Article Text

Abstract
This paper describes the development of the UK military's Ebola Virus Disease Treatment Unit (EVD TU) that was deployed to Sierra Leone as part of the UK response to the West African Ebola virus disease (EVD) epidemic in 2014 and 2015. It highlights specific challenges faced within this unique Field Hospital environment. The military EVD TU was initially established to provide confidence to international healthcare workers coming to Sierra Leone to assist in the international response to the EVD epidemic and formed a key part of the action plan by the UK's Department for International Development. It was designed and staffed to provide a high level of care to those admitted with suspected or confirmed EVD and was prepared to admit the first patient within 6 weeks of the original activation order by the Ministry of Defence. This article outlines the main hazards perceived at the outset of the operation and the methods used to mitigate the risk to the healthcare workers at the EVD TU. The article examines the mechanisms that enabled the hospital to respond positively to challenges that emerged during the deployment, while simultaneously reducing the risk to the healthcare workers involved in care delivery.
- Ebola virus disease
- Treatment Unit
- Mitigation
- Risk
Statistics from Altmetric.com
Introduction
The epidemic of Ebola virus disease (EVD) in West Africa is the largest and most complex that the world has ever seen. On 9 August 2014 the WHO declared the Ebola outbreak a public health emergency of international concern; and this triggered a coordinated response from the UK Government. The response of the UK Defence Medical Services (DMS) to the EVD outbreak from initial planning through to handover of the unit in June 2015 (Op GRITROCK) is summarised by Bricknell et al.1
In the UK, the DMS are unique in their capability to deploy a field hospital at short notice. This capability was provided by the designated ‘Vanguard’ hospital, at the time 22 Field Hospital, who were initially given the mission to command the Kerry Town Ebola Virus Disease Treatment Unit (KTTU) for up to 60 days, but not longer than 120 days, before handing over the facility to a non-governmental organisation (NGO). Due to the nature of the rapidly evolving epidemic initial timelines were tight, 22 Field Hospital were activated to train for this role, on 28 September 2014, deployed to Sierra Leone on 16 October and the official opening of the KTTU was 5 November 2014. The intent was to provide a facility that would reassure healthcare workers (HCWs) working in Sierra Leone, while being safe to those working within it.
This article describes in detail how the military-run KTTU functioned within this response and how it built on existing infrastructure, manning, training and clinical governance structures to create a new ‘Field Hospital paradigm’. This new paradigm includes the construction and development of the KTTU, intended to provide reassuringly high quality care to those involved in the EVD disaster response. The facility was designed to diagnose, and manage EVD cases and treat them to a higher standard than that otherwise available in West Africa. Later the role was changed to also provide a staging post for international HCWs with EVD prior to repatriation to their country of origin.
Designing and developing the infrastructure and systems to provide high quality clinical care
It was clear from the initial medical estimate and risk assessment that Op GRITROCK demanded a shift in mindset and would push the boundaries of EVD clinical care delivery in West Africa. The Vanguard Hospital was a mobile deployable facility accustomed to managing surgical patients supporting a wider military task. It had no experience in functioning as a treatment unit designed to manage patients with a highly infectious viral haemorrhagic fever. In fact within the DMS, there was only one healthcare worker, a Specialist Registrar in Tropical Medicine, with prior experience of managing patients with the EVD in Guinea and Sierra Leone while seconded to the WHO. Preparation of personnel would be crucial to provide a safe working environment for those DMS personnel being deployed to work in the clinical environment.2
The short timelines meant there was limited situational awareness, with no opportunity for the hospital command staff to conduct a reconnaissance or send an advance party to the Kerry Town site prior to deployment. Individual augmentees were force generated at short notice to start an intense and bespoke training package at the Army Medical Services Training Centre, Strensall, UK. Alongside the training package, standard operating procedures (SOPs) were developed by command and clinical staff which were trialled during the validation exercise. Personnel adjusted to the task ahead and clinical teams began to form; it was clear from the training that the challenging physical environment required a strong multidisciplinary approach. Led by a senior Infectious Diseases and Intensive Care consultant, a ‘Clinical Care Bundle’ was produced. This was developed using the principles of critical care organ support, the published literature and emerging guidelines on EVD management.3 ,4 Once implemented the bundle aligned how patients with EVD would be risk stratified and medically managed (Box 1). Each tranche updated this bundle as new knowledge and experience was gained.
Key components of clinical care at the EVD TU
High clinical staff:patient ratio.
A range of nursing specialties and critical care, general internal medicine and infectious disease medical expertise.
Treatment provided according to the ‘DMS EVD clinical care bundle’ with regular audit of data and outcomes.
A 24 h high dependency unit model of care focused on fluid and electrolyte management, management of coinfections and vasopressor support.
Routine use central venous access and ultrasound guided fluid resuscitation.
Blood product replacement guided by clinical syndrome and laboratory parameters.
Access to point of care tests (i-STAT) and on-site laboratory support for routine and EVD diagnostics.
Focus on symptomatic management and nutritional support.
Provision of palliative care provision and management of all patients with respect and dignity.
Strict adherence to infection, prevention and control protocols at all times.
DMS, Defence Medical Services; EVD, Ebola virus disease; EVD TU, Ebola virus disease treatment unit.
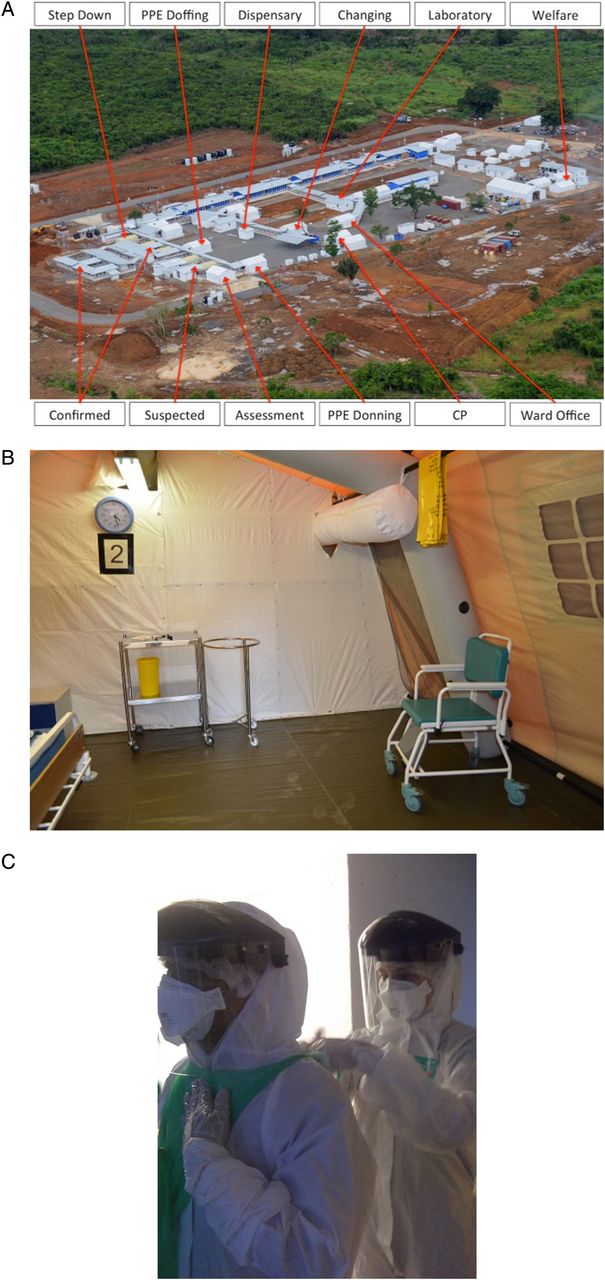
On 16 October 2014, 22 Field Hospital deployed to Sierra Leone. On arrival in country the military KTTU facility, which was collocated with an Ebola virus disease treatment unit (EVD TU) run by the NGO ‘Save the Children International’, was already under construction.5 The military EVD TU was to provide a capability to manage HCWs with confirmed or suspected EVD and work alongside the 80 bed unit operated by Save the Children International (Figure 1A). Healthcare facilities are well-recognised ‘amplifiers’ of EVD transmission during outbreaks and this must be considered and prevented. The careful design of Ebola treatment centres allows for the correct ‘flow’ of patients and staff that is essential to create a safe working environment, and to minimise the risk of nosocomial transmission. The building of the EVD TU was undertaken by the UK Royal Engineers in partnership with local contractors to meet the specification and designs of the DMS planners. On arrival in the country, the command and clinical teams were able to influence the final construction of the TU and the assessment area and suspect wards were modified to reflect the SOPs developed in training. A final simulated exercise was undertaken in the facility to quality assure the training and preparation phase prior to receiving the first confirmed patients with EVD.

{kind=link}
(A) The military EVD TU Kerry Town. Areas not labelled include the colocated, 80 bedded Save the Children International EVD TU, a joint logistics area, a joint pharmacy and a mortuary. (B) A ‘suspect’ room during the stimulation exercise prior to the opening of the EVD TU at the beginning of November. It illustrates the separation provided by these rooms giving those patients admitted with confidence that their risk of cross-contamination would be low combined with a reasonable level of comfort while they awaited an update on their diagnosis. (C) The donning and doffing areas in the EVD TU. An area at the side of the EVD TU was designed to provide a space for the staff entering the ‘red zone’ to don their personal protective equipment using the buddy pair system. This system enhanced the safety of those individuals entering the red zone as the buddy would supervise procedures, assist with patient care and support the other in the unfortunate event of a collapse or illness within the facility. CP, control post; EVD TU, Ebola virus disease treatment unit; PPE, personal protective equipment.
Patients with symptoms consistent with EVD would be admitted to their own room with access to their own toilet and shower while waiting for a diagnosis. This separation of beds containing suspected EVD cases provided confidence to those admitted that transmission of the disease from EVD positive to negative patients would be prevented. Colocated and supporting the facility was a pharmacy, a military laboratory which provided the ability to do blood tests and provide blood products and a Public Health England laboratory enabling rapid EVD diagnosis. These diagnostic capabilities provided essential support to the clinicians and improved the initial understanding of the disease. This allowed the protocols to be reviewed and updated as the operation progressed, in order to optimise care delivery. It was soon recognised that the initial handover to an NGO at the 60-day point could not be met and there would be a requirement for further clinical tranches. During Op GRITROCK, the military EVD TU capacity changed as the outbreak epidemiology evolved, from 12 to 20 to 10 beds and finally, to eight beds.
Figure 1A illustrates the KTTU layout. The military EVD TU was located in a rural location with forest being cleared prior to construction. The main treatment areas, termed the ‘red zone’, were divided into an assessment area for receiving patients, a ‘suspect’ area for the investigation and management of suspected EVD cases, a ‘confirmed’ area for EVD cases and a ‘step-down’ area for the less intense care of recovering patients with EVD. Suspect consisted of four beds separated into individual isolation rooms (Figure 1B); confirmed originally had the capacity to treat 16 patients with EVD, but changed during the course of the operation and there were an additional four step-down beds available. Discrete areas were constructed for the donning and doffing of personal protective equipment (PPE) (Figure 1C).
Understanding and mitigating the risk
It was clear that detailed preparation and planning was required to mitigate the risk of infection to the EVD TU clinical staff. The optimal approach depended upon several factors including: a clear understanding of the likely means of transmission in a healthcare environment; trust in the efficacy of protective measures and prudence in their use and an approach to patient care that minimised hazard while maximising worker safety and effectiveness.3 The provision of medical care to critically ill patients can be challenging in any setting, particularly resource-limited remote environments. The application of appropriate skills and adherence to defined protocols makes the care of patients with EVD less daunting and hazardous. It must also be recognised that despite extensive protective measures the absolute risk cannot be eliminated, and the chance of ‘individual error’ remains. A comprehensive approach to staff safety is required by clinical and non-clinical leaders to limit the likelihood of these errors. All entries and exits from the red zone were recorded. Regular clinical governance meetings were implemented incorporating significant event analyses (SEA). The senior nursing officer was responsible for recording all SEAs and PPE breaches within the red zone (the clinical area containing suspected or confirmed patients with EVD), with the information being promulgated to Permanent Joint Headquarters.
Initial risk assessments focused on the risk to personnel of acquiring EVD, and the many other operational hazards of high priority. For clinical staff there is also a degree of crossover in that acute febrile illnesses, such as malaria or infectious diarrhoea would often require admission to the suspect areas of the EVD TU until EVD was ruled out or another diagnosis was confirmed. Table 1 summarises the main clinical risks and methods used to mitigate.
Clinical risks to personnel deployed on Op GRITROCK
During early planning and risk assessment the absolute risk of EVD cross-infection to the military clinical staff was unknown. When tranche 1 deployed, 10% of HCWs in Sierra Leone were becoming infected with EVD. Based on other NGO infection rates and the mitigation planned to be put in place, it was estimated that the risk to clinical staff deploying was approximately 1% over a 60-day period, but in reality these figures were crude and made at an early planning stage. Predeployment training aimed to improve staff confidence through team building and repeated rehearsals using the new PPE. It was imperative that personnel understood the risks involved, and only performed appropriate tasks with which they were familiar.
Safety of HCWs was considered the first priority, but was balanced against the provision of high levels of clinical care in the EVD TU. Examples include the placement of central venous catheters by experienced doctors only and venipuncture by similarly experienced operators. Furthermore, ceilings of care for patients with EVD were put in place that restricted the use of interventions such as ventilatory support or renal replacement therapy in EVD TU. Although both these capabilities have subsequently been safely delivered in West Africa during the final stages of the outbreak, early risk/benefit analysis, operator safety and the wider public health context of rapidly expanding epidemic excluded their use. For similar reasons patients with EVD were generally considered ‘Not for cardiopulmonary resuscitation’ which was perceived to be high risk to the clinicians, with negligible patient benefit in the absence of any escalation in care.
During scale-up of the facility and during the end of the deployment there were challenges when patient numbers were low, as there was an altruistic desire by many HCWs to do more, but admissions were governed by the medical rules of eligibility. There was a concern about finding an appropriate balance, where there should be a sufficient number of patients to allow skills to be practised, refined and maintained and also ensuring that the facility was not overloaded, leading to an increase in risk of cross-infection. The number of staff deployed to operate the facility safely was based on full capacity, and improved understanding of required staff:patient ratio was gained through experience.
Each tranche was also faced with ‘shockwaves’ as all tranches experienced clinical staff requiring admission to the EVD TU with symptoms reaching the EVD case definition, in whom EVD needed to be excluded. The introduction of the FilmArray diagnostic capability provided earlier diagnosis of many non-EVD infections, particularly those of the gastrointestinal or respiratory tracts, with the consequence being that the duration of admission was shortened for many patients presenting with non-specific symptoms consistent with early EVD.11 The FilmArray's utility in the KTTU HCWs was repeatedly demonstrated during small outbreaks of infectious gastroenteritis where detecting an alternative diagnosis prevented the admission of an HCW to the red zone for further assessment.
Wearing PPE in the tropical climate was neither a risk-free nor comfortable activity and HCWs became rapidly exhausted and dehydrated as well as there being a risk of heat illness, including heat stroke and syncope. Furthermore, limited visibility and dexterity was a side effect of wearing the PPE itself. Minimising the duration in PPE and ensuring safe donning and doffing procedures was, therefore, key to preventing errors and medical emergencies in HCWs. A buddy–buddy system was used at the donning stage with a third person double-checking the PPE was being worn correctly before HCWs entered the facility. While in the facility, HCWs continued to work under the close observation of their buddy in order to identify early high risk events, such as gross contamination with body fluids. On exit, when HCWs were often tired, designated PPE monitors talked the HCWs who remained in their buddy pairs, through the safe removal of PPE in a formalised and stepwise manner in order to minimise human error. At the outset of the operational tour clinical notes were maintained within the facility and electronically transferred to the ward office computers using wireless Bluetooth capability. This process prolonged the duration HCWs were wearing their PPE and risked the rushed completion of notes. A decision was, therefore, made to keep clinical notes outside the facility and transfer information, such as physical examination findings, to an HCW outside the red zone for incorporation into the written record later.
A perception from other EVD TUs was that the risk of cross-infection increased after working in the red zone continually for greater than 2 months, so a decision was made to limit the working period of clinicians to 60 days in the KTTU. This required further tranches of clinicians to be trained and deployed and this was made easier by reinforcements provided by the Canadian Armed Forces. A series of combined training programmes were designed to build teamwork and align knowledge and use of the SOPs and clinical bundle, a returning clinician and a member of the command team oversaw the training of each subsequent tranche. Maintaining clinical continuity was considered important and this was provided by a clinician from each tranche remaining for a few weeks, but not entering the red zone unless considered essential, in order to assist with the transition of a new group of HCWs. Continuity of the command chain, and thereby governance, was enabled by not rotating these personnel until the fourth tranche when an adequate overlap period was built in to enable an effective handover.
Despite all reasonable precautions serious adverse events relating to EVD did occur. There were two needlestick injuries in close succession, with affected personnel requiring evacuation to the Royal Free Hospital in London. Review of these episodes changed how sharps were accounted for within the facility and no further similar events occurred. The most significant event was when a member of the KTTU nursing staff became infected with EVD and aeromedical evacuation back to the UK was arranged for her and colleagues in whom she had been in close contact.10 A case review of the events leading up to this case could find no obvious problem with her PPE use, but as a precaution the duration an HCW could remain in the red zone was reduced to 90 min. Anticipation of these scenarios enabled provisional plans to be enacted and these aeromedical evacuations were smooth and uneventful. Despite this, these events presented challenges to both command and clinical staff in managing their own fears and those of their colleagues.
Robust reporting of accidents and potentially hazardous incidents and regular reviews of these at clinical governance meetings produced a feedback mechanism whereby the working practices within the KTTU were frequently adjusted throughout the operational tour. The development of SOPs for all aspects of command, assurance, clinical care, clinical governance, logistics and training and the development of the clinical care bundle, standardised the activity of individuals within the facility. This improved clinical care and reduced the time spent by HCWs in PPE. An inspection of the facility by the WHO assessed the KTTU at 100% in all clinical governance indicators—the first unit to ever achieve this and re-enforced the comprehensive approach to infection, prevention and control and the delivery of high standards of patient care.
Conclusion
The deployment of a military EVD TU on Op GRITROCK provided an unique opportunity to highlight the ability of the DMS to deploy a Field Hospital ready adapt to new challenges and provide care to a different patient population at short notice. For the staff involved it was a physically and psychologically demanding tour with obvious challenges and risks. This article summarises how the role of the Vanguard Hospital was adapted to the unique operational environment experienced on Op GRITROCK and details the processes required to ensure the hospital functioned effectively. Like any new deployment, there were always going to imperfections in the plan prior to deployment, but these were clearly outweighed by the successes achieved. Most important among these was the provision of excellent clinical care, validated through the WHO inspection; few episodes of accidental injury or other infectious disease, including malaria; no significant heat illnesses and a far lower than expected EVD infection rate among HCWs. The experience of the military EVD TU is one where robust command and clinical structures and systems, overlying a dominant culture of continuous improvement, led to a highly favourable outcome. There are few operational tours where everyone that deployed returned home safely, but on Op GRITROCK this is what happened, while the primary aim of reassurance was also achieved.
Acknowledgments
All those personnel deployed both on and in support of OP GRITROCK. Particular mention to the key role played by the Army Medical Services Training Centre, Strensall. To the bravery of the national and international HCWs who responded to the outbreak and that we were privileged to care for at KTTU.
References
Footnotes
Contributors LEML, ATC, TF and ALM have contributed to the planning, conduct and reporting of the work in this article. LEML has been responsible for the overall content of the work submitted.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.