Article Text

Abstract
Introduction Survival in exsanguinating cardiac arrest patients is poor, as is neurological outcome in survivors. Hypothermia has traditionally been seen as harmful to trauma patients and associated with increased mortality; however, there has been speculation that cooling to very low temperatures (≤20°C) could be used to treat haemorrhagic trauma patients by the induction of a suspended animation period through extreme cooling, which improves survival and preserves neurological function. This has been termed emergency preservation and resuscitation (EPR).
Methods A systematic review of the literature was used to examine the evidence base behind the use of deep and profound hypothermia in haemorrhagic shock (HS). It included original research articles (human or animal) with cooling to ≤20°C after HS or an experimental model replicating it. Normovolaemic cardiac arrest, central nervous system injury and non-HS models were excluded.
Results Twenty articles using 456 animal subjects were included, in which 327 were cooled to ≤20°C. All studies describing good survival rates were possible using EPR and 19/20 demonstrated that EPR can preserve neurological function after prolonged periods of circulatory arrest or minimal circulatory flow. This additional period can be used for surgical intervention to arrest haemorrhage in HS that would otherwise be lethal.
Conclusions The outcomes of this review have significant implications for application to human patients and the ongoing human clinical trial (EPR for Cardiac Arrest from Trauma). Current evidence suggests that hypothermia ≤20°C used in the form of EPR could be beneficial to the HS patient.
- Haemorrhagic shock
- Therapeutic hypothermia
- Suspended animation
- Emergency preservation and resuscitation
- Deep hypothermia
- Profound hypothermia
Statistics from Altmetric.com
- Haemorrhagic shock
- Therapeutic hypothermia
- Suspended animation
- Emergency preservation and resuscitation
- Deep hypothermia
- Profound hypothermia
Key messages
Outcome of exsanguination cardiac arrest is poor, with the maximum window for intervention to surgically arrest haemorrhage defined by the time from wounding to exsanguination.
Cooling to ≤20°C successfully extends this window in animal models of haemorrhagic shock, increasing survival rates and preventing neurological damage.
This cooling is not compatible with spontaneous circulation but is a cooled circulatory arrest or low-flow circulation induced by a cold liquid flush.
During the cooled period, surgical haemostasis (potentially of multiple injuries) can be achieved before rewarming and resuscitation using cardiopulmonary bypass.
This has been termed emergency preservation and resuscitation (EPR), and a trial in human victims of penetrating trauma is ongoing.
EPR could have a major role in improving survival in haemorrhagic battlefield casualties with injuries normally irreparable before exsanguination.
Introduction
Trauma is the leading cause of death during the first four decades of life in westernised countries,1 with haemorrhage accounting for >50% of deaths in the 48 hours post injury.2 In 2007, the outcomes of cardiac arrest (CA) resulting from exsanguination following trauma were described as ‘dismal’.3 In trauma, hypothermia is well documented as being associated with mortality4 ,5 and a number of mechanisms for this have been proposed (Table 1).6 Despite this, there has been debate about the role of hypothermia during haemorrhagic shock (HS), with the suggestion that it could actually form part of a new method of initial trauma treatment, one that could improve neurological outcomes in particular.7 ,8
Pathophysiological processes caused by hypothermia6
A basic definition of hypothermia is a core body temperature (CBT) <35°C, although different classifications are used in trauma and non-trauma contexts (Table 2),6 and alongside acidosis and coagulopathy forms the ‘lethal triad’—these components work synergistically to exacerbate haemorhage,9 which eventually leads to exsanguination CA, with the brain ischaemic insult time being around 5 min at normal CBT.10 During HS, hypothermia likely occurs most significantly due to energy depletion11—the reduced oxygen delivery to tissues causes a switch from oxidative-phosphorylation to substrate-level phosphorylation and a drop in heat production and CBT.12 ,13 This hypothermia can be viewed as a by-product of HS and has been termed ‘shock-induced hypothermia’ (SIH), distinct from the hypothermia occurring as a result of cooling while tissues are adequately oxygenated, which has been termed ‘therapeutic hypothermia’ (TH).8 Failure to recognise the difference between TH and SIH could limit the translation of hypothermia into trauma care.8
Definitions of grade of hypothermia6
Hypothermia may have beneficial effects in HS. Mild TH decreases muscle metabolism13 and cerebral metabolism is reduced by 6–8% per 1°C drop in CBT,14 thereby reducing oxygen demand during HS. It remains unclear if either the protective or harmful effects seen in mild hypothermia are seen during extreme cooling. There has been increased interest in the concept of rapidly inducing deep or profound hypothermia (≤20°C) to extend ischaemic time in severely injured patients in HS as a form of ‘suspended animation’.8 ,11 This is not compatible with spontaneous circulation and therefore requires subsequent resuscitation, giving rise to the term ‘emergency preservation and resuscitation’ (EPR).15 Tisherman reports that the damage found in battle casualties with penetrating truncal injuries is often technically repairable, although not in a timeframe compatible with life16—EPR may provide an opportunity for such repair.
To answer the question whether deep and profound hypothermia in haemorrhagic trauma is beneficial or not, a systematic review of the current literature on the use of cooling to ≤20°C in HS was performed.
Method
In November 2016, searches of Medline using both PubMed and Ovid were performed using the terms ‘hypothermia shock’, ‘hypothermia coagulopathy’, ‘therapeutic hypothermia trauma’ and ‘emergency preservation and resuscitation’ with no filters applied which yielded 1721, 756, 2862 and 94 results, respectively. A further Ovid search using the terms ‘emergency preservation and resuscitation’, ‘hypothermia trauma’ and finally the term ‘therapeutic hypothermia’ AND ‘trauma’ yielded 59, 192 and 1091 results. It was likely that the number of relevant articles would be small so the search criteria were kept deliberately wide to ensure all articles were identified. A manual search of the reference lists of several key articles identified further literature; once duplicate articles were removed, 5571 records remained. The remaining article titles and abstracts were screened to identify those that met the inclusion criteria which were:
Original human or animal research articles.
Subject temperature of ≤20°C. Studies using controls or comparisons at other temperatures were included if they included a group ≤20°C.
Subjects must be in HS or have experimental replication of HS in at least one of the research groups.
Research examining CA following exsanguination (or a model of it).
English-language, French-language or Italian-language articles.
Exclusion criteria were research of normovolaemic CA, central nervous system injury, burns and other non-HS studies and foreign-language articles other than those described.
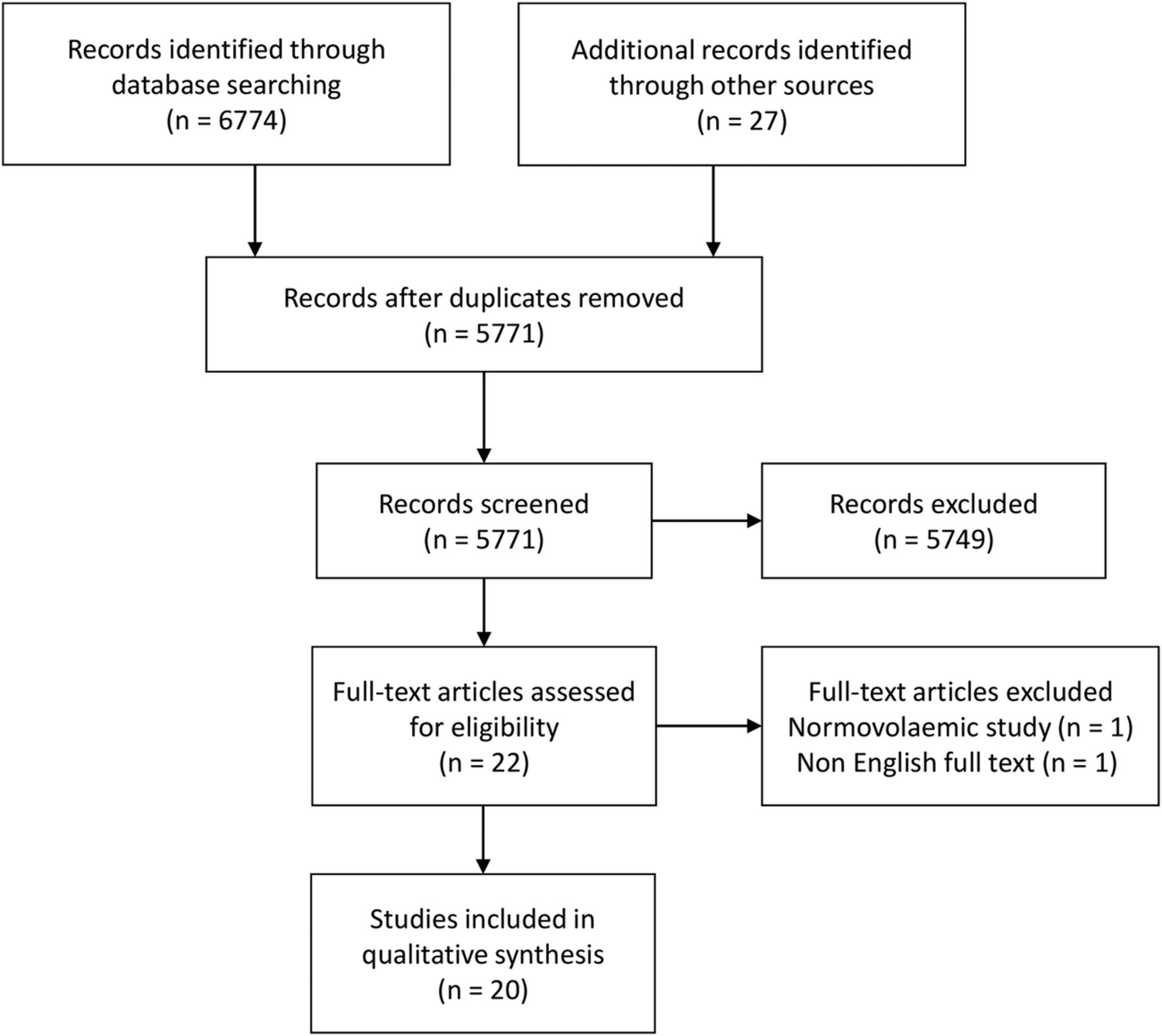
Based on title and abstract, 22 potentially suitable original articles were identified; full-text review excluded two—one assessed the correct depth of hypothermia but in a normovolaemic CA model and the other was a Chinese-language article (Figure 1).

{kind=link}
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram showing search method and results.
Results
Study methodology
Twenty original research articles met the inclusion criteria,3 ,15 ,17–34 none of which were a human study. Nine used a pig model,20 ,21 ,24–29 ,33 seven a canine model15 ,17–19 ,22 ,23 ,32 and four used a rat model,3 ,30 ,31 ,34 totalling 456 animal subjects (188 pigs, 174 dogs and 94 rats). Overall, 38 subjects were sacrificed in equipment and protocol familiarisation,20 ,23 ,25 ,27 5 were used as blood donors23 and 10 excluded from the study results for other reasons;17 ,25 ,31 76 animals were used as normothermic controls/shams3 ,15 ,17 ,19 ,24 ,28 ,31 ,34 and these, along with 327 animals exposed to cooling3 ,15 ,17–34 to various temperatures <20°C, were used to produce the study results. Of the 327 cooled subjects, all but two controls underwent HS before cooling.17 All 20 studies3 ,15 ,17–34 reported on survival and 19 reported neurological outcomes3 ,15 ,17–33 alongside other outcomes according to study; postintervention observation ranged from 3 hours34 to 6 weeks,20 ,21 ,24 ,28 ,29 with the exception of one subject that was observed for 4 months.17
Initial evidence for EPR
In 1990, Tisherman et al demonstrated that return of spontaneous circulation (ROSC) could be achieved after 30 min of HS (mean arterial pressure (MAP) of 40 mm Hg) and up to 120 min of circulatory arrest (CirA) at a tympanic membrane temperature (TMT) of 15°C in a dog model. Three groups of five subjects were tested with 60, 90 and 120 min of cooled CirA. Bleeding and cooling (via a cold flush) was achieved through pre-inserted cardiopulmonary bypass (CPB) cannulas. All had ROSC and survived to 72 hours; the mean neurological deficit scores (NDS) (Table 3) were 0%, 10% and 27% (p<0.05), respectively. All of the 60 min group, 60% of the 90 min group and 20% of the 120 min group scored one on overall performance category (OPC) assessment (Table 3); the other 40% of the 90 min group scored OPC 2.17 This is the first example of the use of EPR in an HS model.
Overall performance categories and neurological deficit scores17
Optimum temperature for EPR
Following on from the original study,17 various studies have shown that cooling to 10°C offers the best survival rates and the best neurological outcomes. Improved NDS and OPC scores after 120 min of cooler CirA (post-30 min HS) were found in one study where canine subjects were cooled to a TMT of 15°C (n=10) or 10°C (n=12). After 120 min, subjects were rewarmed and resuscitated via CPB before a period of intensive care running to the end of the experiment at 72 hours. Two subjects were excluded for breached experiment protocol—ROSC was possible in all remaining subjects. Final NDS scores were non-significantly better in the 10°C cooling group compared with the 15°C cooling group, with a further trend towards a better outcome in the 10°C cooling group, where 90% of subjects had outcomes of OPC 1 and 2 versus 50% in the 15°C group.18
EPR at 10°C has been further demonstrated to provide optimal outcomes in dogs by Behringer et al. Three groups were cooled to 10°C (n=3), 15°C (n=5) and 20°C (n=6) before 60 min CirA with two additional group cooled to 10°C before 90 (n=6) or 120 (n=7) min CirA. Animals cooled to 10°C for 90 min and all 60 min subjects (all temperatures) survived the full 72 hours. All the subjects in the groups cooled to 10°C for 60 and 90 min had OPC and NDS scores of 1 and 0%, respectively—these were the best results, with the remaining groups having NDS and OPC scores of 0–27% and 1–3.22
Experimentally, cooling to 10°C appears to be the optimum temperature with cooling below this temperature providing worse outcomes as demonstrated by a 2006 study by Alam et al28 that investigated the optimum depth of cooling in a pig HS model. Four groups of eight were used: a normothermic group and groups cooled to 15°C, 10°C and 5°C; after 30 min of HS induced via iliac vessel and later aortic injury, 60 min of cooling to the target temperatures was initiated before rewarming and resuscitation. The normothermic group were all brain dead after rewarming/resuscitation, four of the 5°C group survived to the immediate postintervention stage, with three dying over the following 12 days—only one of this group survived to the 6-week point and was cognitively impaired. The 10°C group had the best outcome; only one subject died and all survivors were neurologically intact, having the same learning ability as normal pig. The difference in survival between the 5°C and 10°C groups was statistically significant. The 15°C group had similar neurological outcome as the 10°C group but survival was reduced (5 vs 7 out of 8)—EPR at 10°C produces the best survival rate in pig and hence may be the best temperature target during human EPR trials.
Duration of EPR
Alam et al suggest that the EPR cooling period should be kept as short as possible, with the maximum duration (allowing good survival rates in pig) being 60 min. In a pig model, CPB was used to induce 10°C circulatory low flow after 30 min of HS from iliac vessel incision, before 5 min of haemorrhage from an aortic incision. Subjects were cooled to 10°C for 60 or 120 min and injuries were surgically repaired during this period. Four-week survival was 92% in the 60 min group versus 50% in the 120 min group. The difference was statistically significant. Arrhythmias and acute cardiac failure accounted for four of the deaths in the 120 min group and one of the deaths in the 60 min group during the first 24 hours. Statistically significant delays in return to full walking were seen in the 120 min group (7.2 days vs 2.2 days); however, none of the subjects had any histological brain damage.33 The need to keep the EPR period short is further supported by research using a rat model in which 75 min of 15°C no-flow EPR (post-HS and CA) was associated with a statistically significant eightfold increase in mortality and worse neurological outcomes versus 60 min of 15°C no-flow EPR.31 However, there may be effective ways to safely extend the EPR period which would have obvious benefits in terms of allowing greater time for intervention.
There is variation in the duration of EPR that can be tolerated in different species. Drabek et al demonstrated that in a rat model EPR (at 15°C) for a period of 60 min provided good outcomes, while 75 min it did not. All of the subjects in a 60 min EPR group survived to the end of the experiment (3 days) compared with only two of seven in a 75 min EPR group.3 This survival rate is a lot lower than that demonstrated in dogs at the same temperature but for 120 min of cooling;18 however, the variation in results could be due to the considerable variation in study methodology. Potential interspecies differences between humans and animals may make it difficult to extrapolate findings from rat or dog models into human research. Optimum duration for EPR may be different in humans and it might also be the case that neurological damage is more obvious in higher functioning species that would not be identified using OPC and NDS tools in rodent and canine models.
Additional factors influencing outcome in EPR
In addition to depth of cooling, the rate at which EPR is induced also influences outcome. In a pig model of HS, fast cooling (FC) at a rate of 2°C/min was superior to medium cooling (MC) or slow cooling (SC) at 1 and 0.5°C/min, respectively. FC achieved 87.5% 6-week survival compared with 62.5% with the MC rate and 37.5% with the SC rate. No neurological deficit was observed in survivors, nor was there any histological brain damage.24
Better outcomes are achievable with EPR if subjects have a higher MAP in the HS period before the EPR cooling period.19 Survival rates are significantly higher in canine subjects that have a MAP of 40 mm Hg during 60 min of HS compared with subjects with a MAP of 30 mm Hg for 60 min of HS when resuscitated immediately post HS (without cooling) or when resuscitated after an additional 60 min of EPR. Sixty minutes of full CirA at a TMT of 15°C (following 60 min of HS at a MAP of 30 or 40 mm Hg) does not cause additional mortality or clinically significant neurological damage versus normothermic fluid resuscitation administered immediately after the 60 min of HS at either MAP (demonstrating that EPR provides additional time without risking increased mortality or neurological damage).19 This also suggests that optimisation of patients prior to induction of EPR could maximise survival rates and requires further investigation.
Novel strategies, such as optimisation of cooling fluid/flush, may be needed to successfully extend the EPR period. The addition of oxygen, and/or glucose, to the EPR-induction flush may increase the EPR time after which good neurological function can be achieved. The addition of oxygen to cooling flushes in a canine model of HS successfully extended the EPR period at which good neurological outcomes were achieved to 3 hours of no-flow (at 10°C). Unfortunately there was insufficient statistical power to draw firm conclusions about the results, particularly about the addition of glucose alongside oxygen in the flush.32 Optimum cooling speed, flush composition and physiological conditions prior to induction of EPR are all areas that warrant further research in order to produce the best possible outcomes.
Post-EPR memory and learning
Memory and learning are not adversely affected by post-HS EPR in pig. In part 1 of a two-part study, four subjects already trained in a food-retrieval task underwent simulated HS, achieved by an incision into the aorta (post-thoracotomy). EPR consisted of 60 min of low-flow CPB at 10°C. Three survived and retained the ability to carry out the task 2 weeks later. Five untrained subjects underwent the same procedure and the four survivors were able to learn and carry out the task as well as 15 non-HS controls. In part 2, subjects were divided between three groups (five per group) which underwent 15, 30 or 60 min of HS induced by iliac vessel incisions, followed by 2 min additional haemorrhage through an aortic incision. All subjects were treated with EPR as before and injuries repaired. Survival for the 15, 30 and 60 min HS groups was 80%, 60% and 80%, respectively. Three of the four survivors in the 60 min group took longer to learn the task than controls but 2 weeks later had better task scores. Notably, the authors commented that the surgical repair of injured vessels during this study was easier due to the cooling fluid in the vessels being clear and because of the low-flow state.21
Biochemical changes in EPR
There is evidence that inflammatory response modulation by hypothermia may underpin some of its protective effects. Analysis of blood samples for levels of IL-1β, IL-6, IL-10, tumour necrosis factor-α, tumour growth factor -1β and heat shock protein-70 at various stages of EPR show that hypothermia reduces pro-inflammatory IL-6 expression and increases anti-inflammatory IL-10 expression. Hypothermia also increases protective heat shock responses. Immunological changes are confined to the early postinjury phase, which the authors who carried out this research concluded did not reduce the effectiveness of the subjects' immune response against infection, although it is worth noting that during this study there were two deaths due to sepsis.26
The development of a rodent model of HS and EPR has permitted further study of the molecular mechanisms involved in EPR, using the wider range of molecular tools available for use in rodents and through the increased cost effectiveness of using a small animal model.30 Poorer neurological outcomes seen in rodents after prolonged EPR of 75 min versus medium duration EPR of 60 min may be partially explained by the nitration of proteins and poly (ADP-ribose) polymerase (PARP) (a DNA repair enzyme) activation within the brain. Increased protein nitration and PARP activation within the hippocampus, cortex and striatum is seen after 75 min of EPR but not after 60 min of EPR, and Han et al argued that this could constitute a target for adjunctive therapies. However, a number of confounders, namely variation in EPR induction flow rate, may have contributed to these findings.31
EPR alters gene transcription and creates a pro-survival profile in terms of inflammation, stress response and apoptosis. In a rat model of HS and 60 min of low-flow EPR at 15°C, 571/23 000 genes analysed saw a statistically significant twofold or greater increase or decrease in expression compared with normothermic controls.34 Gene groups in which there was increased expression were those involved with apoptosis regulation and there was an increase in levels of their corresponding proteins. Gene groups that were downregulated were involved in regulation of metabolic pathways, such as bile acid conjugation, lipid metabolism and gluconeogenesis. Hypothermic subjects actually had a relatively high blood glucose, likely due to hypothermia-induced reduction in insulin secretion and sensitivity.
Portable EPR equipment
Two of the studies we identified were tests of a prototype low-cost compact CPB pump25 ,27 as small low-cost CPB devices would be necessary to facilitate EPR in forward role facilities or austere environments. The first tested this pump's effectiveness in cooling pig in HS to 10°C, with 5/6 subjects successfully completing the experimental protocol through to the final 3-week outcome assessment, all of which were neurologically intact with no late complications; the survival rate was considered comparable to that using conventional equipment.25 The second of the studies tested the prototype against a conventional pump in a pig model of HS. Pigs in HS underwent 60 min EPR at 10°C using either the prototype (n=6) or a conventional (n=6) pump before rewarming and resuscitation. Both pumps achieved a 100% survival rate at 72 hours and both groups had one death at the end of the experiment period (3 weeks); one likely from cardiac arrhythmia and one from sepsis. All survivors were neurologically intact.27 The success of the portable low-cost pump is an important step towards real-world testing and application of EPR.
EPR in realistic trauma models
One potential limitation of research into the use of EPR is that many studies use blood withdrawal alone as a method of inducing HS and the additional effects that trauma might have on outcome are not apparent. However, the use of 60 min CirA at a TMT of 10°C in an HS model in dogs with or without additional trauma (from splenic transection) has been investigated. All subjects survived to 72 hours (the duration of the experiment). All subjects in the ‘HS without additional trauma’ group had OPC scores of one. In the ‘HS with trauma’ group, 50% had OPC scores of one, 12.5% a score of two, 12.5% a score of three and 25% a score of four,23 suggesting that HS-only models do not produce the same mortality as more realistic HS plus trauma models. The study's authors suggest this may be because blood withdrawal does not produce the same systemic inflammatory response as trauma. Despite EPR being less effective in experimental models that more accurately simulate real-world trauma, it still produces good outcomes with 62.5% of the ‘HS with trauma’ group scoring OPC 1 and 2.23 EPR is also effective in models of HS with other injuries—60 min of low-flow CPB at 10°C produced good outcomes in pig models of vascular injury, vascular plus colonic injury and vascular, colonic and splenic injury with 6-week survival rates of 90%, 87.5% and 75%, respectively. Furthermore, all survivors were neurologically intact and demonstrated normal learning.
Direct comparison of survival using EPR against a control group using the best current treatment shows EPR to be superior. Wu et al compared normal cardiopulmonary resuscitation (CPR) with EPR. Dogs with splenic transection were bled until CA where they were treated with conventional CPR and fluid resuscitation or EPR (at 10–15°C) for a period of 60 min, before attempted resuscitation via CPB. Post resuscitation, the EPR subjects were kept at 34°C for either 12 or 36 hours. All 7 dogs in the CPR group died, whereas 12/14 dogs treated with EPR survived to 72 hours. In the dogs treated with EPR, those kept at 34°C for 36 hours had better neurological outcomes than those kept at 34°C for 12 hours, with 62.5% scoring an OPC score of 1 compared with 14.2% in the 12-hour post-EPR cooling group. The difference in survival rate between CPR and both EPR groups was statistically significant.15 EPR is a superior intervention to CPR following post-haemorrhage CA in this model replicating both HS and trauma with longer periods of post-EPR cooling, at temperatures several degrees below normal CBT, providing the best neurological outcomes.
Induction of EPR via thoracotomy
The majority of the studies identified during our search cooled subjects via catheters placed surgically before induction of HS, which raises questions about the potential difficulty of inducing EPR in real-world trauma victims in whom access to blood vessels may take too long to allow effective use of EPR. Rhee et al investigated the use of emergency department thoracotomy (EDT) to induce EPR, given that EDT is already used in exsanguinating patients unresponsive to conventional resuscitation. They found that post-HS (via thoracic aortic laceration) it was possible to initiate and maintain hypothermia in pig via the aorta itself. One group of seven subjects was treated with 90 min of CPB-induced 10°C low-flow, during which surgical vascular repair took place, before rewarming and resus; five survived, with four of them having perfect neurological scores. A second group of three animals was maintained at 10°C no-flow for 20–40 min, before resuscitation—two of these survived with good neurological function, with one dying due to accidental extubation. They concluded that induction of EPR is possible through EDT,20 though the death through accidental extubation highlights the need to have robust procedures and training if EPR is to be effective in real-world trauma.
Discussion
Overall, 19/20 of the studies reviewed demonstrated good survival rates with good neurological outcome using EPR after HS, in at least one of the groups they tested. The remaining study identified good survival rates, but reported on gene expression rather than neurological outcome.34 These studies do however have limitations. They are all preclinical or proof-of-concept studies using animal models and the variation in response to EPR between species might indicate that humans could have a different response compared with animal models. It is notable that the investigations into EPR come from a small number of researchers, who have declared competing interests due to holding patents involving EPR.3 ,30–32 There is also significant heterogeneity between the studies in terms of methodology, complicating the matter of integrating the data. Despite all of this, the data from these studies show that EPR has a potential application in treating human HS patients.
There are also potential risks associated with the use of EPR, such as infection and haemorrhage that must be noted; sepsis or infection was reported in 5 studies24 ,26–28 ,33 and antibiotics use was reported in 13 studies.15 ,17 ,20–29 ,33 There is also a clinically observable tendency to bleed more while hypothermic, but this is confined to the cooling phase, and may not be clinically significant because blood in the circulatory system has been rapidly replaced by cooled preservation fluid during the EPR period and injuries are repaired surgically, thus achieving haemostasis.29 Inflammatory and immune response is supressed by EPR although this is also confined to the cooling period and incidence of infection is small compared with the high survival rates reported in all studies.
EPR in humans
EPR would likely be most beneficial to severely injured patients and would need to be initiated rapidly after injury. In reality, it may be difficult to achieve EPR in a timeframe compatible with life in prehospital, battlefield or early hospital settings, but we speculate that it will be achievable in the emergency department by accessing the aorta during EDT, as described by Rhee et al.20 In our opinion, animal studies of EPR show promise and investigation of EPR in humans is warranted.
A clinical trial of EPR on patients who suffered exsanguinating CA following penetrating trauma (stabbing or gunshot wounds) is underway.35 ,36 The literature surrounding this trial did not meet the inclusion criteria to be part of our results, but it is the most important piece of work in this field to date. It is predicted that the results of this EPR for Cardiac Arrest from Trauma (EPR-CAT) trial will not be ready for publication for another 2 years (S Tisherman, personal communication, 2016); however, this trial may start to offer more definitive answers to the question of whether EPR is either practical or effective in critically injured humans.
Conclusion
EPR can be used to provide additional time for haemostatic surgery in animal models of HS, and if this can be replicated in human HS patients, it may reduce mortality in the most severely wounded trauma victims. The studies on large animal models suggest that rapid cooling (2°C/min to 10°C) using cooling fluid with the addition of glucose and oxygen as substrates allows the longest period of EPR, while providing good neurological outcomes. While there are risks associated with EPR, such as infection and haemorrhage, the bleeding risk is not clinically significant because it is confined to the cooling phase, during which haemostasis is achieved surgically and the risk of infection is likely to be outweighed by the survival and neurological outcomes in the animal studies described. Achieving cooling in EPR in human trauma victims may not be achievable in a timeframe compatible with life and there are also questions about whether or not it can reduce mortality in humans, while preserving neurological function. The current evidence from animal models does not fully answer these questions but the ongoing human EPR-CAT study may do. Hypothermia in the trauma patient has classically been seen as a terrible foe, but ongoing and future research may demonstrate that in the form of EPR this old adversary could become a new friend.
References
Footnotes
Contributors All authors contributed to this article.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.