Article Text

Abstract
Major incidents occur on a regular basis. So far in 2017, England has witnessed five terrorism-related major incidents, resulting in approximately 40 fatalities and 400 injured. Triage is a key principle in the effective management of a major incident and involves prioritising patients on the basis of their clinical acuity. This paper describes the limitations associated with existing methods of primary major incident triage and the process of developing a new and improved triage tool—the Modified Physiological Triage Tool-24 (MPTT-24). Whilst the MPTT-24 is likely to be the optimum physiological method for primary major incident triage, it needs to be accompanied by an appropriate secondary triage process. The existing UK military and civilian secondary triage tool, the Triage Sort, is described, which offers little advantage over primary methods for identifying patients who require life-saving intervention. Further research is required to identify the optimum method of secondary triage.
- major incidents
- triage
- emergency medical services
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
The priority of primary major incident triage is to minimise rates of under-triage; existing UK military and civilian primary major incident triage tools currently demonstrate high rates of undertriage.
The Modified Physiological Triage Tool-24 (MPTT-24) is a pragmatic approach to primary major incident triage, with low rates of undertriage, and can be used by clinicians/non-clinicians alike.
The secondary triage process is a more detailed assessment and helps to mitigate for the overtriage incurred following primary triage.
Additional research is required to identify the optimum method for secondary triage which is likely to include additional physiological measurements (e.g. Shock Index) and an assessment of anatomical injury.
Even with experienced prehospital clinicians deployed, having a reliable secondary triage process will allow for cognitive off-loading in what is a high-acuity event.
Introduction
Clinical triage has its roots firmly in military medicine with a Royal Naval Surgeon, John Wilson, being the first to describe prioritising patients on the severity of their injuries, be they ‘slight, serious or fatal’.1 There is little difference between Wilson’s process in 1846 and the process of triage that we use today, comprising the process of prioritising patients on the basis of their clinical acuity. In a major incident, where the demand for patients' clinical care overwhelms the available healthcare resources, this prioritisation, or triage, is key to the effective management of the incident. Existing military and civilian major incident doctrine describes prioritising patients into three categories: priority 1 (immediate), priority 2 (urgent) and priority 3 (delayed).2 Using relatively simple algorithms, or triage tools, we use a patient’s physiology as a measure of clinical severity of injury and to predict the need for urgent clinical attention. However, until recently, there has been no agreement as to what constitutes a priority 1 or 2 patient, thereby introducing a considerable barrier to effective major incident triage research.3
Historically, injury scores such as the Injury Severity Score (ISS) have been used as a means to validate both field triage tools for individual trauma patients and also major incident triage tools.4 However, as these can only be calculated retrospectively, they have little relevance in the prehospital setting and moreover represent a flawed metric with which to validate our triage tools.5 More relevant is the need for a life-saving intervention, and in the context of overwhelmed resources such as a major incident, represents the ideal metric with which to validate our triage tools. But what constitutes a life-saving intervention? First introduced as a concept by Baxt in the early 1980s for the purposes of validating field-triage algorithms, the definition of a life-saving intervention has expanded with medical advances, and what started as a list of five procedures has been developed by consensus into a list of over thirty interventions (Figure 1).3 4 6 7

Life-saving interventions defining the priority 1 patient, derived using international consensus methodology. ACLS; Advanced Cardiac Life Support
The problem
When the performance of existing methods of triage such as the Major Incident Medical Management and Support (MIMMS) Triage Sieve and the UK Defence Medical Services (DMS) Military Sieve is analysed, it is evident that they do not accurately identify those in need of life-saving intervention.8 9 Indeed, this is not a problem unique to UK triage tools; both the START (USA) and Careflight (Australia) tools were found to be just as inaccurate following the London 7/7 bombings.10 Here, in a retrospective study of patients treated at the Royal London Hospital following the terrorist attacks, existing triage tools were observed to demonstrate only 50% sensitivity at identifying those in need of life-saving intervention; in other words, they missed one in every two patients needing an intervention.10
In response to the London 7/7 bombings, the UK’s National Ambulance Resilience Unit (NARU) introduced the NARU sieve. Combining elements of civilian practice (the traditional MIMMS Triage Sieve) and the existing DMS Military Sieve, the NARU sieve now includes an assessment of conscious level and catastrophic haemorrhage.11 12 Unfortunately, a number of military and civilian trauma registry studies have shown that the Military Sieve (essentially analogous to the NARU sieve) also lacks the accuracy to adequately identify those needing a life-saving intervention.8 13
A potential solution
In response to this problem, a method of primary physiological triage that demonstrated improved performance over existing tools was sought.13 The initial aim was to define the priority 1 patient in terms of the requirement for a life-saving intervention. This was achieved through an international process of consensus methodology using experts involved in major incident management. By providing such a definition, it was then possible to create a binary outcome (i.e. those requiring life-saving intervention and those who did not) with which to compare triage tools.3
Using a retrospective military cohort from the Joint Theatre Trauma Registry, a trauma registry containing data on all seriously injured patients treated by the UK DMS; logistic regression methodology was used to identify the optimum thresholds of simple physiological parameters (heart rate, respiratory rate and GCS) at predicting the need for life-saving intervention.13 These thresholds were then combined to produce the Modified Physiological Triage Tool (MPTT).13 In both military and civilian trauma populations, the MPTT demonstrated the greatest sensitivity, correlating with the lowest rates of undertriage (i.e, missing patients in need of life-saving interventions). However, within both populations, the improvement in sensitivity came with a reduction in specificity and had the highest rates of overtriage (classifying patients who did not require a life-saving intervention as priority 1).8 9 13
The dilemma
In an ideal world, the perfect triage tool would have both minimal under and overtriage, but such a tool does not exist; therefore the overall effectiveness of a triage tool lies in the balance between identifying those in need of intervention and minimising those misclassified as either not needing (undertriage) or needing (overtriage) a life-saving intervention.
In the major incident setting where there are multiple patients, the priority must be to identify those in need of life-saving intervention. Failing to identify these patients results in direct and immediate harm; a recent studydemonstrated increased mortality and ISS in cohorts of undertriaged patients.14
Undertiage must therefore be kept to a minimum; in doing so, we must be prepared to tolerate a higher rate of overtriage, which in itself is not without consequence.15 16 If through overtriage medical facilities are overwhelmed with the non-critically injured, there is a concern that these patients may detract from the care for those with critical injuries, thereby resulting in increased morbidity and mortality.16
Reports following the London 7/7 bombings suggest that the overall scene overtriage rate was 64%, which was tolerated with no impact on patient morbidity or mortality.17 However, we must remember that this incident occurred in a major city, supported by four major trauma centres and a number of trauma units. Whether this level of overtriage could be tolerated in a rural or less developed setting is a fundamental discussion point for regional major incident planners.
Science versus usability
Whilst the MPTT was statistically derived and outperforms existing methods of triage, it may not represent the most appropriate method for primary major incident triage.13 A key principle of major incident triage is that it must be rapid, reliable and reproducible. Accurately calculating the GCS takes time, requiring both familiarity and experience but even then, large inter-rater variation has previously been described. Additionally, having an upper respiratory rate threshold of 22 breaths per minute requires the individual assessing the patient to measure the respiratory rate for 30 seconds; when faced with a large number of patients, this is likely to result in the triage process taking a prohibitively long time.
Pragmatic revisions to the MPTT were proposed to increase its usability, resulting in the development of the MPTT-24 (Figure 2).18 As the entry step to the triage tool, an assessment of catastrophic haemorrhage was introduced with the subsequent application of a tourniquet or haemostatic dressing if required. While this has always been a feature of the DMS Military Sieve, it had not been included in civilian triage tools until after the London 7/7 bombings, and reflects recent experience from terrorist major incidents such as the Paris Bataclan attacks where there was a high incidence of injuries associated with catastrophic haemorrhage.19 The GCS assessment was replaced with the Alert, responds to Voice, responds to Pain, and Unresponsive(AVPU) Scale, with the key cut-off point being if the patient responds to Voice. Previous studies suggest that this corresponds to a median GCS score of 13, correlating with that in the MPTT, where the optimum threshold being identified as GCS<14.20–22 Finally, a higher respiratory rate threshold was used (24 breaths per minute), allowing for a more rapid assessment of respiratory rate. By adopting this level, individuals using the MPTT-24 are able to count the respiratory rate for 15 seconds and then multiply by 4 (or 10 seconds and multiply by 6). This step alone will reduce the time required to calculate the respiratory rate by 15(or 20) seconds, thereby reducing the overall time needed to triage using the tool by up to a half.

Modified Physiological Triage Tool-24 (MPTT-24). Vassallo 2017 CC BY 4.0.18
Within both military and civilian trauma registry settings, the MPTT-24 was shown to clinically and statistically outperform the existing NARU and Military Sieve.18 The MPTT-24 conveys two distinct advantages over its precursor the MPTT; first, it can be performed more rapidly, and second it is more suitable for non-clinicians from other emergency services.
Future directions
Within the UK, existing military and civilian major incident doctrine uses a two-stage approach to triage.2 12 The first (primary triage) takes place at the scene of the incident, and as described previously, is a quick assessment of the patient using simple physiology to determine their need for life-saving intervention. The background and clinical experience of the provider performing primary triage will vary. While it will predominantly be undertaken by the Emergency Medical Services, in some circumstances, such as a Marauding Terrorist Firearms Attack, it may not be a healthcare professional but a firearms officer performing the triage.19 The process therefore must be reliable and reproducible, irrespective of the background and experience of the individual providing it.
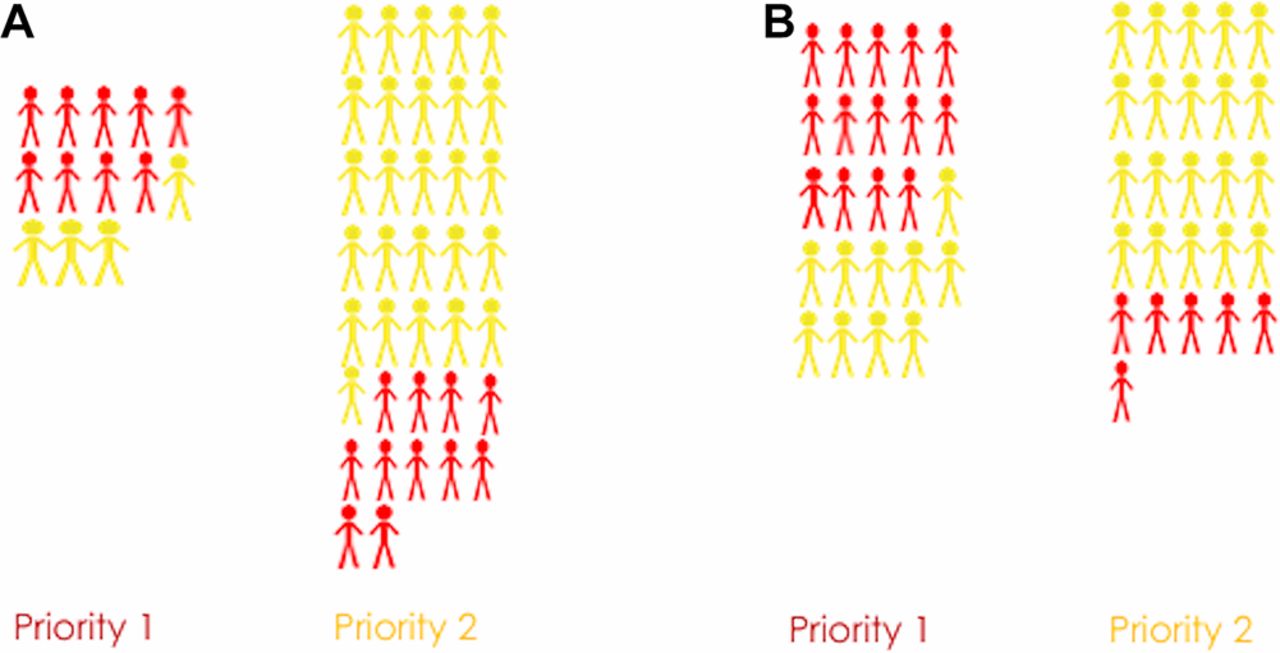
With the priority of primary triage to maximise the identification of genuine priority 1 patients and to minimising undertriage, the MPTT-24 represents the optimum method with which to acheive this. However,whilst adopting the MPTT-24 will reduce the undertriage rate, it will result in more patients (not in need of life-saving intervention) being categorised as priority one (greater overtriage)(Figure 3).18
{kind=link}
{kind=link}
{kind=link}
Comparison of under and overtriage rates between the Military Sieve (A) and Modified Physiological Triage Tool-24 (MPTT-24) (B).
Secondary triage
The secondary triage process is designed to be a more accurate assessment of the patient. Typically taking place in a more permissive environment (away from the actual incident itself), it is a more detailed assessment of the patient and is usually performed by a more experienced clinician, allowing for the application of clinical gestalt.2 Therefore patients overtriaged by the primary process will be reassessed, allowing for downgrading of triage category if required; thereby reducing the overall rate of overtriage. Performed appropriately, this process should ensure that patients needing a life-saving intervention receive these in a timely fashion, while de-escalating care for those who do not need a life-saving intervention.
Prior to the development of the MPTT and MPTT-24, an analysis of the existing secondary triage process (the Triage Sort) and its ability to identify those in need of life-saving intervention within a prospective military environment was undertaken. In this setting, it was found to give little benefit over the existing Military Sieve in terms of sensitivity and rates of undertriage.23 The MPTT-24 outperforms the Triage Sort and conveys a number of advantages, namely speed of use, no requirement for senior clinicians and not being reliant on blood pressure monitoring. With a lack of improvement in performance over primary triage methods, the Triage Sort is itself, not fit for purpose as a secondary triage process.
Whilst the physiological assessments within the Triage Sort do not convey an advantage over the MPTT-24 in terms of performance, the implication of senior clinician gestalt on triage tool performance have not previously been identified and this is included in the Triage Sort as the final stage ‘upgrade at senior clinician discretion’.2 Reports from the London 7/7 bombings suggest that where senior clinicians performed triage, rates of overtriage were lower, implying that there was an improvement in triage performance.17 A hugely variable factor, it is unlikely to be possible to objectively measure clinical gestalt, and thereby to compare performance independently against physiological assessment.
Due to the nature in which the MPTT was derived, it is likely to represent the optimum performance that a simple physiological triage tool can have at predicting the need for life-saving intervention and we are likely to have now exhausted the use of simple physiological assessment for this purpose.13 While it is reasonable to assume that senior experienced clinicians at a major incident will add benefit to the triage process, they may not always be available to do so. Gestalt should therefore complement any secondary triage process, rather than the secondary process being reliant on it. Having exhausted the potential of simple physiological assessment, the adoption of alternative physiological assessments such as the Shock Index or the assessment of anatomical injuries may provide the additional performance that is required for secondary triage.23
Conclusions
A key principle of major incident triage is that it must be able to be performed rapidly, with reliable results, irrespective of the background of the provider using it. Within the high stress environment of a major incident, the use of triage algorithms allows for this and enables an element of cognitive off-loading. As patients progress through each echelon of care at a major incident, the accuracy of the triage process assessing them must increase. Triage is a dynamic process, and for it to be effective at a major incident, it needs to be a tiered process. While we are confident that the MPTT-24 represents the optimum method of primary physiological triage, research is urgently needed to investigate the optimum secondary triage process.
References
Footnotes
Twitter @jamievassallo, @defprofem
Contributors JV drafted the original manuscript with SH and JES reviewing the draft and contributing substantially to subsequent revisions.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.