Article Text

Abstract
Introduction Alcohol-related harm continues to represent a major public health problem and previous evidence suggests that alcohol misuse within the UK Armed Forces is higher than in the general population. The aim was to introduce a population-level primary care intervention with an existing evidence base to identify and support Service Personnel whose drinking places them at greater risk of harm.
Implementation Following successful piloting, the Alcohol Use Disorders Identification Test-Consumption (AUDIT-C) brief screening tool was introduced as part of routine dental inspections by Defence Primary Healthcare (DPHC) dentists. Alcohol brief intervention (ABI) advice and signposting to support services was offered to personnel identified as being at increased risk and recorded in the patient’s electronic health record.
Achievements to date Patients attending DPHC Dental Centres are now routinely offered AUDIT-C with 74% (109 459) personnel screened in the first 12 months rising to over 276 000 at 24 months, representing the single largest use of AUDIT-C and ABIs in a military population to date.
Discussion Introduction of AUDIT-C has seen Defence successfully deliver a whole population alcohol initiative, overcoming implementation barriers to demonstrate the flexibility of a dental workforce to deliver a public health intervention at scale and contributing towards promoting positive attitudes towards alcohol use. The initiative represents a first step towards the goal of a standardised alcohol screening and treatment pathway across DPHC while recognising that the Defence Medical Services are only one aspect of the broader public health approach required to tackle alcohol-related harm in Service Personnel.
- dental
- alcohol
- public health
- primary care
Data availability statement
There are no data in this work.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known on this topic
Alcohol-related harm is a major public health problem in the UK and requires a multisectoral preventive approach which includes primary care interventions.
Alcohol use in the UK Armed Forces has been reported to be higher than in the general population and alcohol misuse impacts on health, well-being and operational effectiveness.
The evidence base for alcohol screening and brief interventions in primary care is well established.
What this study adds
The largest military alcohol intervention to date has routinised population-level brief screening and signposting and is delivered by the dental workforce.
A piloted training model served to increase practitioner confidence and positively influence beliefs which in turn promoted acceptance of the initiative by dental teams.
The methodology and lessons learnt could be adapted to any primary healthcare setting.
Introduction
Alcohol-related harm impacts at an individual and a societal level and represents a major public health problem.1 Tackling alcohol misuse requires a coordinated approach beyond the remit of healthcare services alone and encompassing population strategies but primary care, including dentistry, can play an important role in raising awareness and preventing the development of harmful drinking habits through early identification and brief advice. Primary care clinicians can also facilitate access to mental health and specialist addiction services as part of an alcohol treatment pathway. The benefits of preventive lifestyle interventions to oral and general health are recognised2 and the expectations on primary care dental teams in relation to alcohol are implicit in guidance from the National Institute for Health and Care Excellence (NICE) and the Royal College of Surgeons.3 4 These are underpinned by an established evidence base for the effectiveness of brief interventions.5 6
Aside from well-publicised general health impacts, alcohol misuse is a major risk factor for oral cancer and increases the risk of dental trauma and facial injury.7 8 NICE9 and the Department of Health’s ‘Delivering Better Oral Health’ (DBOH)10 recommend the use of alcohol screening tools and alcohol brief interventions (ABI) by dental teams as preventive strategies to promote sensible drinking. DBOH highlights the opportunity provided by routine dental attendance to deliver brief alcohol advice to patients drinking above recommended levels, while brief interventions by dental and other medical professionals contribute to wider efforts to ‘Make Every Contact Count’ when delivering preventive messages.11
What do we mean by harmful drinking?
Alcohol misuse means drinking excessively or exceeding the lower risk limits. The terms harmful or high-risk drinking describe a pattern of alcohol misuse which directly contributes to health problems whereas the term dependence is associated with alcohol tolerance, cravings or a preoccupation with drinking that continues despite harmful outcomes.12
Does the UK Armed Forces have a problem with alcohol?
Evidence indicates that alcohol misuse within the UK Armed Forces (UK AF) population is higher than in the UK general population,13 14 with estimates of increased risk drinking levels ranging from 39%15 to 67%13 of the total service population. The impacts of alcohol misuse on Service Personnel (SP) can be significant and include: postdeployment violence, negative relationship changes, problems at home, self-harm and various disciplinary offences, all of which threaten individual well-being and can harm operational effectiveness.13 16 A recent paper found that alcohol misuse continues to be one of the most common mental health conditions among serving and ex-serving UK SP, yet individuals who were misusing alcohol were less likely to seek professional support than those experiencing other mental disorder symptoms.17 A report by the Institute of Employment Studies on ‘Alcohol in the Armed Forces’ identified a requirement to introduce interventions to reduce the impact of excessive alcohol consumption in SP and recommended the use of alcohol screening tools, the provision of education and training for practitioners and an agreed protocol of care.16
Prior to the introduction of Alcohol Use Disorders Identification Test-Consumption (AUDIT-C) in the UK AF, SP were not routinely asked or advised about alcohol use using any standardised approach. An opportunity existed for the dental workforce to integrate the brief AUDIT-C screening tool and ABIs into routine inspection appointments alongside smoking, dietary and oral hygiene advice as part of a common risk factor approach.
An opportunity for a public health initiative
All UK SP are required to attend for a periodic dental inspection (PDI) to ascertain an individual’s dental risk status and to treatment plan as necessary to: restore and promote oral health, ensure operational readiness and to reduce the risk of dental morbidity. Recall intervals are determined by the patient’s oral health risk and are consistent with NICE Dental Recall Guidelines, ranging in frequency from 6 to 24 months.18
Historically, a patient’s weekly alcohol consumption was recorded by the patient on a medical history form prior to a dental inspection. These data were incorporated into the patient’s individual electronic health record (iEHR) and were used to report population estimates of alcohol consumption but the findings were inconsistent with those in the literature for the UK AF and the median consumption figure of just 10 units was thought to be an underestimate.15
Defence dentistry’s access to the UK AF population on a regular recurring basis offered the opportunity to introduce AUDIT-C and ABIs to routinely screen, advise and, where indicated, signpost SP to support services. Importantly, dental services could identify personnel who might otherwise not have sought help for alcohol-related issues.
Translating opportunities into action
Piloting AUDIT, AUDIT-C and brief interventions
The AUDIT developed by the WHO is a 10-question screen that identifies potentially increased risk drinking. The AUDIT-C19 is a shortened three-question version of AUDIT for rapid use in a clinical environment to help identify patients whose alcohol use may potentially place them at increased risk. The AUDIT-C has been used in a wide range of primary care settings and populations20 21 but this was the first time it had been used at scale in a military setting and there are currently no published studies validating its use in military populations.21 22 The initial pilot15 trialled the full 10-question AUDIT accompanied by ABIs as a preventive harm reduction tool.
ABIs offer the opportunity to support individuals who drink alcohol at increased or higher risk levels.23 They occupy a gap between primary prevention and the treatment of serious alcohol disorders.20 An ABI is a brief, evidence-based, structured conversation about a patient’s alcohol consumption. This non-confrontational approach seeks to motivate patients to consider making changes to their drinking behaviours.5 24 The introduction of ABIs into a dental setting can improve a dental patient’s awareness of recommended drinking guidelines and alcohol-related health consequences24 and has the potential to stimulate a patient’s internal motivation to take action, even if this is simply ‘sowing the seed’ for a later decision.
For the initial pilot, six single and multichair Defence Primary Healthcare (DPHC) Dental Centres participated (two each from the Army, Royal Air Force (RAF) and Royal Navy (RN)).15 Quota sampling identified a representative sample that was stratified into four age groups. A questionnaire was developed to assess staff attitudes towards the delivery of AUDIT and ABIs in a dental setting. Participating dental centre staff were trained using a basic educational package developed to provide an overview of the pilot and the evidence for AUDIT and ABIs. Dentists were encouraged to conduct brief (3–5 min) ABIs for patients whose AUDIT score indicated that they were potentially at increased risk.
Developing the alcohol initiative and supporting resources
Following the initial pilot, the feasibility of delivering training in the use of screening and ABIs across all DPHC Dental Centres was piloted. Responding to clinician feedback that the AUDIT was effective but too time consuming to use in dental primary care, 10-question AUDIT was replaced by the three-question AUDIT-C (Figure 1) which is consistent with advice given to dental teams in the Department of Health’s DBOH.10

Alcohol Use Disorders Identification Test-Consumption (AUDIT-C), three-question format.
To facilitate chair side data entry and population-level reporting, an electronic template was incorporated into the patient’s iEHR (Figure 2). Data collection was undertaken during PDIs. The template recorded the AUDIT-C score and outcome interventions, including whether the highest scoring individuals were offered signposting to support services or a general practitioner (GP) referral. AUDIT-C and ABI patient refusals were also recorded.

Defence Medical Information Capability Programme (DMICP) dental record alcohol template.
Follow-up piloting assessed the acceptability of a 2-hour ABI course to deliver training based on the successful ‘Have a Word’ ABI training programme. This programme was developed by Cardiff University’s Violence Research Group,25 was trialled, accredited and delivered by Public Health Wales training teams and was adopted by organisations including Public Health England.26
The initial pilot had highlighted a need to provide clear, concise and standardised patient information to support verbal ABI delivery and to highlight the health implications of alcohol at all risk levels. A wallet card was produced that would be provided to all personnel scoring above zero following AUDIT-C.
Delivering training
In preparation for wider implementation of AUDIT-C, guidance was issued to senior management and all DPHC medical and dental centres, including information on the delivery of AUDIT-C, ABIs and the process for onward referral to primary care medical centres.
The ‘Have a Word’ approach to alcohol screening and brief advice formed the basis of training for all dental professionals across all DPHC Dental Centres, which included over 1000 personnel. The PH Wales Alcohol Training Lead trained 28 alcohol trainers drawn from all dental professional groups. Trainers cascaded the standardised 2-hour ‘Have a Word’ training package to local dental centres, including at overseas locations.
Training emphasised that staff were not providing a specialist alcohol service but that screening would form the basis for advice and signposting of patients whose AUDIT-C indicated a potentially increased risk of alcohol-related harm. This advice could be as short as 30 s to 2 min, provided it was delivered as a targeted intervention. Public Health England has since announced the launch of a dedicated e-learning training resource for dental teams which is used for ongoing training.
In January 2016, the Chief Medical Officer published updated national alcohol consumption guidelines.27 These included the removal of a safer lower limit of alcohol consumption and a recommended weekly limit of 14 units per week for males and females. This was consistent with the direction and advice given to DPHC dental teams.
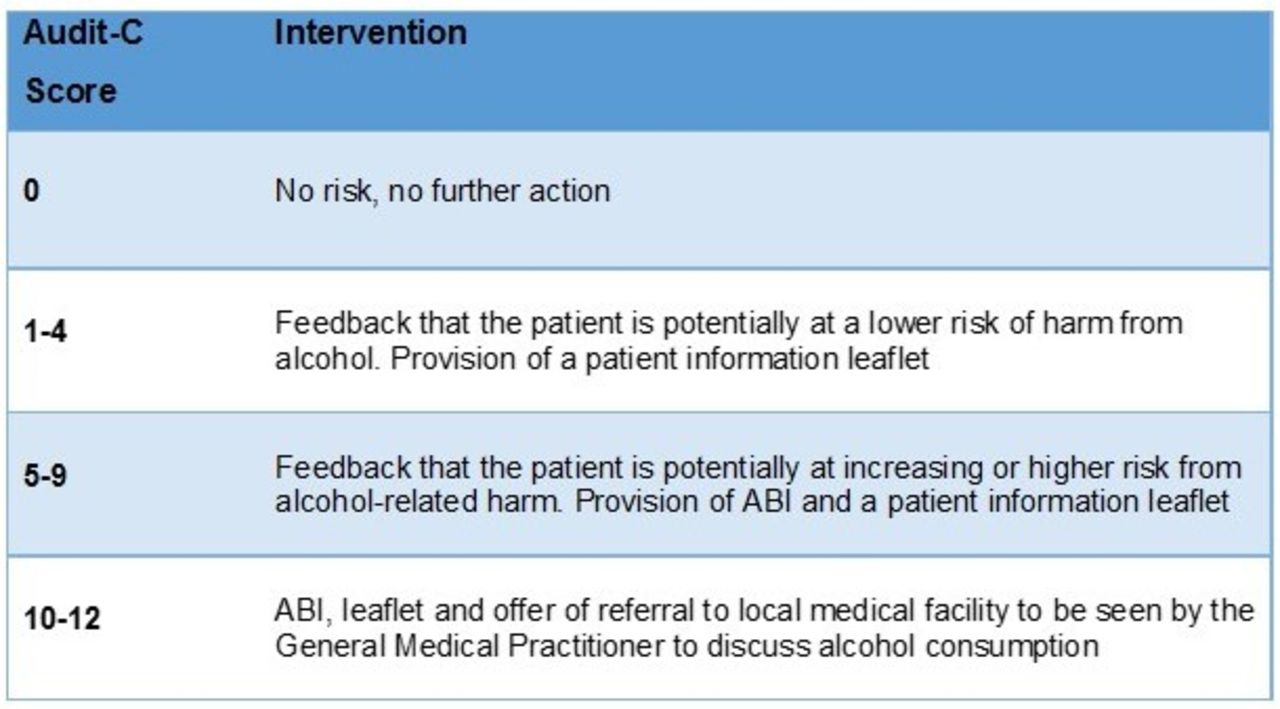
The introduction of AUDIT-C across the UK military took place on 1 June 16 and was supported by wallet cards, Frequently Asked Questions (FAQs) for dental teams and direction on appropriate interventions based on an individual’s AUDIT-C score (Figure 3).

Alcohol Use Disorders Identification Test-Consumption (AUDIT-C) intervention guidance. ABI, alcohol brief intervention.
SP scoring 10–12 on AUDIT-C and thus potentially dependent drinkers would be offered a primary care referral to a DPHC medical facility. Patients could also be signposted to the confidential National Drinkline using the phone number in the wallet card. Patients are free to decline any aspect of the intervention.
Results from the initial pilot of 319 male participants using the full 10-question AUDIT identified that 39% reported a score that indicated an increased risk of alcohol-related harm. Retrospective analysis of previous alcohol consumption data recorded in iEHRs was matched to this cohort, yielding a comparable figure of just 7% who would have been at increased risk. ABIs were recorded for 60% of participants whose AUDIT score indicated they were at increased risk, whereas none of the cohort had previously had any alcohol intervention recorded in their iEHR.
Barriers to delivery of alcohol interventions
Questionnaire feedback was received from 14 of the 20 dentists at pilot sites. Most supported AUDIT over existing arbitrary self-reporting of alcohol consumption but doubts were raised about the feasibility of screening in the dental setting in addition to the existing administrative workload. Other concerns cited a distraction from clinical dentistry, fear of overloading patients with information and the requirement for additional training. These concerns related to conducting full AUDIT rather than AUDIT-C and three-quarters felt that screening and ABIs could effectively raise patient awareness about the risks of heavy drinking.
The initial pilot demonstrated that brief screening offered an acceptable method for identifying individuals whose alcohol consumption potentially places them at increased risk. It facilitated delivery of sensible drinking advice by dentists but highlighted the need for improved training and stakeholder engagement as well as a need to reduce the administrative and time burden on clinicians. The latter was achieved through adoption of the simplified three-question AUDIT-C tool which is recommended in the latest NICE guidance on screening and brief intervention for harmful drinking,4 for use in clinical scenarios where time is limited.
Managing clinician concerns
Subsequent piloting of the model by which training in AUDIT-C and ABIs would be delivered across all DPHC Dental Centres generated further feedback. It was apparent that some dentists were not delivering an ABI to patients scoring 5 or above from AUDIT-C and that the wallet cards were sometimes being used as a substitute for verbal ABI, representing a missed opportunity for behavioural change through verbal reinforcement. Several clinicians expressed concern at the prospect of delivering ABIs to senior officers and worried about managing patients who became resistant or aggressive when asked about their drinking habits.
Further feedback highlighted that dentists wanted clearer direction on the process for offering and making a primary care referral as this was felt to be a significant step over and above the delivery of verbal advice and there was concern about the ethicolegal aspects of managing potentially dependent drinkers.
Training sought to provide solutions for clinician–patient communication barriers and Figure 4 summarises the principles of ABI delivery and engaging resistant patients in the dental setting. Medicolegal societies and Ministry of Defence (MoD) Legal Services provided ethicolegal clarification on the management of potentially dependent drinkers and the resulting practitioner advice received Caldicott Committee approval before promulgation to dental teams in a guidance note. Potentially dependent drinkers were not to be referred to the medical centre without consent. The only possible exception being visible intoxication where immediate intervention might be warranted to prevent serious harm, particularly where safety critical duties, such as driving, were involved. This is broadly in line with existing medicolegal advice for all healthcare professionals.28
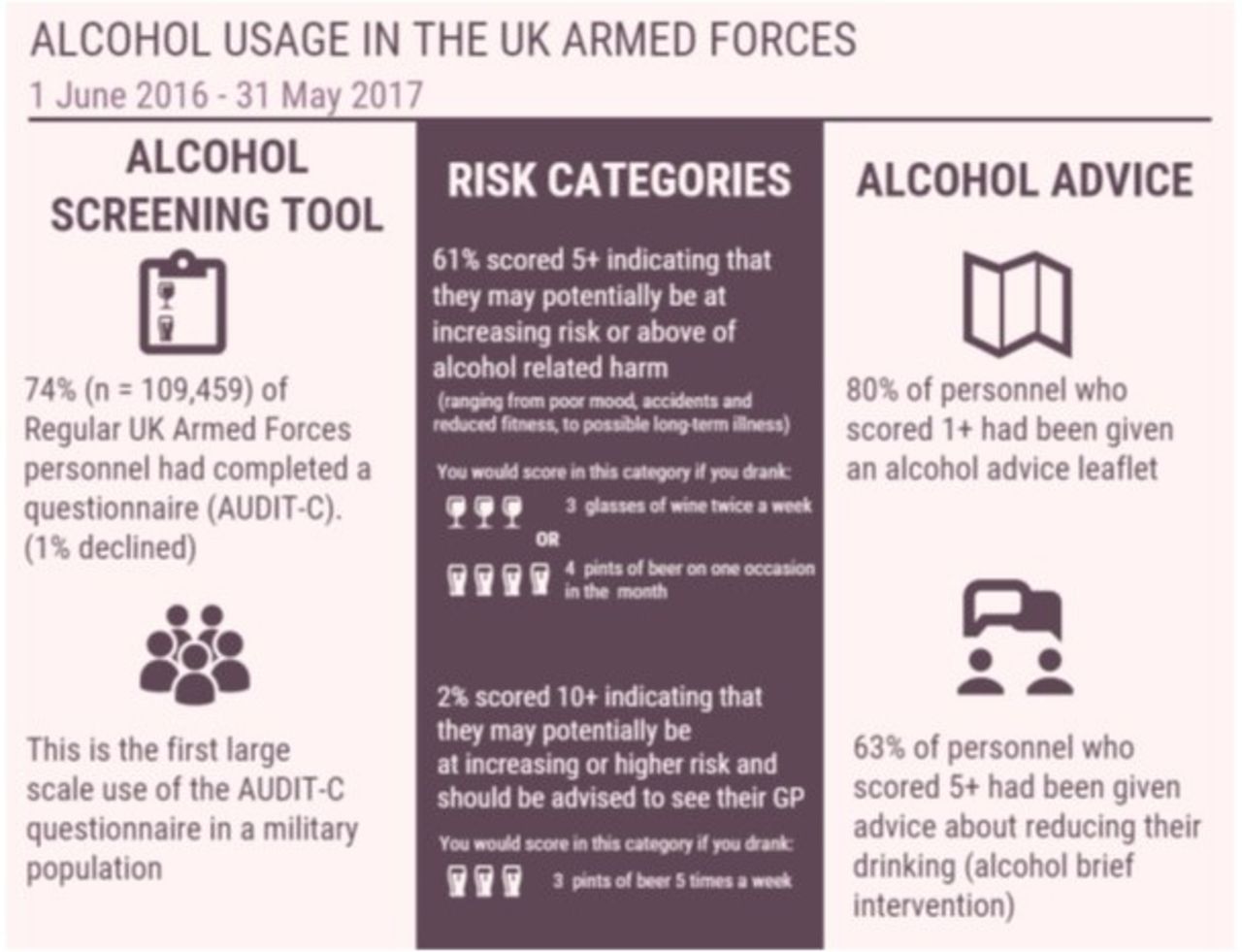
Infographic included in the Official Statistic: Alcohol Usage in the UK Armed Forces 1 June 2016 to 31 May 2017. Published 20 July 2017. AUDIT-C, Alcohol Use Disorders Identification Test-Consumption; GP, general practitioner.
What has been achieved to date?
The introduction of AUDIT-C aimed to engage with over 140 000 trained UK SP over an 18-month period. By June 2017, 12 months on from the Defence-wide introduction of the initiative, 109 459 SP had been screened, representing 74% of the Armed Forces population. A total of 80 662 alcohol advice wallet cards had been issued, 42 074 ABIs had been recorded and 217 individuals with the highest AUDIT-C scores (10–12) were recorded as having accepted a referral to their GP. Just 1% (780) of SP were recorded as having declined an ABI. An Official Alcohol Statistic was published by MoD on 20 July 2017 and key facts are reported in the infographic (Figure 5) extracted from the publication.29

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Summary of advice given to Defence Primary Healthcare (DPHC) dental teams on delivery of alcohol brief interventions (ABI) in the military dental setting. AUDIT-C, Alcohol Use Disorders Identification Test-Consumption.
An evaluation of AUDIT-C and ABIs in the UK AF took place at the 24-month point and will be discussed separately. It used a workforce survey and paired cohort data to demonstrate the effectiveness and sustainability of the initiative with the number of individuals having been screened rising to over 276 000, 90 000 of whom were second AUDIT-Cs delivered at follow-up appointments.30
Achieving sustainability
Prior to AUDIT-C, Defence offered no routine screening or advice on alcohol. Three years on, over 600 individuals have been trained and delivery of AUDIT-C and ABIs by dental teams is routine business. Results to date show that AUDIT-C is accepted by SP and the workforce as part of the common risk factor approach to patient care.
This initiative is a public health first for Defence. Routinely delivering, recording and reporting on a whole population alcohol screening initiative by a trained dental workforce is something that no other military has yet achieved. The initiative was recognised in Defence’s Annual Health and Wellbeing Report as an important achievement.31
The AUDIT-C and ABI population-level data that have been generated are on a scale unrivalled in the military context and offer opportunities to examine the relationship between reported AUDIT-C scores, ABIs delivered and subsequent AUDIT-C at follow-up. However, the limitations of AUDIT-C need to be recognised.
Limitations of AUDIT-C
AUDIT-C is a brief screen; it is not diagnostic and is open to response biases. It does not give a measure of absolute or relative risk and does not discriminate between occasional binge and regular heavy drinking. An individual can drink within the Chief Medical Officer’s Low Risk Drinking Guidelines27 yet achieve an AUDIT-C score that indicates potentially increasing or higher risk from alcohol-related problems. Despite this, the probability of past-year alcohol dependence in individuals scoring 10–12 out of 12 is 75% in men and 88% in women.32 That 2% (2502) of SP identified as being in this highest risk group is of concern and Defence has a duty of care to ensure these individuals are offered further professional support.
The retest reliability of AUDIT-C is good33 but changes in individual AUDIT-C scores at follow-up may represent a learnt response to questioning rather than true behaviour change although screening assessment reactivity, where the act of undertaking AUDIT-C produces a therapeutic effect, is possible. These factors present problems in establishing a causal link between AUDIT-C, ABIs and outcome measures. Despite this, a 2018 Cochrane review found evidence that brief interventions were effective in reducing alcohol consumption in hazardous and harmful drinkers,5 supporting continuation of the initiative.
Selecting outcome measures of success is difficult. Aside from changes in AUDIT-C score, health outcomes such as variations in recorded rates of alcohol-related mental health conditions are subject to confounding and any changes may reflect increased case finding due to greater acceptance and awareness in the UK AF population. Broader outcome measures such as reported rates of alcohol-related driving and disciplinary offences, or aeromedical evacuations due to alcohol-related injury, may be helpful but present similar problems in establishing causal links.
Lessons learnt in overcoming implementation barriers
The UK AF implementation of AUDIT-C and ABIs offers a model for policymakers to consider how large organisations such as the NHS use their primary care workforce to deliver a public health intervention at scale. Embedding screening and brief advice across health services has historically been challenging and improvement initiatives face individual, organisational and system-wide barriers to success.34 Front-line practitioners may lack training in the psychological language of motivational interviewing, the skills to deliver cognitive behavioural interventions or the system-wide support that enables them to deliver an additional intervention on top of a busy workload.
Using evidence to influence practitioner beliefs
Healthcare practitioner confidence and beliefs are important. Individuals are more likely to voluntarily undertake interventions that they believe in and which they find easy to perform and this can reduce barriers to implementation35 while helping to maintain the ‘buy-in’ required for sustainability. Securing Chain of Command acceptance of the initiative was important in facilitating positive leadership. This generated an enabling environment, increasing acceptance within the dental team. The reverse was also found to be true where the local leadership was not engaged. The ‘Have a Word’ programme by Cardiff University’s Violence Research Group36 sought to overcome these barriers through the application of brief advice in a format suited to delivery in the clinical environment. Training takes place in clinical settings and the training team show how brief advice can be adapted to fit the individual circumstances of health professionals. Randomised trials support this approach and have confirmed that brief advice delivered in dental outpatient settings can be cost-effective.37
Next steps
Future work will focus on standardising Defence’s alcohol treatment ‘offer’ as a single pathway spanning primary care teams and mental health services. Defence dentistry will form the implementation model for this work which will be consistent with NICE pathways.38
The AUDIT-C initiative also sought to positively influence the culture and attitude towards alcohol consumption in UK SP at the individual and organisational level. The degree to which this has been achieved is unknown but the Defence Medical Services is just one component of the broader public health approach required to effect change. Defence, as with wider society,39 must focus on evidence-based measures to limit the availability, affordability and social acceptability of alcohol if lasting cultural change is to be achieved.
Data availability statement
There are no data in this work.
Ethics statements
Patient consent for publication
Ethics approval
The dissertation work reported in the manuscript was conducted as service audit (audit registration number RCDM/Res/Audit/1036/14/0402). The remainder of the work is a service improvement project carried out by DPHC as part of routine business.
Acknowledgments
Dr Andrea Docherty—public health consultant for Defence Primary Healthcare, advocate of dental alcohol interventions and SME during development of the initiative. Surg Capt Tim Elmer—current head of the Defence Public Health Unit, consultant in Dental Public Health and instigator of the dental alcohol interventions initiative.
References
Footnotes
Contributors MAD as lead author (corresponding author) was responsible for the idea of the article and drafted the majority of the content. MAD was supported by PF, on whose original MPH dissertation, the work draws heavily and who supplied his dissertation for reference. PF, with support from JS and others, was instrumental in implementing the original alcohol initiative and JS provided input on the training section of the manuscript. RR provided input on sections covering the impact of alcohol on Service Personnel and some of the advantages and disadvantages of AUDIT-C as a screening tool.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.