Article Text

Abstract
Introduction Mid-portion Achilles tendinopathy (mid-AT) is common in soldiers, significantly impacting activity levels and operational readiness. Currently, Victorian Institute of Sport Assessment—Achilles (VISA-A) represents the gold standard to evaluate pain and function in mid-AT. Our objective was to estimate VISA-A thresholds for minimal important change (MIC) and patient-acceptable symptom state for return to the presymptom activity level (PASS-RTA), in soldiers treated with a conservative programme for mid-AT.
Methods A total of 40 soldiers (40 unilateral symptomatic Achilles tendons) were included in this prospective cohort study. Pain and function were evaluated using VISA-A. Self-perceived recovery was assessed with the Global Perceived Effect scale. The predictive modelling method (MIC-predict) was used to estimate MIC VISA-A post-treatment (after 26 weeks) and after 1 year of follow-up. The post-treatment PASS-RTA VISA-A was estimated using receiver operating characteristic statistics. The PASS-RTA was determined by calculating Youden’s index value closest to 1.
Results The adjusted MIC-predict was 6.97 points (95% CI 4.18 to 9.76) after 26 weeks and 7.37 points (95% CI 4.58 to 10.2) after 1 year of follow-up post-treatment.
The post-treatment PASS-RTA was 95.5 points (95% CI 92.2 to 97.8).
Conclusions A VISA-A change score of 7 points, post-treatment and at 1 year of follow-up, can be considered a minimal within-person change over time, above which soldiers with mid-AT perceive themselves importantly changed. Soldiers consider their symptoms to be acceptable for return to their presymptom activity level at a post-treatment VISA-A score of 96 points or higher.
Trial registration number NL69527.028.19.
- sports medicine
- foot & ankle
- orthopaedic sports trauma
Data availability statement
Data are available on reasonable request. The data supporting the findings of this study are available from the corresponding author on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
The ability of Victorian Institute of Sport Assessment—Achilles (VISA-A) to detect true changes in health status is population-specific and context-specific. VISA-A thresholds for minimal important change (MIC) and patient-acceptable symptom state for return to presymptom activity level (PASS-RTA), regarding active soldiers treated for mid-portion Achilles tendinopathy (mid-AT), are currently lacking.
In a non-military population, the MIC for VISA-A was found to be 14 points after 12 weeks and 7 points after 24 weeks.
WHAT THIS STUDY ADDS
In soldiers, thresholds for MIC VISA-A were 6.97 points (95% CI 4.18 to 9.76) after 26 weeks (post-treatment) and 7.37 points (95% CI 4.58 to 10.2) after 1 year of follow-up.
In soldiers, the post-treatment threshold for PASS-RTA was 95.5 points (95% CI 92.2 to 97.8) after 26 weeks.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Values for MIC VISA-A can be used to determine the number of responders in clinical trials or to a certain treatment in clinical practice and also by clinicians to interpret change scores in light of the probability that an individual soldier with mid-AT experiences a meaningful change.
The PASS-RTA VISA-A may guide clinicians in rehabilitating soldiers treated for mid-AT.
Introduction
Mid-portion Achilles tendinopathy (mid-AT) is defined as persistent Achilles tendon pain 2 to 7 cm proximal to the calcaneus and with loss of function related to mechanical loading.1 2 Mid-AT is most common between the ages of 30 and 50 years.3 Symptoms can be long lasting despite state-of-the-art treatment.4 5 In the general population, up to 60% reports pain after 5 years of follow-up,6 and 37% still experiences some level of pain and reduced function after 10 years of follow-up.4 Mid-AT is also very common among soldiers and can have a profound impact on physical activity levels and military operational readiness.7 8 A previous diagnosis of tendinopathy is considered the strongest risk factor for mid-AT.2 7
The Victorian Institute of Sport Assessment—Achilles (VISA-A) is recommended as a patient-reported outcome measure to evaluate the clinical course of mid-AT.2 3 VISA-A is a validated, disease-specific questionnaire that assesses pain, function in daily living and sporting activity.9 Despite thorough validation, the responsiveness of VISA-A, that is, the ability to detect true changes in health status, may depend on several factors including population characteristics, interventions and period of follow-up.10 11
The minimal important change (MIC) is defined as a threshold for a minimal within-person change over time, above which patients perceive themselves as importantly changed.11 The MIC has limited generalisability across patient groups.10 No studies so far have estimated the MIC for VISA-A in soldiers with mid-AT. Moreover, no MIC for mid-AT has been reported beyond a 24-week follow-up period,5 12 13 hampering the current interpretation of long-term follow-up VISA-A change scores.
The patient-acceptable symptom state (PASS) is defined as the threshold beyond which patients consider themselves to be well.14 MIC and PASS are complementary as they reflect the patients’ perspectives of ‘feeling better’ (MIC) and ‘feeling good’ (PASS).14 A PASS indicating return to presymptom activity level (PASS-RTA) for soldiers treated for mid-AT is currently lacking. Such a threshold may aid in preventing a recurrence of mid-AT.
Therefore, our objective was to determine post-treatment both the MIC VISA-A and PASS-RTA VISA-A in soldiers treated with a conservative programme for mid-AT. Additionally, we aimed to determine MIC VISA-A at 1 year of follow-up.
Methods
Study design and setting
The data were collected as part of a large prospective cohort study (https://www.toetsingonline.nl/to/ccmo_search.nsf/Searchform?OpenForm, file number ToetsingOnline NL69527.028.19), aimed to evaluate a conservative treatment programme for soldiers suffering from mid-AT. The study was conducted at the Sports Medicine Centre of the Department of Training Medicine and Training Physiology of the Royal Netherlands Army, Utrecht, the Netherlands.
Eligibility criteria
Consecutive patients, consulting the Sports Medicine Centre for mid-AT between July 2019 and January 2021, were eligible for inclusion based on the following criteria: (1) military personnel (18–60 years) in active duty; (2) a clinical diagnosis of mid-AT2 and (3) symptoms for 2 months or more. In case of bilateral symptoms, only the side with the lowest score on the VISA-A questionnaire was included into the analysis.
Participants were excluded on the basis of: (1) concomitant insertional Achilles tendinopathy (ins-AT); (2) signs of a complete Achilles tendon rupture; (3) prior Achilles tendon surgery; (4) use of statins fluoroquinolones, or corticosteroids15 and (5) a previous diagnosis of rheumatoid arthritis, diabetes mellitus or psoriasis.15 All participants were recruited by the main researcher (MP, physical therapist).
Patient and baseline characteristics
The following patient characteristics were retrieved at baseline: age (years), height (cm), weight (kg), body mass index (%), gender (male/female), symptom duration (months) and baseline VISA-A score.9
Conservative treatment programme
The 26-week conservative treatment programme used in this study has been published in detail.16 In short, this programme consisted of: patient education;2 focused extracorporeal shockwave therapy (four weekly sessions during the first 4 weeks); an individualised exercise programme on a stair climber or cross-trainer (at least two weekly sessions during the first 8 weeks); followed by a return to running programme (up to three weekly sessions from week 8 to 26).16
Study procedures
The follow-up measurements for this study consisted of a self-administered, written VISA-A questionnaire,9 a 7-point Global Perceived Effect (GPE) scale11 and a so-called anchor question (yes/no): ‘Have your mid-AT symptoms recovered to such an extent that you were able to return to your presymptom activity level?14
VISA-A scores can range from 0 to 100, where 100 equals a perfect asymptomatic score. The GPE expresses self-perceived recovery as 1: very much improved; 2: much improved; 3: little improved; 4: no change; 5: a little deterioration; 6: much deterioration and 7: very much deterioration.
VISA-A was taken at baseline, at the end of the conservative treatment programme (after 26 weeks) and at 1-year post-treatment (after 78 weeks). The GPE was taken after 26 weeks and at 1 year of follow-up (after 78 weeks). The anchor question was evaluated post-treatment.
Statistics
Analyses were performed using SPSS (IBM SPSS Statistics for Windows, V.25.0, IBM, Armonk, New York, USA) and according to the recommendations of Terwee et al.11 Baseline characteristics of our study population were presented with appropriate measures of central tendency and dispersion. The MIC was estimated using the predictive modelling method (MIC-predict), which is an anchor-based method relating VISA-A change scores to the GPE.11 17 First, the correlations between the numeric VISA-A change scores (after 26 weeks and at 1 year of follow-up), and corresponding categorical GPEs were calculated using Spearman’s rank correlation coefficients.18 Validity was assumed at a correlation of at least 0.30.11 When data were deemed valid for estimation of the MIC the 7-point GPE was dichotomised to ‘not improved’ (scores 4–7) and ‘improved’ (scores 1–3).11 17 In case the percentage of improved patients was not approximately 50%, the adjusted MIC-predict was used.11
The PASS-RTA was estimated using receiver operating characteristic (ROC)-analysis in SPSS, by plotting the VISA-A post-treatment scores after 26 weeks to the return to presymptom activity level outcomes. The area under the curve (AUC) was interpreted as ‘failed’: 0.5–0.6; ‘poor’: 0.6–0.7; ‘fair’: 0.7–0.8; ‘good’: 0.8–0.9 and ‘excellent’: 0.9–1.0.19 Youden’s index was calculated to maximise sensitivity and specificity, using the formula: (sensitivity+specificity) − 1. The PASS-RTA was determined with Youden’s index value closest to 1. Finally, the 95% CIs around MICs and PASS-RTA were calculated.20
Results
A total of 40 soldiers were included in this study. None were lost to follow-up.
Patient characteristics are presented in Table 1.
Patient characteristics of active soldiers with mid-AT
Spearman’s rank correlation coefficients between VISA-A change scores and the GPE at 26 weeks and between VISA-A change scores and the GPE at 1 year of follow-up were 0.46 (p 0.003) and 0.53 (p 0.000), respectively. Both values met the minimum threshold of 0.30 for assuming validity of the anchor.11 Dichotomisation of the GPE indicated improvement in 95% (38/40) of all patients after 26 weeks and in 93% of all patients (37/40) at 1 year of follow-up. As the percentage of patients reporting improvement largely exceeded 50%, the adjusted MIC-predict was used to correct for bias (ie, overestimation of the MIC).17 The adjusted MIC-predict was 6.97 points (95% CI 4.18 to 9.76) after 26 weeks and 7.37 points (95% CI 4.58 to 10.2) after 1 year of follow-up post-treatment.
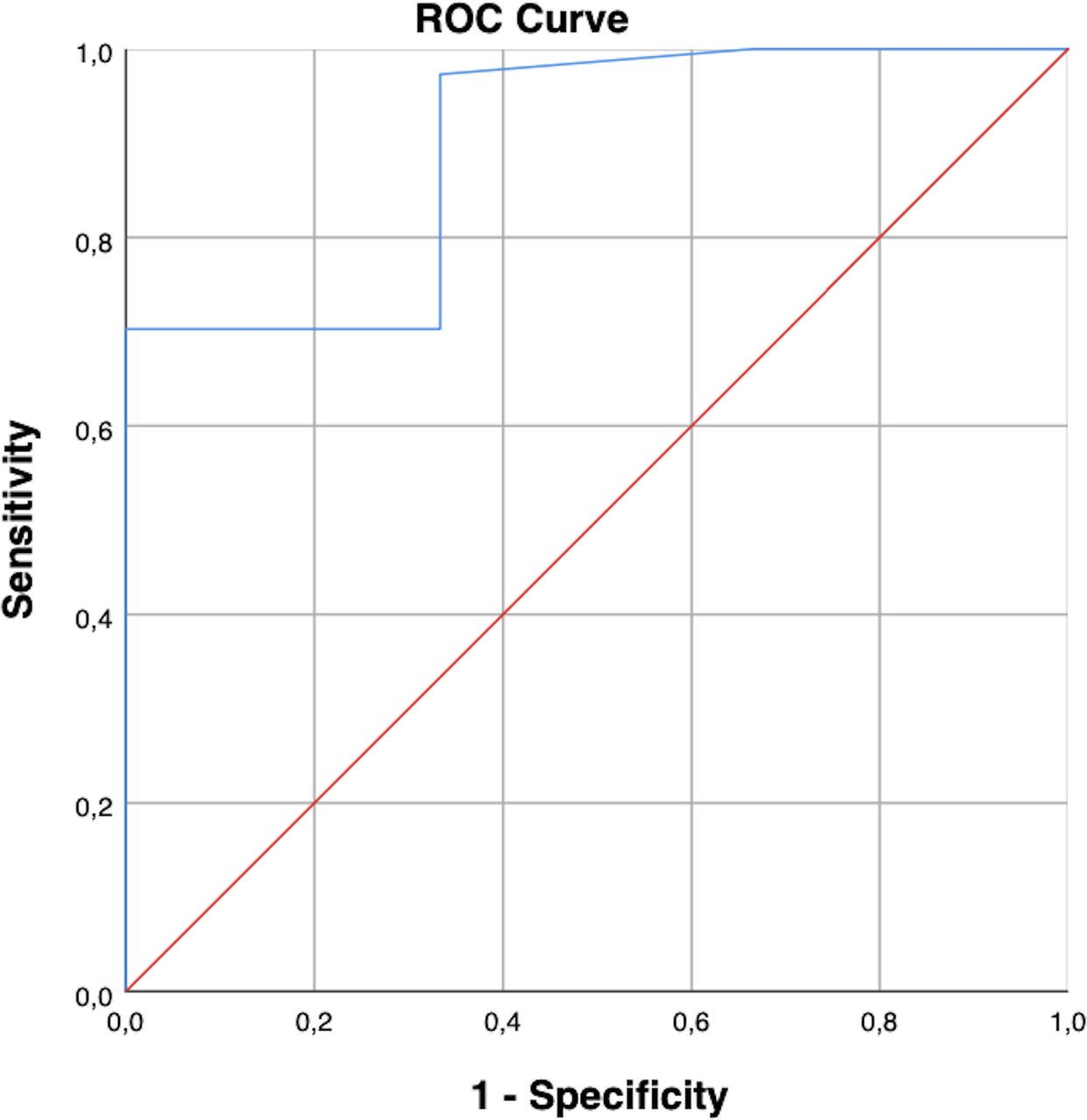
The post-treatment PASS-RTA was 95,5 points (95% CI 92.2 to 97.8) (Figure 1). The corresponding AUC was 0.896 (95% CI 0.728 to 1.000).
{kind=link}
The ROC curve expresses the ability of VISA-A to distinguish patients that were able to return to their presymptom activity level from patients who were unable to return to their presymptom activity level. Diagonal segments are produced by ties. PASS-RTA, patient acceptable symptom state for return to presymptom activity level; ROC curve, receiver operating characteristic curve; VISA-A, Victorian Institute of Sport Assessment—Achilles tendon.
Discussion
This is the first study to report VISA-A thresholds for both MIC and PASS-RTA, in soldiers treated with a standard care programme for mid-AT. Our values for MIC can be used to identify responders in clinical trials or to a certain treatment in clinical practice and also by clinicians to interpret VISA-A change scores in light of the probability that an individual soldier experiences a meaningful change.11 The PASS-RTA provides an estimate for soldiers to return to their presymptom activity level.
We have found an adjusted MIC-predict value of 6.97 points (95% CI 4.18 to 9.76) after 26 weeks (post-treatment) and an adjusted MIC-predict value of 7.37 points (95% CI 4.58 to 10.2) at 1 year of follow-up. The post-treatment PASS-RTA was 95.5 points (95% CI 92.2 to 97.8) in our study. Two remarks need to be made to put our results for MIC and PASS-RTA into perspective. First, when evaluating treatment progress in soldiers with mid-AT, it is important to acknowledge that in a general population VISA-A scores can be expected to improve 21 points, on average, following state-of-the-art treatment.21 Second, in a systematic review, Iversen et al22 reported that mid-AT patients rarely achieve VISA-A scores equal to those of uninjured healthy controls.22 The authors concluded that a VISA-A score of 90 points can be considered full recovery from mid-AT.22
We can compare our MIC of 6.97 points post-treatment with a recent non-military study by Lagas et al5 in mid-AT patients that reported a comparable MIC value of 7 points (95% CI −10 to 28) after 24 weeks of treatment. In the latter study, the MIC was found to be higher after 12 weeks of follow-up, as the authors reported a value of 14 points (95% CI 3 to 19). We were unable to retrieve studies estimating MIC VISA-A beyond a 24-week follow-up period. Therefore, we cannot compare our MIC after 1 year of follow-up to the existing literature.
Concerning PASS, Lagas et al5 reported values of 50 points (95% CI 47 to 70) after 12 weeks and of 60 points (95% CI 38 to 80) after 24 weeks. Their PASS value at 24 weeks was considerably lower than our PASS-RTA of 95.5 points after 26 weeks. Our higher PASS-RTA may well be the result of generally high physical requirements for soldiers, with respect to work and sports. It should be acknowledged that different PASS definitions may make comparisons difficult: our PASS-RTA focused on the resumption of presymptom activity level, while Lagas et al5 estimated a PASS defined as a general acceptable symptom state.
Two more non-military studies have estimated the MIC VISA-A in mid-AT,12 13 using different statistical methods. De Vos et al12 suggested a MIC value between 10 to 15% of the VISA-A scale reporting a value of 12 points. Tumilty et al13 defined the MIC as the minimum score or higher achieved by 75% of the patients in their longitudinal study, reporting a value of 16 points after 12 weeks. The statistical methods used in these two studies do not meet the current definition of MIC,11 since they do not estimate either a minimal within-person change over time or provide an actual threshold above which patients perceive themselves as importantly changed.
Currently, there is discussion about the concept of MIC in the literature, questioning the validity of published values.11 The discussion mostly relates to inconsistencies in clinical terminology used for MIC and to a variety of methods used to estimate MIC values, of which some are less methodologically sound.11 Therefore, Terwee et al11 conducted a systematic review aiming to provide practical guidance for estimating methodological sound MIC values, discussing three anchor-based methods: the MIC-predict method, the MIC-roc method and the Mean change method or MIC-mean method.11 We have used the MIC-predict method, which uses logistic regression analysis to estimate the MIC, with the dichotomised GPE as our dependent variable and the VISA-A change score as the independent variable.11 17 The MIC-predict method is based on the predicted probability that, on the basis of the observed VISA-A change score, a patient belongs to the improved group on the GPE.11 17 The MIC-roc method uses ROC statistics and is based on the ability of a measurement instrument to distinguish improved from not improved patients on an anchor.11 The MIC-roc is defined as the value for which the sum of the proportions of misclassifications ([1-sensitivity]+[1-specificity]) is the smallest.11 The MIC-predict method and MIC-roc method should be used over the MIC-mean method, as they provide an actual threshold between improved and not improved patients, while the MIC-mean does not reflect a threshold for minimal improvement, but rather a mean in a (usually small) subgroup of patients reporting ‘little improvement’. The MIC-predict method is considered the most appropriate anchor-based method, as it is more precise than the MIC-roc and can be corrected for bias if the percentage of patients reporting improvement is not about 50%.11
Strengths and limitations
We have conducted our study according to recent recommendations for MIC studies.11 We used the proposed definition of MIC to avoid inconsistency in terminology (eg, minimal clinical important difference, minimal important difference, meaningful change threshold, minimal detectable change), as seemingly interchangeable terms sometimes refer to different concepts.11
A disadvantage of all anchor-based methods is the concern about reliability and validity of the anchor question, as recall bias may occur over time.11 Therefore, in advance, we calculated the correlation between the VISA-A change scores and corresponding GPEs, which indicated that our data were suitable for estimating the MIC.11
For MIC studies, a minimum sample size of 100 patients has been recommended.11 Although we have included 40 soldiers in our study, we cannot substantiate this being an actual limitation, as we have found significant results for MIC values and PASS-RTA. This may be the consequence of using the currently preferred MIC-predict method that has shown to increase statistical power in MIC studies compared with the MIC-roc method.17
Although the soldiers included in this study were all recreational runners and mostly male (38/40), they held a variety of military job functions that reflect the variety in physical activity levels within the military.
Recommendations for future studies
We have estimated MICs for improvement. A MIC for improvement may not be the same as a MIC for deterioration.11 Therefore, caution is warranted when generalising our MICs to individuals reporting deterioration. Future studies may address if, and to what extent, MIC VISA-A values for improvement differ from values indicating deterioration.
Finally, we would like to emphasise that mid-AT and ins-AT are considered different clinical entities in the literature,23 with different responses to treatment.24 25 Therefore, we would like to recommend that future studies aiming to estimate the MIC in Achilles tendinopathy perform analyses for mid-AT and ins-AT separately.
Data availability statement
Data are available on reasonable request. The data supporting the findings of this study are available from the corresponding author on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The study was conducted according to the principles of Good Clinical Practice and was approved by the ethics committee METC Brabant, Tilburg, The Netherlands (number of approval 1921). Participants gave informed consent to participate in the study before taking part.
References
Footnotes
Contributors MP, EWPB, PHH and FJGB: contributed to the conception and design of the study. MP, EWPB, PHH: contributed to the acquisition, analysis and interpretation of data. MP, EWPB, PHH and FJGB: drafted the manuscript or revised it critically for important intellectual content. MP is acting as guarantor. All authors read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer The opinions or assertions contained herein are the private views of the authors and are not to be construed as official or reflecting the views of the Department of Defense or Dutch government.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.