Article Text

Abstract
Background This article describes a novel patient care algorithm which provides a Role 1 (R1) medic with a structured approach to delivering prolonged field care (PFC) in a resource-limited environment. PFC is a vital component of the operational patient care pathway providing the continuum of care from completion of a primary survey to the delivery to hospital care. Future operational environments are likely to have more fragile or extended lines of communication, potentially delaying evacuation to hospital care. This delay may lead to increases in patient morbidity and mortality. Effective PFC offers an opportunity to improve patient outcomes and help mitigate against this risk.
Methods An initial prototype model of a PFC care process was developed using existing hospital-based guidance. A series of medical and trauma vignettes and best available evidence were used to refine the algorithm.
Results The algorithm has been designed be used in conjunction with patient specific clinical guidance making the approach generalisable for all patient groups. For UK military, clinical guidance is provided by clinical guidelines for operations. The algorithm can be downloaded into a convenient format to be used on mobile devices or printed as an aide memoire.
- prolonged field care
- algorithm
- clinical guidelines for operations
- end organ
- sepsis
Data availability statement
There are no data in this work.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Prolonged field care (PFC) is a process of continuing patient care in a prehospital setting. It starts with the completion of a primary survey and continues until the patient has been handed over to hospital care.1 PFC aims to stabilise, delay or reverse the physiological deterioration of a seriously ill or injured patient through effective patient care supported by timely and appropriate medical interventions. PFC is a vital component of the operational patient care pathway. It represents the incremental care necessary to bridge the potential clinical vacuum between completing tactical field care and delivery to expert hospital care.2
In more recent large-scale conflicts such as Iraq and Afghanistan, the evacuation of sick or injured service personnel was in the majority of cases, reliable and timely.3 As a consequence, there was little imperative to develop or refine a PFC capability.4 5 Future operational environments are likely to have more fragile or extended lines of communication, and this may lead to delayed evacuation to expert hospital care with associated increases in patient mortality and morbidity.6
This article describes a novel PFC algorithm which aims to provide a Role 1 (R1) medic with a structured approach to delivering patient care in a resource-limited environment. In the context of this article, the term R1 medic refers to those UK military career employment groups that may be expected to provide prehospital emergency care and include team medics, combat medical technicians, medical assistants, paramedics, advanced nurse practitioners and medical officers. It is envisaged that this evidence-based step-by-step process of delivering care is generalisable to all patient groups, military or civilian regardless of their age. The process has been designed to be used in conjunction with patient-specific clinical guidelines. For the UK military population, this guidance is found in Clinical Guidelines for Operations (CGOs).7
Background
The initial literature search concentrated on UK and international military journals and published doctrine from the 20th and 21st centuries care using search terms such as delayed evacuation, golden hour, prolonged care and extended care. The aim was to identify elements of patient care and medical interventions that had been shown to improve patient outcomes where there was a delay in receiving expert hospital care. The available evidence from the more recent conflicts in Iraq and Afghanistan was scarce because in most cases patients were evacuated to hospital care within an hour of wounding.3 8 9 Current UK military Battle ATLS10 and US Special Operations Forces11 guidance focuses on delivering specific medical interventions rather than describing a process of patient care. A subsequent literature review of civilian experiences in conflict and disaster zones, expedition and wilderness medicine highlighted the challenges of delivering prolonged care in logistically constrained, resource-limited environments. Non-government organisations such as the International Committee of the Red Cross have published valuable guidance on delivering care in conflict and disaster zones.12 13 Developing end-organ failure or sepsis were common sequelae of delayed access to expert hospital care.14 Addressing these particular threats to patient morbidity and mortality formed the foundation of this new PFC process.
A PFC working group comprising doctors, nurses and paramedics with a background in hospital intensive care or prehospital care attended a series of development workshops. An initial prototype model of a PFC care process was developed using existing hospital-based guidance. A series of medical and trauma vignettes based on epidemiological data from the Iraq and Afghanistan conflicts were tested on the model to refine the care process and tailor it to meet the needs of a R1 prehospital care provider. It became apparent early on in the development process that PFC is not necessarily intuitive to a R1 medic and that a more processes-driven approach to delivering care would assure consistent clinical delivery. The approach also proved to be a useful mechanism for identifying potential clinical and equipment capability gaps. There were challenges in extrapolating NHS best practice into prehospital care. An example being the requirement for X-ray confirmation of nasogastric tube placement. A Defence Lines of Development (DLOD) analysis identified instances where the implementation of hospital guidelines was currently unachievable because of equipment constraints or unrealistic training requirements. In some instances, there was a requirement for compromise, accepting that on some occasions the risks from suboptimal clinical delivery may outweigh the sequalae of no intervention.
The mnemonic ‘HITMAN’ (Figure 1) is currently used by the UK military as a clinical handrail to support the delivery of PFC. It does not describe a process of care and its effective use requires additional clinical training. PFC relies on implementing a broad spectrum of clinical knowledge and skills, many of which are not core business for Role 1 providers, who primarily work and train in military medical centres. To overcome this relative lack of experience, a more prescriptive, process-driven approach to delivering PFC is proposed. HITMAN has provided the foundation for this new algorithm and will continue to be used as a clinical checklist.
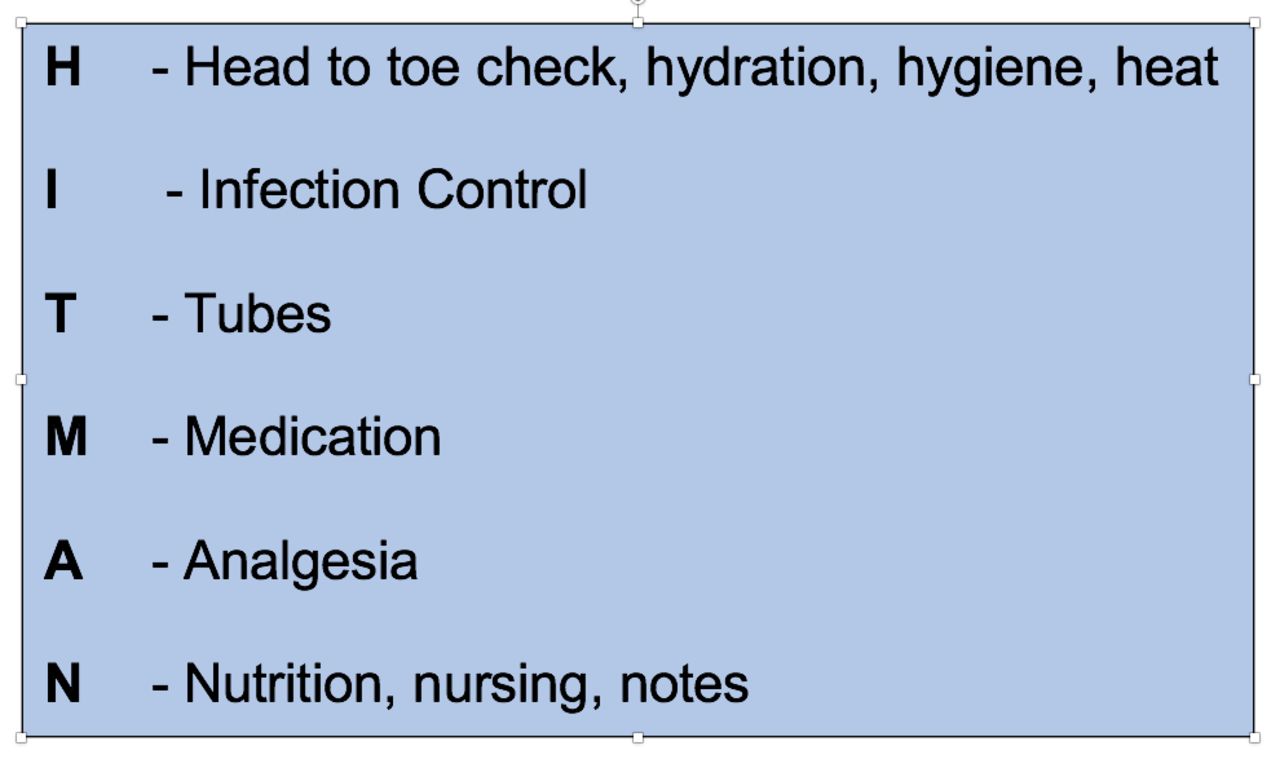
HITMAN mnemonic.
Systematic approach to delivering PFC
The systematic approach to delivering PFC is described as a three-phase algorithm.
Prepare for PFC phase. This initial phase addresses the considerations necessary to achieve a smooth transition from the tactical field care environment and end of the primary survey to a continuous cycle of patient care.
The maintenance phase. This is a continuous cycle of patient care arranged as a prioritised sequence of stages that are linked to patient-specific guidance. This phase of continuous care only stops once the patient has been handed over to expert hospital care. This maintenance phase may be delivered in a static location or on the move during the evacuation phase. It will often be a combination of the two modalities.
Prepare for evacuation phase. During this phase, the R1 medic addresses the considerations necessary to overcome the challenges of maintaining continuity and quality of care during transfer to expert hospital care.
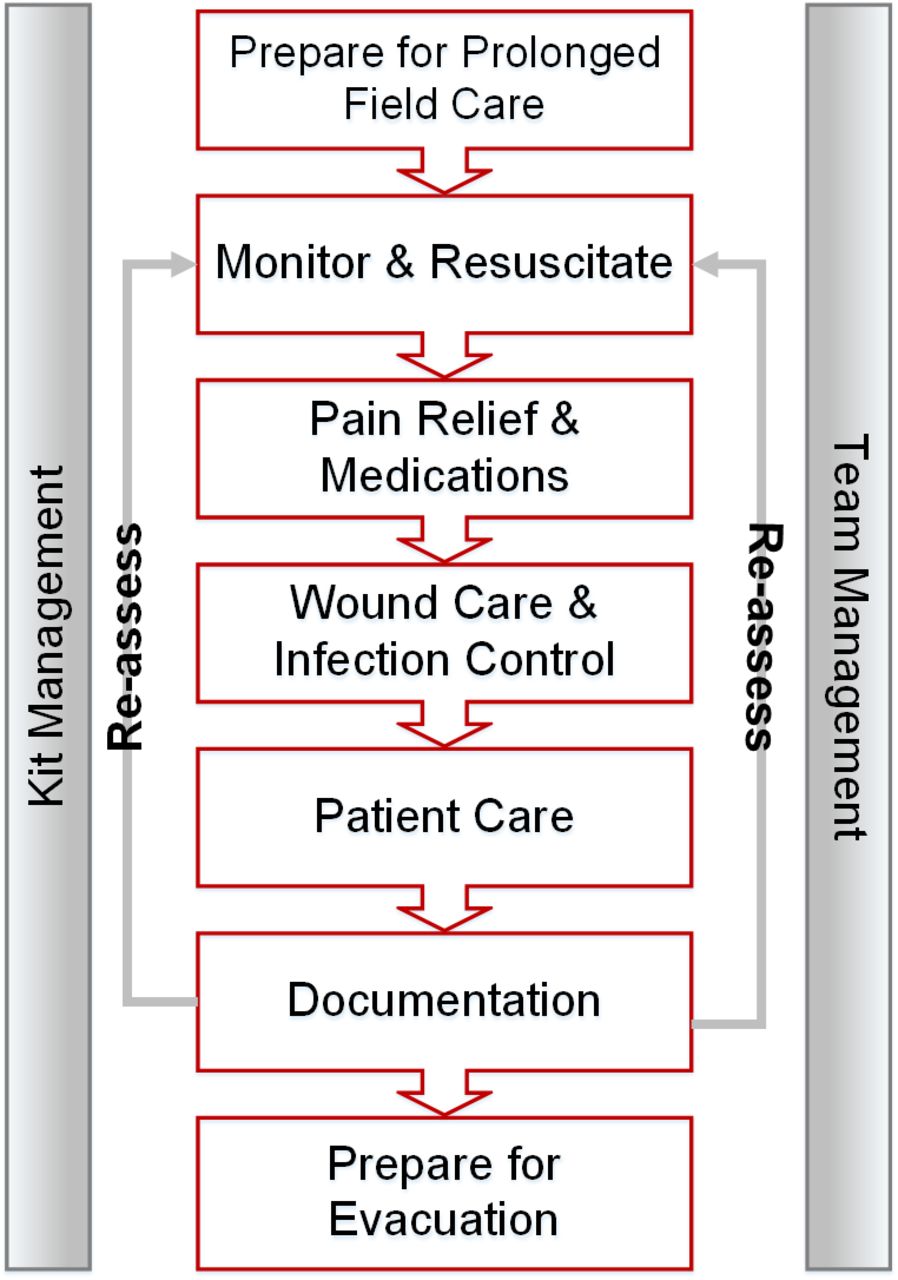
The PFC algorithm is a pathway within the R1 section of CGOs (Figure 2). Each red box within the algorithm either represents a phase of care or a stage in the care pathway. The algorithm has been designed to be used in conjunction with patient-specific clinical guidance making the approach generalisable for all patient groups. For the UK military, clinical guidance is provided by CGOs. By using this approach, the algorithm remains consistent. Any future updates in clinical practice are captured in the relevant clinical guidance.
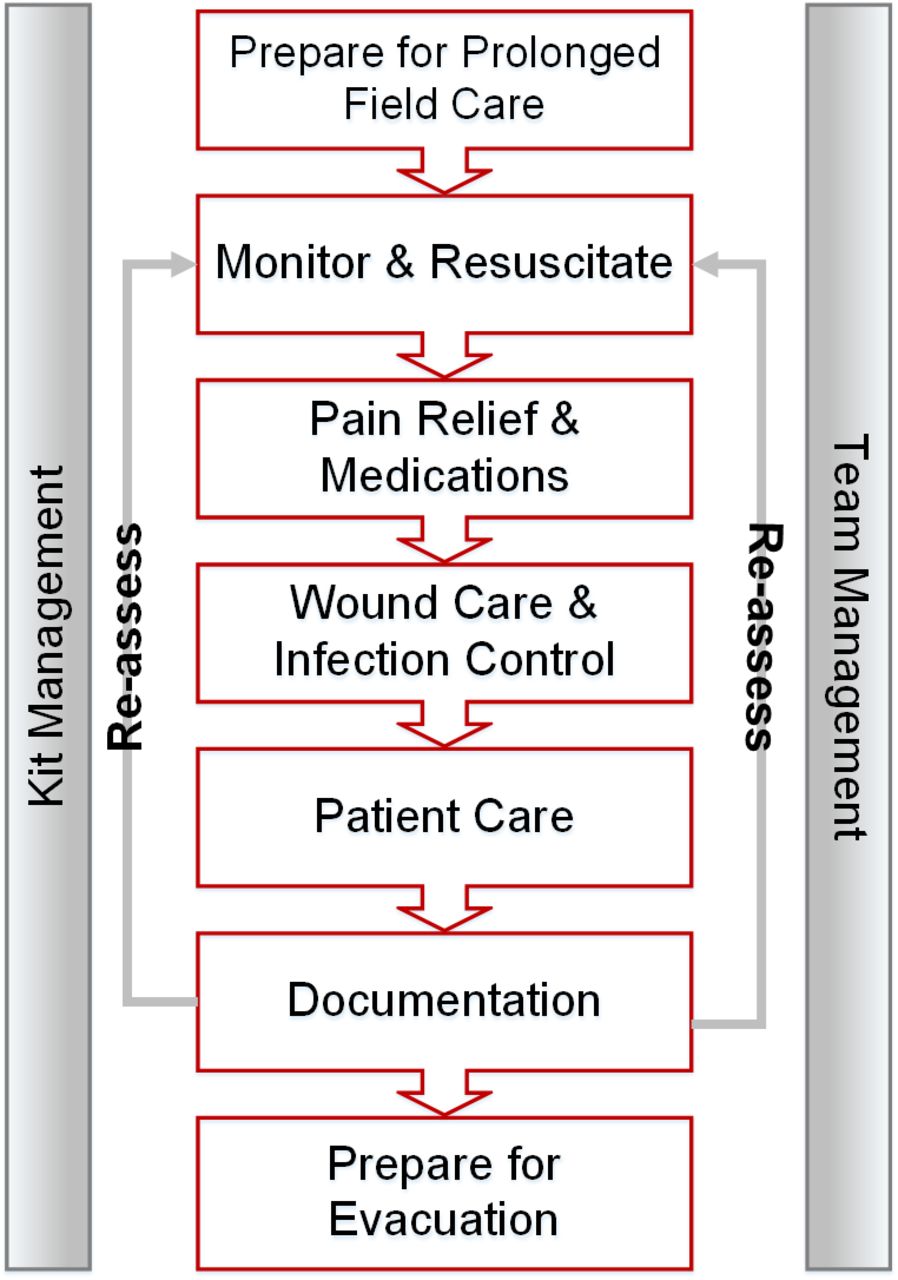
Prolonged field care algorithm.
Prepare for PFC
The prepare phase guides the R1 medic through the transition from tactical field care into PFC. It relies on recognition that the patient requires ongoing care and that there is likely to be a delay in evacuation to expert hospital care. It involves four stages: first, creating a safe environment in which to work; second, an early re-assessment of the patient’s condition; third, a secondary survey; and finally prioritising the problems identified into a plan of care. The priority is to identify and then establish a safe environment for the patient and the medic that is conducive to delivering safe, prolonged and effective clinical care to the patient.
Create a safe environment. This clinical space may be in a static location or on a mobile platform. In many cases, the location or platform will be opportunistic requiring a degree of flexibility, adaptation and improvisation from the medical team supported by some guiding principles. The approach cannot be too prescriptive as is unlikely that any two situations will be the same. The guiding principles underlying the choice of a safe environment are PROTECT, CONTROL and SUPPORT. Protect focuses on safeguarding the vulnerable patient from a variety of man-made and natural environmental threats. Simple measures such as providing protection from the elements, blast or ballistic threat, elevation off the ground and the provision of safety equipment such as eye protection, body armour and insect nets will safeguard the patient from potential harm. Control gives consideration to mitigating the sources of infection. Examples of this include establishing a clean clinical working space while isolating dedicated areas for contaminated and non-contaminated waste. CGOs provide practical guidance on infection control measures. Early consideration should be given to supporting activities of daily living for the patient and the R1 team which requires the provision of potable water, food, sanitation and power. At the end of this stage, a safe clinical area should be established that has been optimised for prolonged field care subject to the tactical or environment constraints of the particular situation.
Re-assess and resuscitate. Moving a patient from the initial point of care to a safer location may potentially interfere with earlier treatment interventions. It is a priority to re-assess and restore appropriate resuscitation before proceeding to the secondary survey. Advice on the appropriate resuscitation protocols can be found in the pathways and treatment sections of CGOs.
Secondary survey. This represents a head to toe search for the traumatic and disease non-battle injuries that are not part of a primary survey. Careful consideration of the mechanism of injury and the subsequent injury patterns will often provide vital clues to identifying the more subtle pathologies. Common illness and injuries that are often overlooked include corneal abrasions, base of skull fractures, ruptured tympanic membranes, subtle axilla and groin wounds, fractures of ankles, wrists and fingers, concurrent chest infections and infected rashes. At the end of this stage, the medic should have produced a comprehensive list of illnesses and injuries that require treatment.
Priorities of care. The illnesses and injuries identified during the primary and secondary surveys should be prioritised according to patient need and clinical urgency. The resulting prioritised problem list forms the plan of care that is used during the maintenance phase.
Maintenance phase
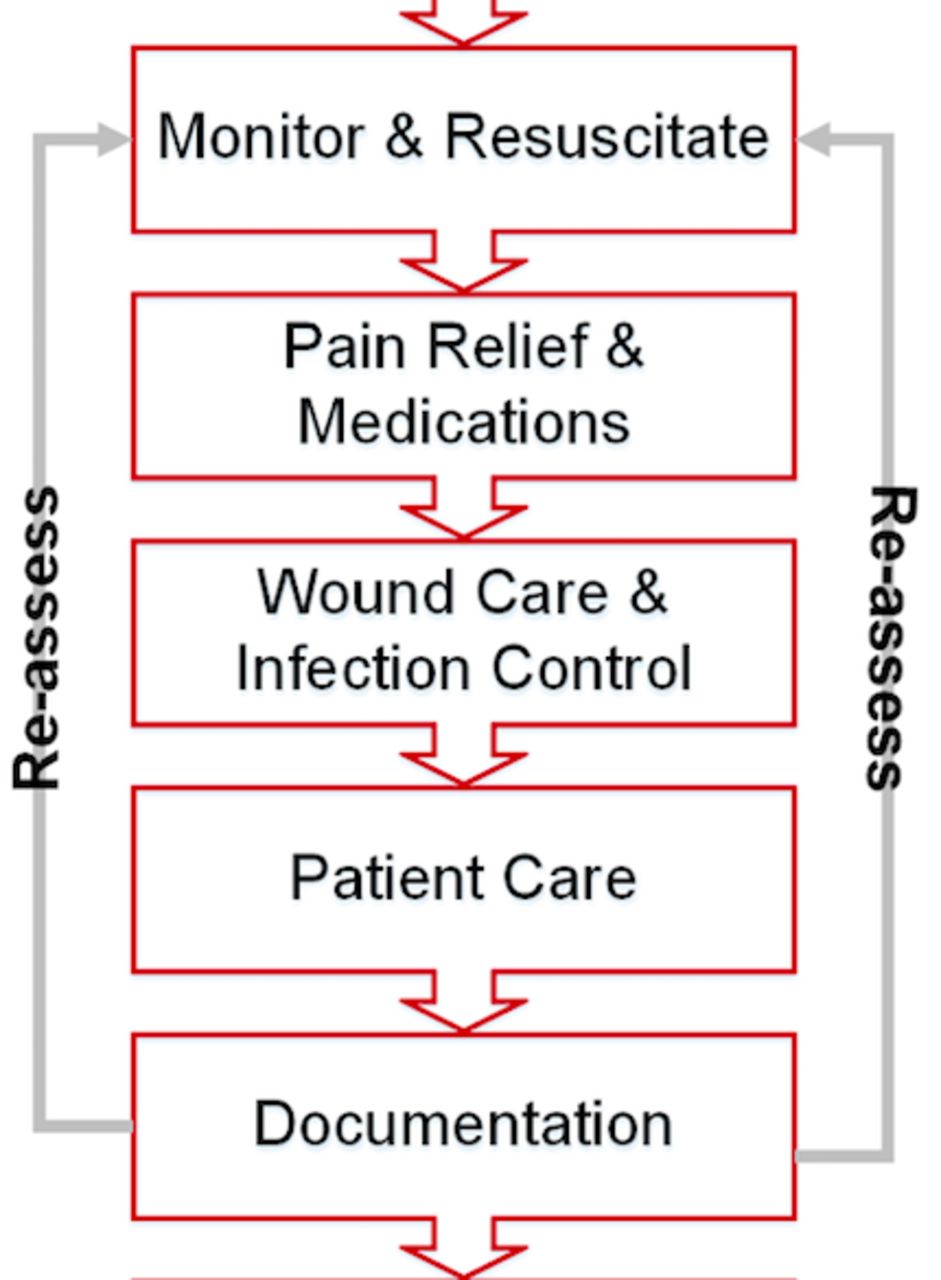
The maintenance phase is a cyclical pattern of care divided into five stages (Figure 3). The stages are monitoring and resuscitation, pain and medication, wound care and infection control, patient care and documentation. The pre-requisite to starting this phase of care is the establishment of a safe environment in which to deliver care and a prioritised treatment list of illnesses and injuries. The maintenance phase is based on delivering cycles of care on an hourly basis. The time allocated to each stage in the cycle remains at the discretion of the medic, but it should reflect the priorities identified during the primary and secondary surveys. The five stages have been sequenced to reflect the priorities of care identified during the literature reviews and the PFC development workshops.8 9 13 14 Evidence and experience suggest that improved patient outcomes are likely to be achieved by delivering appropriate medical interventions and attentive patient care within a prescribed cycle of clinical care.
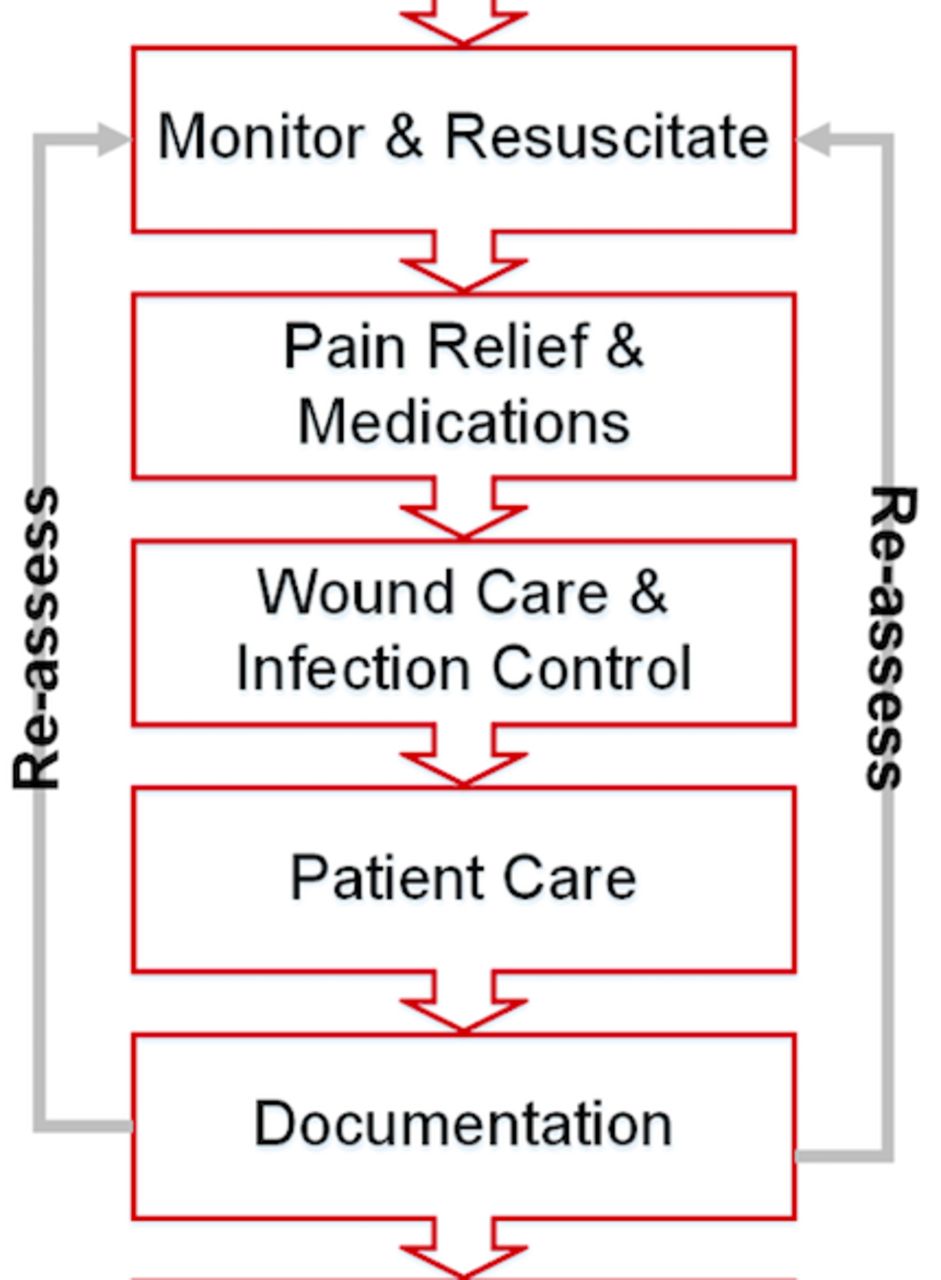
Maintenance phase.
Monitoring and resuscitation
The sophistication of the physiological monitoring available will depend on equipment availability and the scope of practice of those providing the medical care. At the most rudimentary level, monitoring and interpreting observable vital signs are sufficient to identify a deteriorating trend in a patient’s physiology. Early anticipation of a developing sepsis or poor end-organ perfusion offers an opportunity for pre-emptive medical interventions which may improve patient outcome.
The resuscitation stage focuses on addressing the physiological disruption resulting from an injury or illness. The treatment modalities available for resuscitation (eg, intravenous fluids, blood products, oxygen and clotting adjuncts) will depend on the logistical constraints of a particular deployment and the scope of practice of those providing medical care. For the UK military, links to specific resuscitation protocols and treatment guidelines can be found in CGOs. In a casualty with life-threatening haemorrhage, shock should be reversed as soon as possible using a blood product.,. In circumstances where blood products are not available, clotting adjuncts, for example, tranexamic acid (TXA) should be considered alongside early intravenous fluids to restore normotensive physiology.15 Where there are limitations to the availability of monitoring equipment, realistic resuscitation end points that are observable and measurable such as radial pulse, urine output and level of consciousness are recommended.15
Pain and medicines management
Pain management has been prioritised in the maintenance cycle, as early effective pain management has been shown to reduce the overall requirement for analgesia and has an association with improved trauma resuscitation outcomes.16 Effective analgesia allows more thorough wound cleaning and reduces distress for the patient and the medic. Pain should be managed in accordance with the CGOs’ pain ladder. Early use of adjuncts such as patient positioning and fracture splintage will lead to more resourceful use of limited analgesia supplies.
The targeted use of medicines reduces the risk of sepsis, improves clotting and provides prophylaxis against disease. They can improve patient comfort and help alleviate anxiety and in doing so contribute to the psychological well-being of the patient. The availability of medicines in the R1 environment is finite and resupply may not be guaranteed. It is important to take stock of the medicines that are available early in the cycle and plan their judicious use for the duration of the PFC episode. Medicines management can be optimised further by identifying and treating potential problems early emphasising the importance of attentive patient care, regular physiological monitoring, accurate documentation and trend interpretation. The use of medicines is governed by an individual medic’s competency and scope of practice.
Wound care and infection control
Wounds sustained in conflict should be considered to be highly contaminated.17 High-energy projectiles often drag foreign material deep into the tissues and bacterial colonisation and rapid proliferation occur early.18 Accordingly, wound care is a priority due to the increased risk of developing sepsis. Larger wounds will need to be explored and irrigated to remove foreign material and other contaminants. This may require the use of local anaesthetic to provide additional pain relief. As much as 6 L of fluid may be required, but the use of precious intravenous fluids for this function should be avoided. Potable water is suitable for this purposed with no indication for detergents or antibacterial additives.18 For UK military personnel, guidance on wound management including burns and infection control can be found in CGOs. In situations where there is a large wound or multiple wound sites, several cycles of wound care may be required during the maintenance phase. Short concentrated episodes of wound care within the hourly cycle is preferred. This gives the patient some respite from potentially distressing procedures and allows the medic to address the wider holistic needs of the patient.
Patient care
High-quality, holistic patient care is the cornerstone to effective PFC. Guidance in CGOs provides the R1 medic with a structured approach to addressing the physical and psychological needs of their patient. It is based on a hospital model of ‘intentional rounding’ that ensures that a patient’s fundamental healthcare needs are assessed and managed in an organised way.19 Good communication and rapport building are key to alleviating a patient’s sense of anxiety, isolation and vulnerability often associated with injury or illness.20 The process addresses nutrition, hydration, hygiene, sanitation, dressing and mobilisation in a systematic fashion. It should include regular hourly assessments of pressure areas and pain scores. During every patient care cycle, the repositioning of an immobile patient or limb must be considered if pressure sores are to be avoided.
Documentation
Historically, the standard of record-keeping in the prehospital care environment has been of a variable standard.21 Earlier versions of R1 documentation did not support patient observation over a prolonged period. Figure 4 illustrates a prototype R1 casualty assessment chart. The left-hand side of the chart has been designed to record initial patient observations. The upper section captures the age, time, mechanism of injury, injuries sustained together with their vital signs and initial treatments. In the UK military, this is commonly known as the ATMIST report. The lower section allows annotation of the signs and treatments on a diagram with an area to list the problems identified during the primary and secondary surveys. On the right-hand side of the chart, a National Early Warning Score (NEWS) 2 style warning system is intended to graphically alert the medic to abnormal physiological trends. The colour change from white through amber to red is intended as a prompt towards proactive clinical intervention.22 The use of an additional sheet will extend the patient’s observation over a 24-hour period.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Casualty assessment chart.
Prepare for evacuation
This phase ensures that the appropriate preparation and planning has taken place to safeguard a patient during evacuation. PFC must be continued for the duration of the transfer highlighting the requirement for adequate medical supplies and a suitably qualified and experienced medic. Packaging the patient is an opportunity to anticipate potential problems and deal with them ahead of the transfer. All tubes and lines must be secured to ensure continued access for monitoring and treatment. The patient must be comfortable, secured on a stretcher and wrapped in appropriate thermal protection. Hearing and eye protection should be provided based on the environmental threat. A pre-emptive increase in analgesia and use of antiemetics may improve the patient experience.
At times, R1 medical teams may be required to evacuate a patient to an exchange point or medical facility. Careful consideration should be given to the availability, suitability and capacity of the transport options available. Where practicable, the choice of transportation should not compromise patient safety or the capacity to deliver PFC. The mitigation strategies necessary will be unique to each situation but should follow the underlying principles described above. For the UK military, CGOs provide valuable guidance on pre-transfer checklists, vehicle capacities and helicopter safety drills.
Team and kit management
Delivering potentially complex medical care in a semi-permissive, unfamiliar, suboptimal clinical space will be stressful for the medic and the patient. Incorporating human factors considerations into a system of patient care will reduce the likelihood of human error and improve the quality of care given.23 The guidance and training encourages the medic to plan periods of rest for themselves and their patient, and to use other members of their team to ensure the patient receives appropriate care and supervision during the medic’s rest periods. Consideration is given to resource management by taking stock of medicines and medical equipment that have been consumed during the primary survey and optimising the use of remaining stocks over the duration of the PFC. Training includes innovative uses of medical equipment and its packaging to help bridge resource gaps, an example being adapting a SAM splint and plastic bag to construct a washing bowel.
Discussion
This systematic approach to PFC has been designed to be compatible with a whole force concept of usage. This has been achieved by mapping the clinical knowledge and skills required in each stage of care against the national Pre-Hospital Emergency Care competency framework comprehensively described by Sharpe et al.24 Table 1 illustrates a matrix that describes the scope of practice for each PHEC level. To improve the clarity of the table, assume that increasing PHEC level maintain the lower clinical competencies.
PFC/PHEC competency matrix
The text highlighted in red identifies capability gaps, where current training or equipment constrain the quality of clinical care that can be delivered for a particular PHEC level. It is envisaged that the matrix can be used in a number of ways. First, it can inform the medical planning process by defining the quality of care that is achievable by each particular PHEC level. Second, the matrix forms the foundation of the clinical governance and assurance framework. Third, DLOD analysis of the matrix will help inform the training and equipment requirements for the future.
This novel PFC algorithm forms part of the R1 CGOs and links to supporting clinical pathways and treatment guidance. It can be downloaded into a convenient format to be used on hand-held devices or printed as an aide memoire. As DMS medical information systems projects mature, it is envisaged that the PFC guidance will form part of a wider arsenal of telemedicine and critical decision support tools designed to support the deployed medic.
Summary
A novel systematic approach for delivering PFC has been researched, designed and implemented to support the R1 medic. The main effort has been to optimise patient outcome by blending published evidence with subject matter expertise to produce an easy-to-follow, memorable clinical algorithm. The algorithm has been designed to be used concurrently with CGOs. It is described in three phases. The initial phase focuses on preparing for PFC by establishing a safe clinical environment, completing a secondary survey and prioritising the treatment required. The cyclical maintenance phase is repeated for the duration of the PFC with each stage of care revisited on an hourly basis. The cornerstone to this approach is delivering patient-centred care through a prioritised sequence of stages. Each stage is indexed to more comprehensive guidance within CGOs. The preparation for evacuation phase focuses on maintaining a high standard of PFC during the transfer to expert hospital care.
Data availability statement
There are no data in this work.
Ethics statements
Patient consent for publication
Acknowledgments
The authors would like to thank the following people for their valuable contribution to the development of the PFC guidance: Gp Capt Di Lamb (PMRAFNS), Col Chris Wright (L/RAMC), Lt Col Martin Moody (RAMC), Lt Col Harvey Pynn (RAMC), Lt Col Joe D’Arcy (QARANC), Maj Ian Hazzard (QARANC), SSgt Mark Anderson (QARANC). Thanks to Maj Adam Hughes (QARANC) for his patience and advice implementing the PFC guidance into clinical guidelines for operations.
References
Footnotes
Contributors The authors would like to acknowledge the hard work and support from the prolonged field care working group.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.