Article Text

Abstract
Background Trauma patients requiring massive blood transfusion (MBT) have high morbidity and mortality: early and aggressive use of blood products during immediate resuscitation may improve survival. There is currently a lack of evidence to guide initial identification of these patients which is especially important in areas where plasma may need to be thawed. In the absence of this evidence, this study aimed to robustly evaluate expert opinion by using a Delphi process to identify predictors of massive transfusion. This process can be used to ensure that decision rules include variables that have clinical validity, which may improve translation of rules into clinical practice.
Methods An international panel of 35 experts was identified through expert advice against specific criteria. Military and civilian experts from the fields of emergency medicine, critical care, anaesthesia, prehospital care, haematology and general/trauma surgery were included. The Delphi Study was carried out over three rounds. Consensus level was predefined at 80%.
Results 195 statements were generated by the panel of which 97 (49.7%) achieved consensus at the 80% level by the end of round 3. Strikingly no clinical observations reached consensus individually. Metabolic acidosis of a base excess of −5.0 or worse, lactate >5 mmol/L and a low haematocrit on arrival were all considered predictive. Some patterns of injury, but few mechanisms of injury, were considered highly predictive of the need of MBT.
Conclusions This Delphi process has produced a list of parameters that expert clinicians felt were predictive for MBT. This list can be used to inform the generation of decision rules. It is of note that many factors used in current decision rules were not valued by clinical experts—this may be a cause for poor uptake of those rules.
- Massive Transfusion
- Trauma
- coagulopathy
- Shock
- Haemorrhage
- Decision Rules
Statistics from Altmetric.com
Key messages
Experts in resuscitation agree on many parameters which are predictive for massive blood transfusion.
Experts put little weight on abnormalities in routinely acquired clinical observation parameters when predicting massive blood transfusion.
Experts in resuscitation feel medical tests such as lactate are more predictive than any clinical observation parameter when considered in isolation.
There is preference among experts that multiple clinical factors are used when developing clinical prediction tools.
The use of a Delphi Study may help formulate decision rules by ensuring parameters considered useful by experts are considered.
Introduction
Worldwide, injuries are the leading cause of death among those aged 5–44 years.1 Exsanguinating haemorrhage is the sole cause of death in 39% of trauma deaths in civilian trauma,2 and is the leading cause of potentially avoidable death on the battlefield.3
Coagulopathy starts early in the severely injured patient, often before the patient arrives at the emergency department and before significant amounts of fluid have been given.4 ,5 It's presence is associated with worsened outcome,6 as those with coagulopathy are four times more likely to die.7 Patients that require a large blood transfusion have high morbidity and mortality. Stanworth et al found no threshold at which outcomes become worse,8 with a mortality of 22% in those receiving 6–9 units and 42% in those receiving ≥10 units in 24 hours. To try and mitigate trauma coagulopathy, current practice, based on limited evidence, is to give high ratios of fresh frozen plasma to those patients who require high volume transfusions.9
Predicting which patients will require large volume blood transfusion (and hence higher than traditional ratios of FFP) can be clinically challenging. Clinical decision rules exist to predict the likelihood of requiring a massive blood transfusion (MBT) in both civilian10–14 and military15 ,16 trauma, but none of them use a consensus on the practitioner's view of which clinical parameters are useful as their starting point. Clinical acceptability is one of the known barriers for implementation of research17 and ensuring that decision rules use criteria valued by clinicians may improve acceptance of any rules that are developed in the future.
This study sought to establish consensus among experts in the field of resuscitation of major trauma patients about the predictors of MBT.
Methods
A three-round Delphi Study between February 2010 and February 2012 was used to determine which factors were deemed by subject matter experts to be highly predictive of the need for MBT. Expertise was defined as expert knowledge of the resuscitation or transfusion of trauma patients in hospital, prehospital or in a military environment. To demonstrate expertise one or more of the following criteria had to be fulfilled: an active researcher in trauma resuscitation, or a lead clinical role in a centre treating a high volume of trauma or military personnel who had treated high volumes of trauma in the deployed setting. Ongoing clinical exposure was required. Advice on appropriate panel members was received from the serving UK defence consultant advisor in emergency medicine and from one of the authors (KCM-J), the editor-in-chief of the Emergency Medicine Journal at the time of the study. Military and civilian stakeholders from the fields of emergency medicine, critical care, anaesthesia, prehospital care, haematology, general surgery and trauma surgery were identified. All military panel members (less haematologists) had done a minimum of one tour of Afghanistan or Iraq. The panel was multinational.
Round 1
In round 1 of the Delphi Study, the panel members were asked to state what aspects of the history, mechanism, vital signs, examination, investigations and premorbid conditions they felt were predictive of MBT in major trauma patients. They were also asked to express any general views about decision rules. These comments were thematically arranged and turned into the statements that formed round 2.
Round 2
In round 2 the list of statements derived from round 1 were grouped into themes, tabulated and returned to all panel members. The panel were then required to use a Likert Scale (range 1–7)18 to demonstrate their level of agreement or disagreement with each statement with 1 being complete disagreement and 7 being strong agreement. An ‘insufficient knowledge to comment’ option was included for each statement and, if this was selected, the expert was not included in the analysis of that particular statement. All scores 1–3 were counted as disagreement and all scores 5–7 were counted as agreement with a statement. Consensus was calculated by dividing the number of valid responses that agreed or disagreed with a statement by the total number of valid responses for that statement. The panel members were also given the opportunity to make additional comments about each of the statements.
Round 3
Those statements that did not reach consensus in round 2 were reiterated in round 3. Panel members were presented with the statements again; this time they were also shown their round 2 responses and the panel's median response for each statement. They were able to confirm their previous opinion or change it in the light of the median view of the panel. There was a further opportunity to comment on each statement.
Consensus definition
Statements were deemed to meet consensus if 80% of the experts either agreed5–7 or disagreed1–3 with the statement. Where an expert had stated ‘insufficient knowledge’ for a particular statement they were excluded from analysis for that statement.
Statistical analysis
Data were analysed using Microsoft Excel 2000 and SPSS V.19. The frequencies, median, IQR and percentage agreement for each statement were calculated.
Ethical approval
The Chair of the Central Manchester Research Ethics Committee deemed that this Delphi Study did not require formal ethical approval (note on file).
Results
Delphi panel
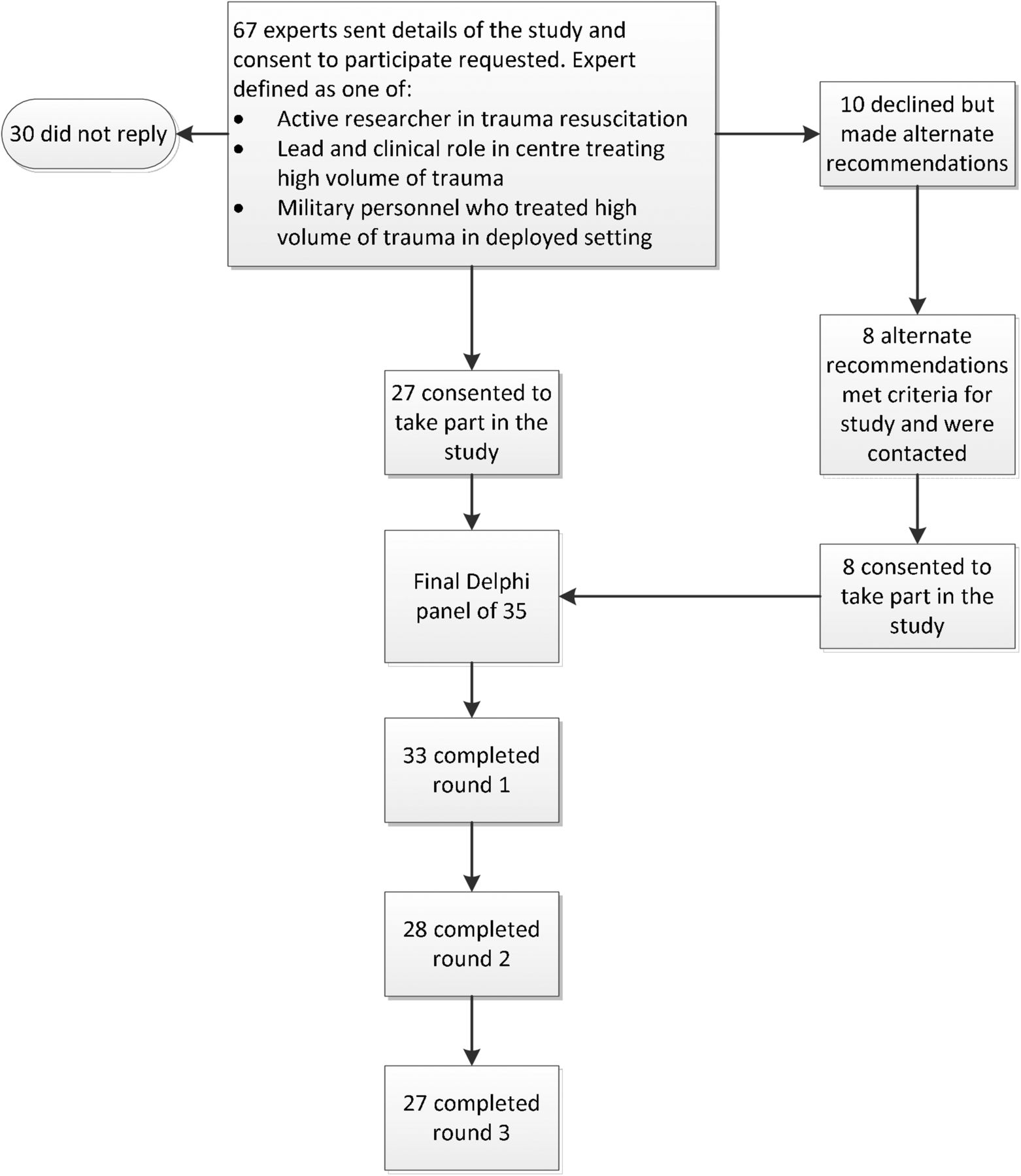
Sixty-seven experts were contacted, of whom 10 declined to take part and 30 did not respond. The main reason given for turning down panel membership was the time required to take part in the study. Alternate and additional suggestions of experts were made by some of those contacted, resulting in the final panel number of 35 of which 13 were regular serving UK military personnel and 11 were from outside the UK. All panel members had clinical roles at the time of the study. The final expert Delphi panel is shown in online supplementary appendix 1. The Delphi panel flow chart is shown in Figure 1.
{kind=link}
Participation flow chart.
supplementary appendices
Delphi results
Thirty-three panel members (94%) completed round 1, while 28 (80%) and 27 (77%) completed rounds 2 and 3, respectively. Deployed military personnel were not able to respond to some rounds due to problems accessing the online resource. Rounds 2 and 3 were lengthy and some panel members were unable to continue to contribute sufficient time to complete the final rounds. Round 1 responses were formulated into 195 statements; 43 (22%) of these achieved 80% consensus in round 2; the remaining 152 statements made up round 3 where a further 54 (28% of the original 195) achieved 80% consensus. In total, 97 statements (49.7%) achieved consensus at the 80% level (of which 12 (6%) achieved negative consensus)—98 statements (50.3%) did not reach consensus.
Those statements reaching consensus are shown thematically in Boxes 1⇓⇓⇓⇓–6 and the full list of statements with the level of agreement achieved is available as online supplementary material.
Statements reaching consensus for mechanism of injury
Statements reaching positive consensus
High energy transfer versus the patient is highly predictive of the need for MBT.
A pressure plate IED or other blast exposure is highly predictive of the need for MBT.
An IED on a foot patrol is highly predictive of the need for MBT.
An IED on vehicles with unrestrained occupants blown clear is highly predictive of the need for MBT.
Multiple gunshots to trunk/torso are highly predictive of the need for MBT.
Gunshot wound into neck/groin/axilla is highly predictive of the need for MBT.
Major crush injury to the torso is highly predictive of the need for MBT.
Major blunt trauma chest/abdomen/pelvis and proximal long bone is highly predictive of the need for MBT.
Mechanism without evidence of injury or altered physiology on arrival in the ED is a poor indicator of severe injury or need for MBT.
No statement in this section achieved negative consensus.
ED, emergency department; IED, improvised explosive device; MBT, massive blood transfusion;
Statements reaching consensus for clinical observations and response to treatment
Statements reaching positive consensus
Absence of radial and femoral pulses is highly predictive of the need for massive blood transfusion (MBT).
Trends in pulse rate, BP, RR, and GCS are more predictive than a single measurement in predicting the need for MBT.
Tachycardia and hypotension on presentation to emergency medical services is highly predictive of the need for MBT.
Hypotension not responsive to small-volume fluid resuscitation is highly predictive of the need for MBT.
Hypotension after exclusion of tension pneumothorax or tamponade is highly predictive of the need for MBT.
A clinically hypoperfused casualty with an appropriate mechanism of injury is highly predictive of the need for MBT.
Hypotension and signs of trauma consistent with massive blood loss (eg, massive haemothorax) is highly predictive of the need for MBT.
ATLS grade 4 shock is highly predictive of the need for MBT.
Being moribund/periarrest on arrival is highly predictive of the need for MBT.
PEA (post trauma) on arrival or in ED is highly predictive of the need for MBT.
Cardiac arrest with ROSC is highly predictive of the need for MBT.
Hypotension on scene with extensive visible blood loss is highly predictive of the need for MBT.
The presence of ongoing visible blood loss (eg, frank loss or via invasive tubes) is highly predictive of the need for MBT.
If there is no response to fluid boluses in the shocked patient then MBT is much more likely.
Lack of response to IV fluids (eg, still very hypotensive after 2 l of crystalloid) is appropriate criteria to start MBT.
No response to initial volume therapy despite appropriate haemorrhage control makes MBT much more likely.
Failure to raise SBP to greater than 100 mm Hg with initial 2 units of blood makes MBT much more likely.
Continuing problems with maintaining BP throughout damage control surgery and resuscitation make MBT much more likely.
If spinal injury is clinically excluded (ie, moves all limbs) and the patient is unstable cardiovascularly then MBT is much more likely.
A normal BP in a young adult with identified haemorrhage risk does not exclude massive blood loss.
A patient who looks well perfused is unlikely to need a MBT.
If a patient is still stable on arrival following a long prehospital time, they are unlikely to require MBT.
Statements reaching negative consensus (disagreed with the statement)
A high BP and slow pulse is highly predictive of the need for MBT.
Appearing pale is highly predictive of the need for MBT.
Confusion is highly predictive of the need for MBT.
Immediate loss of consciousness is highly predictive of the need for MBT.
If the patient requires immediate intubation upon arrival at hospital, this is highly predictive of the need for MBT.
IV, intravenous; MBT, massive blood transfusion; PEA, pulseless electrical activity; ROSC, return of spontaneous circulation.
Statements reaching consensus for investigations and injuries
Statements reaching positive consensus
In isolation no tests are predictive of MBT.
Thrombocytopenia on first full blood count (FBC) is highly predictive of the need for MBT.
Acute anaemia on arrival with minimal fluid resuscitation is highly predictive of the need for MBT.
Low haematocrit on arrival is highly predictive of the need for MBT.
Metabolic acidosis with a base excess (BE) −5.0 or worse is highly predictive of the need for MBT.
Metabolic acidosis with a BE −6.0 or worse is this is highly predictive of the need for MBT.
Metabolic acidosis with a BE −8 or worse is highly predictive of the need for MBT.
Lactate greater than 5mmol/l is highly predictive of the need for MBT.
Significant and increasing lactic acidosis is highly predictive of the need for MBT.
If the patient has a coagulopathy on any tests this is highly predictive of the need for MBT.
Abnormal clotting on ROTEM/TEG is highly predictive of the need for MBT.
The presence of an underfilled pressure curve on the arterial line tracing is highly predictive of the need for MBT.
Massive haemothorax on chest radiograph is highly predictive of the need for MBT.
A positive focused assessment with sonography in trauma (FAST) and abnormal vital signs is highly predictive of the need for MBT.
Two or more injuries with the potential to bleed significantly found on initial imaging (eg, large haemothorax and positive FAST) is highly predictive of the need for MBT
The presence of a vertical shear fracture on pelvic X-ray is highly predictive of the need for MBT.
The presence of an unstable pelvic ring fracture (tile type B or C) is highly predictive of the need for MBT.
CT findings of contrast blush suggesting ongoing arterial haemorrhage, or significant intrathoracic or intra-abdominal haemorrhage is highly predictive of the need for MBT.
CT findings of retroperitoneal haemorrhage is highly predictive of the need for MBT.
CT confirming major pelvic injury is highly predictive of the need for MBT.
Angiographic evidence of major vascular injury is highly predictive of the need for MBT.
The presence of large amounts of blood on initial placement of a tube thoracostomy (typically greater than 500 mL) or large amount of continuous output from tube thoracostomy is highly predictive of the need for MBT.
Severe injury to more than one body region is highly predictive of the need for MBT.
Injury to more than one body cavity is highly predictive of the need for MBT.
Presence of active non-compressible haemorrhage without signs of shock is highly predictive of the need for MBT.
Presence of active non-compressible haemorrhage with signs of shock is highly predictive of the need for MBT.
Major blunt trauma to the upper abdomen (liver/spleen region) is highly predictive of the need for MBT.
Massive abdominal contusion from blunt trauma is highly predictive of the need for MBT.
Bilateral above knee amputation is highly predictive of the need for MBT.
Multiple amputation (three or four limbs) is highly predictive of the need for MBT.
Pelvic involvement with lower limb amputations is highly predictive of the need for MBT.
Multiple open fractures in blast injuries are highly predictive of the need for MBT.
Clinical pelvic instability is highly predictive of the need for MBT.
Obvious open pelvic injury is highly predictive of the need for MBT.
Severe perineal injury is highly predictive of the need for MBT.
Obvious major vascular injury is highly predictive of the need for MBT.
Statements reaching negative consensus (disagreed with the statement)
Abdominal tenderness is highly predictive of the need for MBT.
Abdominal guarding is highly predictive of the need for MBT.
BE, base excess; FAST, focused assessment with sonography in trauma; FBC, full blood count; MBT, massive blood transfusion; ROTEM, rotational thromboelastometry; TEG, thromboelastography.
Statements reaching consensus for prehospital care received
Statements reaching positive consensus
If multiple limb tourniquets are needed in the prehospital environment, MBT is much more likely.
Statements reaching negative consensus (disagreed with the statement)
Giving prehospital fluids is highly predictive of the need for MBT.
If a limb splint has been applied prehospital, this is highly predictive of the need for MBT.
MBT, massive blood transfusion.
Statements reaching consensus for premorbid condition
Statements reaching positive consensus
Patients on anticoagulant therapy are much more likely to need MBT.
Patients with cirrhosis are much more likely to need MBT.
Patients with any pre-existing coagulopathy—eg, haemophilia, liver disease are much more likely to need MBT.
Statements reaching negative consensus (disagreed with the statement)
Patients with diabetes mellitus are much more likely to need MBT.
MBT, massive blood transfusion.
Statements reaching consensus for other aspects of decision rules
Statements reaching positive consensus
If MBT is clinically indicated, commencement of an MBT policy must not be delayed pending results of investigations.
There are no individual predictors of MBT; a composite picture is required taking multiple factors into account.
General trend and course of patient from time zero (injury) is the best predictor of the need for MBT.
Massive blood loss can be contributed to by clinicians through inappropriate use of large volumes of crystalloid in massive blood loss, leading to increased blood loss due to coagulopathy.
Massive blood loss can be contributed to by clinicians through failure to prevent iatrogenic hypothermia
For junior practitioners, or for any grade practicing where major trauma cases requiring MBT are seen infrequently, a decision rule would be helpful.
Decision rules are helpful in that they force early confrontation of the form of resuscitation and the pattern of monitoring.
A decision rule would be useful as it would lead to earlier activation of an MBT protocol and therefore improved product availability.
There is a danger, if a MBT protocol is not instituted early, that inappropriately low volumes of FFP and platelets are given as it is not recognised that they are needed until large volumes of packed red blood cells have been given.
A decision rule to rule out the likely need for MBT would be useful as this may prevent overuse of blood products.
A decision rule would be a useful risk reduction tool.
Guidelines are preferable to rules in this situation—rules may be followed slavishly and cause delay when consulted if not known by heart. Guidance is less proscriptive.
Guidance would be helpful on when to start prehospital blood transfusion where available.
A decision rule which gives a course of action (ie, start MBT protocol) rather than a percentage risk of the need of MBT would be more useful.
Statements reaching negative consensus (disagreed with the statement)
To be appropriately specific, the point at which MBT is ruled in would need to have a 50% chance of requiring a MBT.
To be appropriately specific, the point at which MBT is ruled in would need to have a 60% chance of requiring a MBT.
MBT, massive blood transfusion.
Mechanism of injury
The mechanisms of injury that were felt to be predictive of MBT are shown in Box 1.
The notable finding is that few mechanisms were felt to be predictive on their own; only exposure to an improvised explosive device, mine or multiple gunshot wounds (GSW) to the trunk, single GSW to neck, axilla or groin, or major crush injury to the torso were considered predictive. High energy transfer to the patient can occur in all of these mechanisms, and the panel agreed that this is predictive. Single GSW to the trunk even from a high velocity weapon did not reach consensus. Roll-over, entrapment, pedestrian versus car or fall from a height of greater than 3 m also failed to reach consensus.
Clinical observations and response to treatment
The clinical observations that were felt to be predictive for MBT are shown in Box 2.
Agreement about specific clinical values was not achieved for any single observation parameter. Pulse rate of greater than 130, RR of >40, systolic BP (SBP) of less than 80 mm Hg or a prolonged capillary refill time did not reach consensus. The only physiological parameter that approached consensus was an SBP of less than 80 mm Hg; 78% of the panel felt this was highly predictive. Absence of a radial and femoral pulse was considered significant but thready or weak pulses, even centrally, were not. The panel felt that signs of hypoperfusion linked with exclusion of other factors that cause shock (tension pneumothorax, tamponade or spinal shock), or associated with an appropriate mechanism of injury were predictive of MBT. Trends in observations were also considered predictive along with multiple abnormal observation parameters taken together in the ATLS classification of class 4 shock.
Investigations and injuries
The investigations and injuries that were felt to be predictive for MBT are shown in Box 3.
Acute anaemia, thrombocytopenia, a base excess of −5 or less, and a lactate of 5 mmol/L or more were all agreed as predictive of MBT. Although the panel agreed that any clotting abnormality was predictive for MBT, international normalised ratio of 1.5 or more or prothrombin time greater than 15 s individually were not agreed as being predictive.
Several groups of specific injuries were agreed by the panel as being highly predictive and investigations confirming particular injury patterns such as unstable pelvic ring fractures or massive haemothorax were re-enforced as being predictive. Evidence of blood loss on CT, or on focused assessment with sonography in trauma scanning (if abnormal vital signs were present) especially when more than one location of blood loss was found were also agreed as predictive. The presence of bilateral below knee amputations did not reach agreement although bilateral above knee amputations and triple limb amputation did. Pelvic involvement with lower limb amputation was also considered significant. Abdominal pain and guarding were agreed as not being predictive, although major blunt trauma, crush injury and massive contusion to the abdomen all achieved consensus as predictive.
Prehospital care
Few prehospital interventions reached agreement as being predictive of the need for MBT; these are shown in Box 4.
The need for a tourniquet was considered predictive; however the use of haemostatic agents was not. The administration of prehospital fluids was not felt to be predictive.
Premorbid condition
Those premorbid conditions felt to be predictive of MBT are shown in Box 5.
The only premorbid conditions felt to make MBT more likely were those factors that significantly influenced clotting. The use of anticoagulant therapy, liver cirrhosis or pre-existing clotting abnormalities were all considered predictive.
Other aspects of decision rules
Factors that reached consensus pertaining to decision rules are shown in Box 6.
There was general consensus within the panel that a decision tool to predict the commencement of an MBT protocol would be useful. It was felt that this would be particularly useful for practitioners who were less experienced with patients requiring MBT. Despite the high levels of agreement that a rule would be useful, no agreement was made on the sensitivity or specificity that any rule would require before it was deemed useful.
Discussion
This study has provided the first expert consensus on the predictors of MBT using a Delphi methodology.
Principal findings
Experts take multiple factors into consideration when assessing patients to predict the requirement for MBT. Factors such as mechanism of injury, physiology and the results of investigations are all considered important with an additive effect when more than one factor is affecting the individual patient. When specific injuries or specific mechanism coexist with abnormal physiology, trends in physiology are deteriorating or multiple abnormalities in physiology are present, this is felt to be predictive of MBT.
The weight that is put on individual parameters may be related to how likely it is that factors other than shock can affect that parameter. Individual blood test results showing evidence of hypoperfusion (base excess (BE) of −5.0 or worse, serum lactate of 5 mmol/L or more, or low haematocrit) were considered highly predictive, whereas neither a pulse of greater than 120 bpm nor hypotension with an SBP of less than 80 mm Hg were considered predictive on their own.
This may be due to concerns among the panel about the predictive value of the commonly taught ATLS classifications for diagnosing shock, the validity of which has been challenged,19–21 which may have resulted in clinicians doubting the validity of clinical observations alone. Only 10.9% of ATLS course directors and instructors considered the ATLS classification of hypovolaemic shock as a ‘good guide’ for fluid resuscitation and blood product transfusion in one study.22 Other studies question the usefulness of pulse rate in predicting the need for emergency intervention for haemorrhage in trauma and the association of pulse rate with hypotension.23 ,24 It has also been suggested that a relative bradycardia associated with hypotension after trauma has worse outcomes than tachycardia.25
Evidence does however exist that shows that certain clinical parameters are predictive of MBT. Multiple studies looking at prediction of MBT have looked at the predictive value of BP.10–14 The most commonly used value of SBP for prediction of MBT was less than 90 mm Hg with ORs presented between 2.6 and 20.1 for prediction of MBT at this level. Alternate cut-offs were used by Mclaughlin15 with an SBP of less than 110 mm Hg giving an OR of 3.5 for prediction of MBT in military patients. Furthermore Yucel10 used two cut-off values of less than 100 mm Hg and less than 120 mm Hg with ORs of 3.0 and 1.4, respectively. In all the papers presented that also measured base deficit, the ORs presented were broadly similar for both SBP less than 100 mm Hg and base deficit of 5 or more for prediction of MBT.
The pulse rate, although not as predictive in these studies as SBP or base deficit, had ORs ranging from 1.5 to 7.5 for a pulse of 120 bpm or more.10–12
Overall, absolute evidence of injury known to cause major blood loss, such as the presence of an unstable pelvic fracture, was considered predictive. Open pelvic fractures have been shown to have a high likelihood of requiring MBT in one study,26 although closed but unstable fractures were not found to require MBT in another study, requiring blood transfusion of 4.9 units when unstable versus 2.4 units of packed red blood cell (PRBC) when fractures were stable.27 They would however add significantly to the transfusion requirements in a multiply injured patient. GSWs to the trunk were not thought to be predictive of MBT. Published evidence shows only 14% of patients required theatre following penetrating chest trauma with a mean blood transfusion requirement of 4.5 units of PRBC if caused by GSW and 3.3 if caused by stabbing.28 However the study excluded those requiring emergency thoracotomy and the numbers requiring this were not reported; these patients would likely have higher transfusion requirements.
Limitations of the study
The main limitations of this study are those of the Delphi methodology itself. If statements are insufficiently defined they risk being discounted or being seen as too broad to be useful; similarly, overdefined statements may become so specific they are not generalisable. For example, despite published evidence to the contrary, a pulse of 120 or more was not considered predictive of MBT. Comments made by the panel indicate that a statement such as ‘a pulse of >120 in a major trauma patient once stress/anxiety, tension pneumothorax and cardiac tamponade have been excluded is predictive for MBT’ would be needed before experts were happy to agree with this statement.
Several participants commented that the likelihood that a patient with a GSW to the chest would require an MBT depended on what was hit. This would potentially mean that as well as a statement ‘GSW to the chest with penetration of the heart is predictive of MBT’, the same statement would be required listing all the other organs in the chest individually. This would result in so many statements that the Delphi would have become unmanageable.
Conclusion
This is the first study to define the factors that experts feel are predictive of MBT. Despite the limitations implicit in the Delphi methodology, this study has produced some clear results on what experienced clinicians think is useful to aid decision making in major trauma. There are many barriers to the successful implementation of decision rules in practice.17 A discord between the parameters in the rule and expert clinical opinion is one of these. This study may facilitate the development of future clinical decision rules related to MBT requirement by allowing incorporation, where appropriate, of predictive factors thought to be useful by experienced clinicians. A good understanding of current expert clinical practice will also highlight if any rules vary from this, potentially allowing focused educational instruction during implementation. Of note the lack of agreement on the usefulness of clinical observation parameters suggests concern regarding their utility despite evidence suggesting that they are of value. This requires thought on how these variables are used in decision rules and warrants further education and research.
Acknowledgments
The authors thank the panel members; Lt Col Lynn Adam, Dr John Black, Lt Col Doug Bowley, Prof Karim Brohi, Lt Col Adam Brooks, Prof David Cone, Lt Col Peter Davis, Dr Peter Driscol, Surg Capt Geraint Evans, Dr Peter Goode, Dr Carl Gwinnutt, Dr Timothy Hardcastle, Col Jeremy Henning, Prof John Hess, Brigadier Timothy Hodgetts, Ms Celia Kendrick, Mr Yoram Kluger, Lt Col Simon Le Clerc, Prof David Lockey, Prof Hans—Morton Lossius, Col Peter Mahoney, Prof Michael Millin, Dr Michael Murphy, Dr Cathal O'Donnell, Dr Mike Parr, Sir Keith Porter, Col Sam Rawlinson, Gp Capt Martin Ruth, Surg Captain Jason Smith, Dr Simon Stanworth, Col Nigel Tai, Dr Karl—Christian Thies, Prof Lee Wallis and Dr Andreas Ziegler for their hard work. Their full details are in supplementary data appendix 1.
References
Footnotes
Contributors JVM: main author, ran the Delphi Study, worked with KCM-J to produce the Delphi panel, analysed results, wrote the paper. KCMJ: supervisor of JVM during her MD of which this is part. Helped at all stages in the Delphi Study, provided names for panel, reviewed statements for readability and usefulness, ran the study for a short time during JVM's deployment, edited paper. STH: reviewed the research after the Delphi Study was performed. Gave significant contribution as to how to aim the paper to allow publication with thoughts on what would make the paper most relevant and interesting. Read repeated iterations of the paper and edited final paper. RB: reviewed the research after the Delphi Study was performed. Gave significant contribution as to how to aim the paper to allow publication with thoughts on what would make the paper most relevant and interesting. Read repeated iterations of the paper and edited the final paper.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.