforts should focus on early diagnosis of gingival-periodontal pathologies and encouraging awareness regarding the importance of oral hygiene among military personnel. This includes planning and implementing a preventive and curative periodontal health policy adapted to the military environment in home countries.
There are almost no published reviews on the methodology used in the military periodontal health studies. Therefore, the objective of this study is to identify and analyse the methods used for periodontal research conducted at military facilities in their respective national territories, specifically in terms of type of study design, sample selection and size, diagnostic procedure, evaluation indexes used and implementation of the study. To identify the problems related to the methodological design of the periodontal research could ultimately help to improve military periodontal health.
Methods
A systematic review of the published scientific literature was conducted following the PRISMA guidelines (Preferred Reporting Items for Systematic reviews and Meta-Analyses).6 The search was performed on 31 December 2020, using the inclusion criteria of periodontal health studies performed in a military population on national territory, regardless of the type of study, language or date of publication.
The following studies were excluded: (a) studies on the oral health of military personnel that did not include the periodontal health aspect; (b) those referring only to periodontal emergencies or acute and rapidly progressive periodontal disorders; (c) those conducted in the area of operations because of their unstable context (stress, poor hygiene, increased tobacco consumption), which may influence an adequate diagnosis and (d) those whose abstract was not available.
PubMed, Embase and Web of Science search engines (including Scielo and Medline) were used. In the Pubmed search, the following MeSH terms were used: periodontal diseases, periodontitis, periodontal pocket, periodontal attachment loss, gingivitis, gingival haemorrhage, periodontal index, oral hygiene index, dental plaque index, dental plaque, military personnel, military health, military health services, hospitals, military and military dentistry. A complementary search was also performed in PubMed, Embase and Web of Science with the following keywords: military, conscript, soldier, Armed Forces, Army, Navy, Air Force, periodontal, gingival and dental plaque.
Information on year, country, sample size and selection, age, sex, military, design; periodontal, gingival and oral hygiene indexes; diagnostic procedure, examiners and language were extracted from each study. The mean was used as the parameter of central tendency; the SE of mean (SEM) and CI were used as the dispersion parameters.
Results
The initial search identified 2788 studies in Embase, 1907 in PubMed and 640 in Web of Science. After reviewing the abstracts, and full papers where necessary, 88 studies were found that met the required inclusion criteria to be incorporated into the systematic review.2 7–93 Figure 1 represents PRISMA flow diagram and Table 1 summarises the studies in which the authors provided relevant information regarding the epidemiological design, sample, person variables, indexes used and diagnostic procedures.
Summary of relevant epidemiological information in military periodontal health studies

PRISMA diagram illustrating the literature search and identification process. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Study design, year and context
The primary epidemiological design used (89.8%) was the observational, descriptive and cross-sectional study, where only six (6.8%) were longitudinal intervention studies and three (3.4%) were case-control.
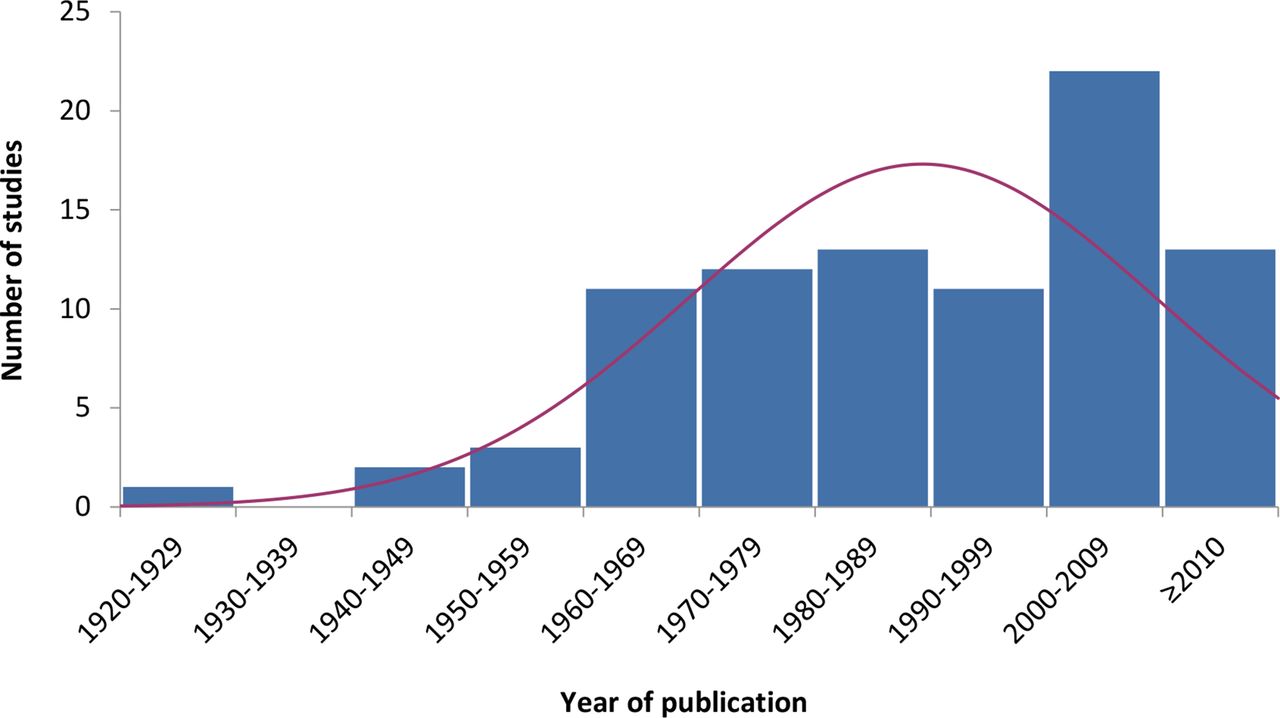
The first of the 88 analysed studies was published in 1921 and the last one in 2020; only six (6.9%) were published before 1964 and the majority were published during the first decade of the 21st century (Figure 2), especially between 2008 and 2010. Most of the studies (20.5%) were conducted on American military personnel, followed by Italian and Swiss personnel (8%). The largest number of the studies (73.9%) were published in English, 6.8% were in Italian and German, 5.7% in Spanish, 2.3% in Danish and Russian and 1.1% in French and Polish.

{kind=link}
{kind=link}
Distribution of the studies by decade of publication.
A total of 35.2% of the studies were conducted in military personnel of the Army, 12.5% in the Navy, 12.5% in the Air Force, 23.9% in joint military personnel of the Armed Forces, and 15.9% did not mention the army of origin of the sample studied. Of the 11 studies conducted in the Navy, 54.5% were carried out in the USA.
Sample features and inference
The reviewed studies were conducted in samples with a wide size range, from 52 to 16 869 individuals, and an average size of 1635 individuals (SEM=304.8). However, due to the wide sample size range, this average value has limited relevance as a parameter of central tendency. Of these, 27.3% had samples of 100–300 subjects. Of the 55 studies that indicated the sample selection procedure, only 34.5% had used a random method, and the remaining included convenience samples chosen because of different reasons, including volunteers, periodic dental examination, military service recruits, academy cadets and so on. In the studies conducted in the USA, this percentage was higher (44.4%).
A limitation found in the studies is the absence of parameters of statistical inference. Only 23 studies (26.1%) included the CI in some of the variables to measure periodontitis, 16 (18.2%) for gingivitis and 19 (21.6%) for oral hygiene. The statistical inference to the population of other parameters, such as presence of dental caries, was only reported in 20 studies (22.7%) and in 18 (20.5%) for age.
Person variables
In the 49 studies that specified the mean age of the participants, the range was 13–84 years with a mean age of 24.5 years (SEM=0.9). The reason data were reported on adolescent patients is because in one of the selected studies they belonged to the National Cadet Corps in India and on elderly patients because some studies also included retired military personnel. Only men were included in 50% of the studies and 27.3% included military personnel of both sexes. Only one study (1.1%) was conducted in women and 19 studies (21.6%) did not specify the sex of the participants in the selected sample.
Indexes and implementation procedures
The studies used various clinical parameters to assess periodontal disease, which are described below. Community Periodontal Index of Treatment Needs (CPITN) was the most used index (19 studies, 21.6%), followed by Russell index in 9 studies (10.2%) and Community Periodontal Index (CPI) and Periodontal Screening and Recording in 5 (5.7%). Only 2 studies (2.3%) used Ramfjörd Periodontal Disease Index and Navy Periodontal Disease Index and 14 studies (15.9%) used other parameters.
In 39.8% of the studies, gingival status was assessed, the most frequent index being Löe and Silness gingival index in nine studies (10.2%); gingival bleeding index (BOP) in seven studies (8%) and sulcus bleeding index by Mühlemann and Son and Papillary-Marginal-Attachment index by Schour and Massler, both in five studies each (5.7%).
Biofilm calculation was estimated in 35.2% of the studies, the most frequent indexes being Silness and Löe plaque index, in eight studies (9.1%), and Greene and Vermillion oral hygiene index and the simplified oral hygiene index by Greene and Vermillion (OHI-S), both in seven studies each (8%).
In 28 studies (31.8%), the examination was performed by one examiner and in another 37 (42%), by two or more examiners. Of the 47 studies (53.4%) that reported using a periodontal probe in their measurements, the most widely used was the WHO probe in 22 (25%) of them. In another 22 studies (25%), different first-generation probes were used, and only 2 (2.3%) used a second-generation probe and 1 (1.1%) used a third-generation probe.
Discussion
The problem of choosing an appropriate index to measure periodontal status
Until 2017, there was not a clear consensus about the clinical criteria to be used in defining periodontal disease.94 Researchers have used different epidemiological study designs and heterogeneous implementation methods. This variety of research methods, which involves the three types of indexes most used in periodontics (periodontal, gingival and oral hygiene indexes), is a relevant issue because it limits the comparability of the study results and leads to undesirable confusion in the estimation of prevalence and severity of the disease.95
Regarding periodontal indexes, the first used for epidemiological purposes was the Russell periodontal index but WHO has been using CPITN since 1987. This index was designed primarily to assess the needs for periodontal treatment of large populations rather than their periodontal status. In 1997, the CPI was introduced but only a few countries record this index due to the difficulty in its correct execution and the time involved.96 Torres et al found that both CPITN and CPI have limitations to adequately assess the prevalence of periodontal disease as they are based on a hierarchical criterion of its progression.97
In 2013, WHO introduced the modified CPI to reduce the weaknesses of the CPI and increase its simplicity and reproducibility. In this case, as with the indexes that measure caries, such as the Klein and Palmer Decayed-Missing-Filled Teeth index,98 all teeth are periodontally scanned, detailing in each tooth, the presence or absence of bleeding and periodontal pockets. This index also records attachment loss.
Dissimilar cut-off values to measuring periodontal pocket depth and level of clinical attachment to establish the existence of disease have been used. In addition, a non-homogeneous number of locations have been evaluated in each tooth and/or a simplified way of the periodontal examination of all teeth using partial registrations.99
In the set of studies analysed, the difficulty of selecting a periodontal index has been mentioned as a main issue.27 This problem also affects the use of the bleeding on probing index34 56 and advocates the need for a more comprehensive periodontal examination.11 44 68 80 83 Covington et al suggested that none of the periodontal indexes used to detect periodontal disease have been universally accepted or used routinely by most researchers.34
According to Trombelli et al, gingival indexes are subjective by nature, and researchers have based their index choice on various criteria, of which bleeding on probing is the most objective indicator to assess gingivitis.100 This is because quantitative measurement of bleeding is more difficult to analyse than the presence or absence of bleeding after probing. Furthermore, the measurement result could be influenced by the pressure exerted by the examiner, even with a slight probing.
In relation to oral hygiene indexes, their lack of precision, sensitivity and specificity as well as the need to improve intraexaminer and interexaminer concordance to increase reliability in examinations performed at different periods of time within the same centre or in multiple centres have been also mentioned as a limitation by Pretty et al.101
Due to the aforementioned differences in research methods and indexes used, it is not easy to compare prevalence and severity of periodontal pathology in military studies. Additionally, it is difficult to compare the results with civilian populations because of the differences in demographic composition, mainly by sex and age structure (the presence of female military staff is still low in armies and the mean age of military personnel is also relatively lower than the civilian population of the same geographic areas). Age is also different in the military studies reviewed (the samples in several studies are composed by conscripts and in other studies by professional military staff or veterans with different age ranges).
Issues regarding epidemiological design and implementation
The mainly descriptive epidemiological designs30 46 used have been pointed out as a research limitation by several authors,7 12 40 as well as the scarce presence of longitudinal designs,9 cohorts42 or studies assessing the level of exposure to risk factors.
There is a reduced representativeness of the study samples used48 80 due to specific issues like the samples size,11 16 54 58 non-random selection,25 45 73 83 lack of responses,60 selection biases10 33 67 and under-representation of variables27 60 64 70 85 92 which reduce data extrapolation.18 34 38 40 44 70 77 A limitation found in several studies is the absence of statistical inference parameters. The need to extend or complement the statistical analysis of the results to improve the usefulness of the study is another issue mentioned82 as well as a more extensive analysis of potential biases in order to optimise the validity of the results.36 39 58 62 64 75
As a determining factor for the comparability of the results, certain characteristics of the type of epidemiological design used in the studies have been mentioned,65 including those related to the procedures and implementation of the study17 33 71 88 90 and/or methods applied44 54 64 72 92 that establish the existence of periodontal disease.2 51 69
We need to agree on a standardised methodology for use in future studies evaluating the periodontal health of military personnel. In this sense, our proposal is to use the modified CPI and periodontal attachment level to analyse the periodontal condition as well as bleeding on probing to evaluate gingivitis, since both are objective and easy to apply in population studies. On the other hand, it is more difficult to propose an oral hygiene index among those that currently exist since none of them is universally applicable. However, the O'Leary index could be proposed to estimate dental biofilm due to its reliability and simplicity in population studies. Although an electronic probe as a measuring instrument could guarantee accuracy in measurements, its availability is not widespread. For this reason, the WHO manual probe could be the chosen alternative for conducting military epidemiological studies due to its wide availability and ease of use.
Limitations
Several limitations are recognised in the writing of this paper. We have selected studies conducted only in the home countries of the armies excluding those performed in deployment abroad as well as studies carried out only in active-duty military personnel. Furthermore, having included studies since 1921, the quality of the information provided by the authors can be variable over this long period of time.
Conclusion
Research on periodontal health carried out in military populations from the 1920s to the present has been performed from an almost exclusively descriptive approach and conducted mainly through cross-sectional observational studies. To assess periodontal status, the authors essentially used the WHO probe and three indexes: CPITN periodontal index and the gingival and plaque indexes, both developed by Silness and Löe. The limitations found related to the epidemiological design and/or its implementation may reduce the representativeness of the results and their comparability.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Acknowledgments
We would like to thank Manuel Fernández Gómez, from the Health Sciences Library of the University of Oviedo, for his invaluable help in the bibliographic search.
References
Footnotes
Contributors MBG, JMCP, GRC and PIAG are responsible for the general content of the manuscript. All contributed equally to the design, implementation of the research, analysis of results, and writing of the manuscript. The author who will act as overall guarantor is Millán Bárcena García (MBG).
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.