Article Text

Abstract
The operational and policy complexity of civil-military relations (CMR) during public health emergencies, especially those involving militaries from outside the state concerned, is addressed in several guiding international documents. Generally, these documents reflect humanitarian perspectives and doctrine at the time of their drafting, and primarily address foreign military involvement in natural and humanitarian disasters. However, in the past decade, there have been significant changes in the geopolitical environment and global health landscapes. Foreign militaries have been increasingly deployed to public health emergencies with responses grounded in public health (rather than humanitarian) approaches, while public health issues are of increasing importance in other deployments. This paper reviews key international policy documents that regulate, guide or otherwise inform CMR in the context of recent events involving international CMR during public health emergency responses, grounded in analysis of a March 2017 Chatham House roundtable event on the subject. Major thematic concerns regarding the application of existing CMR guiding documents to public health emergencies became evident. These include a lack of consideration of public health factors as distinct from a humanitarian approach; the assertion of state sovereignty vis-à-vis the deployment of national militaries; the emergence of new armed, military and security groups and a lack of consensus surrounding the ‘principle of last resort’. These criticisms and gaps—in particular, a consideration for public health contexts and approaches therein—should form the basis of future CMR drafting or revision processes to ensure effective, safe, and sustainable CMR during public health emergency response.
- health services administration & management
- clinical governance
- health policy
- international health services
- organisation of health services
- protocols & guidelines
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- health services administration & management
- clinical governance
- health policy
- international health services
- organisation of health services
- protocols & guidelines
Key messages
Global guiding documents that inform civil-military relations (CMR) in humanitarian crises have not kept abreast of recent geopolitical changes.
In particular, the applicability of CMR guiding documents during public health emergencies (as distinct from natural disaster response guided by standard humanitarian principles) is unclear.
Gaps are evident—consideration must be given to the changing international environment, state sovereignty, new armed groups and the principle of last resort.
CMR guiding documents should be reviewed on this basis in order to appropriately inform future CMR during public health emergencies.
Introduction
Civil-military relations (CMR), especially those involving militaries from outside the state concerned, are guided and informed by various United Nations (UN) guidelines, frameworks and policy papers which have evolved incrementally since the 1990s. They generally address the role of international militaries in natural disasters; are international in flavour, rather than focusing on the use of national militaries and are written from a humanitarian perspective reflecting the primary international concern of the early post-Cold War period. Their relevance in a changed environment is thus questionable, especially where militaries are increasingly responding alongside civilian responders to non-conflict public health emergencies such as Ebola or COVID-19. Nonetheless, UN CMR guiding documents are still relied on to inform and critique CMR during these events.
This paper assesses the appropriateness of the current UN CMR guiding documents for the use of militaries in responding to health challenges and concludes with recommendations to inform future revision.
Methods
The focus of this paper is on those UN policy—what we term ‘guiding documents’—in the context of both international and national uses of militaries in public health emergencies.
Key UN policy documents that regulate, guide or otherwise inform CMR were reviewed. Although there are myriad CMR guiding documents and policies from agencies such as Médecins Sans Frontiers, the International Committee of the Red Cross (ICRC) and various military bodies (eg, the USA, the UK and North Atlantic Treaty Organization), because of their centrality in defining CMR policy this review focuses on three documents from within the UN system (Table 1). These documents do not represent the full spectrum of CMR in the humanitarian community. However, they do represent the three core, consensus-driven and global guiding documents that have been adopted and accepted by the UN for wide international consideration and applicability (while part of the ‘core four’ UN CMR guiding documents, this analysis does not consider the 2013 Inter-Agency Standing Committee (IASC) Non-Binding Guidelines on the Use of Armed Escorts for Humanitarian Convoys. This is because the document addresses the use of armed escorts for humanitarian convoys specifically, rather than providing guiding principles for CMR in humanitarian settings more generally).
United Nations Office for the Coordination of Humanitarian Affairs guidelines on civil-military coordination
Core thematic similarities and distinctions between these documents were mapped to identify the historical and political contexts that informed their development, as well as the operational contexts they seek to inform. The outcome was then considered in the context of global events and conversations surrounding CMR during recent public health emergencies and draws on a March 2017 Chatham House roundtable event and report in which we were observer participants.1 Roughly 50 participants attended from military, international (I) non-governmental organisation(NGO), governmental, UN and academic backgrounds, with representation from high-income, middle-income and low-income countries.
Criticisms of existing CMR guiding documents for public health emergency response raised during the roundtable were synthesised and explicated to identify gaps which were then used to identify key considerations that should inform future CMR policy documents.
Background and context: reviewing the CMR policy geography
The civil-military regulatory domain is complex but comprises five broad groupings of policies specific to CMR2:
General guidance on CMR.
Guidelines related to a specific emergency.
Guidelines on particular elements of CMR.
Guidelines relating to specific bilateral arrangements.
Intragovernmental arrangements.
Most of the documents that concern international military deployments fall in group 1 and appear to assume the deployment of a Global North military to the Global South. Several key UN guidelines form the basis of most strategic discussion regarding CMR at the international level. Specifically, the UN Office for the Coordination of Humanitarian Affairs (OCHA) maintains three sets of guiding documents as mentioned in Table 1.
The historical and political grounding of each are therefore briefly outlined, followed by an analysis of the general themes shared between the documents.
The IASC Reference Paper
The Inter-Agency Standing Committee (IASC) Reference Paper (2004) is arguably the most comprehensive of OCHA’s guidelines, complementing the earlier guidelines and providing guidance for the maintenance of humanitarian principles.3 It argues for the maintenance of the civilian character of humanitarian assistance, the use of military as a ‘last resort’ and a clear division of labour wherever possible.4 Starting from this position of ‘difference’, the IASC Reference Paper recognises that both civilian and military groups may ‘pursue common goals… (using) basic strategies (that) range from coexistence to cooperation’ alongside the ‘shared responsibility’ of coordination (Figure 1).3 5 6

Civil-military coordination scenarios.
While the IASC Reference Paper reaffirms the significance of the humanitarian principles (namely humanity, neutrality, impartiality and independence), it is relatively pragmatic in their application, recognising that a humanitarian imperative ‘may at times necessitate a pragmatic approach’ to CMR.3 However, the IASC Reference Paper contains further principles that limit the contributions of military, stipulating that military relief activities are ‘by their nature and definition, not “humanitarian”’.3
Key elements of these principles are listed in Box 1.2
Summary of IASC core principles
The use of military assets is a last resort, and the ‘military should avoid direct assistance unless it is the only way of providing life-saving assistance’.10
The civilian nature of humanitarian assistance must be retained wherever possible.
The ‘distinction’ between humanitarian assistance and military roles in security and relief must be maintained.
The ‘military and civil defence assets of belligerent forces engaged in combat shall not be used to support humanitarian activities’.10
‘Request for the use of military assets must be made by the (UN) Humanitarian (or) Resident Coordinator’.10
The ‘use of MCDA should be planned to be limited in time, and include a clear exit strategy’. This is ‘in order to avoid creating dependency on military support’.10
Countries providing ‘should respect the UN codes of conduct and humanitarian principles’.10
‘As a general rule, humanitarian convoys will not use armed or military escorts’.10
The MCDA Guidelines
The Military and Civil Defence Assets (MCDA) Guidelines were adopted in 1994 by consensus and revised in 2007. They were developed at the request of OCHA and the International Federation of the Red Cross and Red Crescent Societies in response to civil-military interaction in emergencies in the early 1990s, such as the Spitak, Armenia Earthquake (1988) and Operation ‘Provide Comfort’ in northern Iraq (1991–1996). The guidelines provide a model legal framework for the utilisation of MCDA in humanitarian contexts, and address situations such as man-made and environmental disasters in times of peace (Box 2).
Military and Civil Defence Assets (MCDA) definition
MCDA (as defined in the 1994 Oslo Guidelines) includes ‘relief personnel, equipment, supplies and services provided by foreign military and civil defence organisations for international humanitarian assistance. Furthermore, “civil defence organisation” means any organisation that, under the control of a Government, performs the functions enumerated in Article 61, paragraph (1), of Additional Protocol I to the Geneva Conventions of 1949’.17
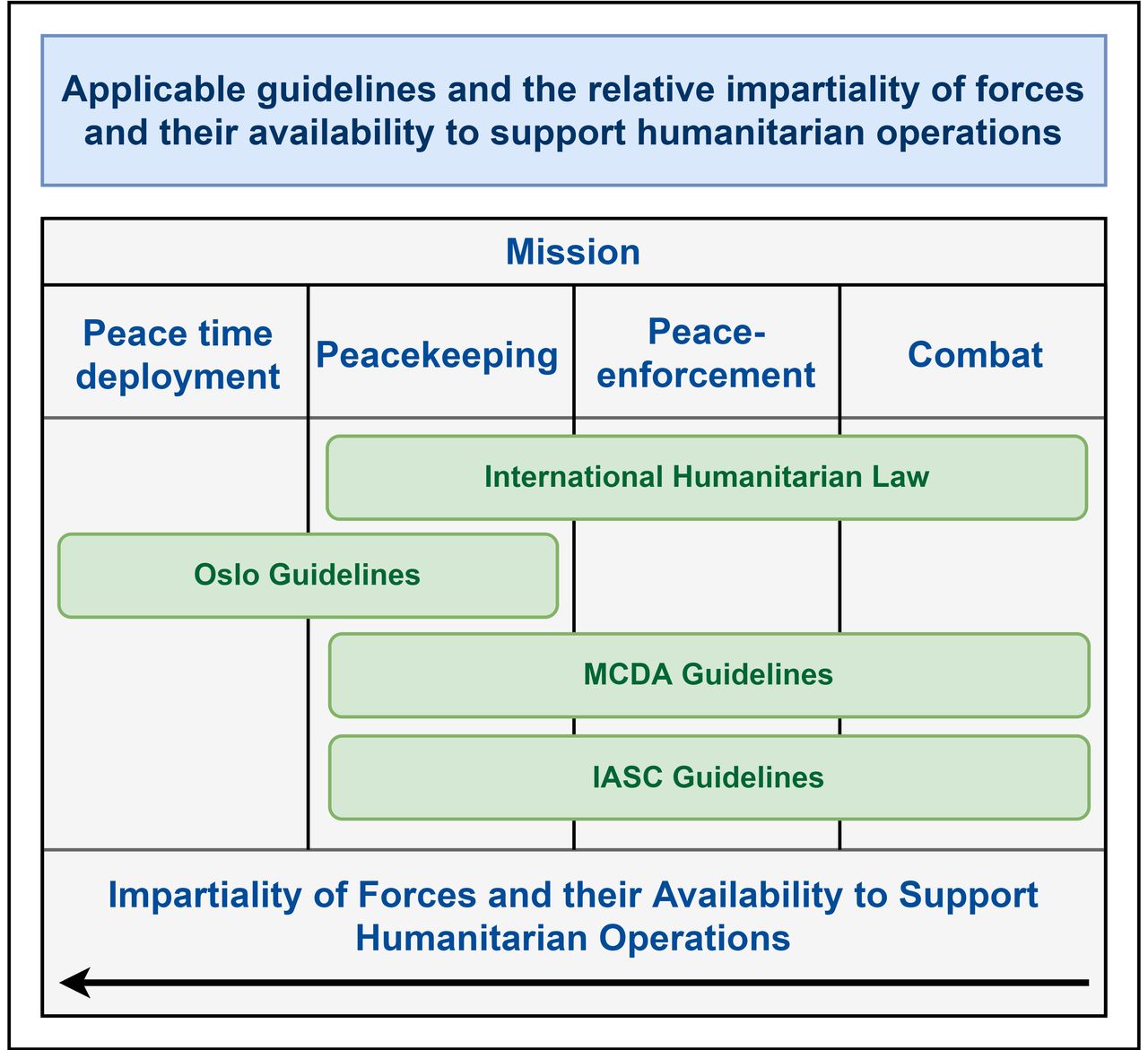
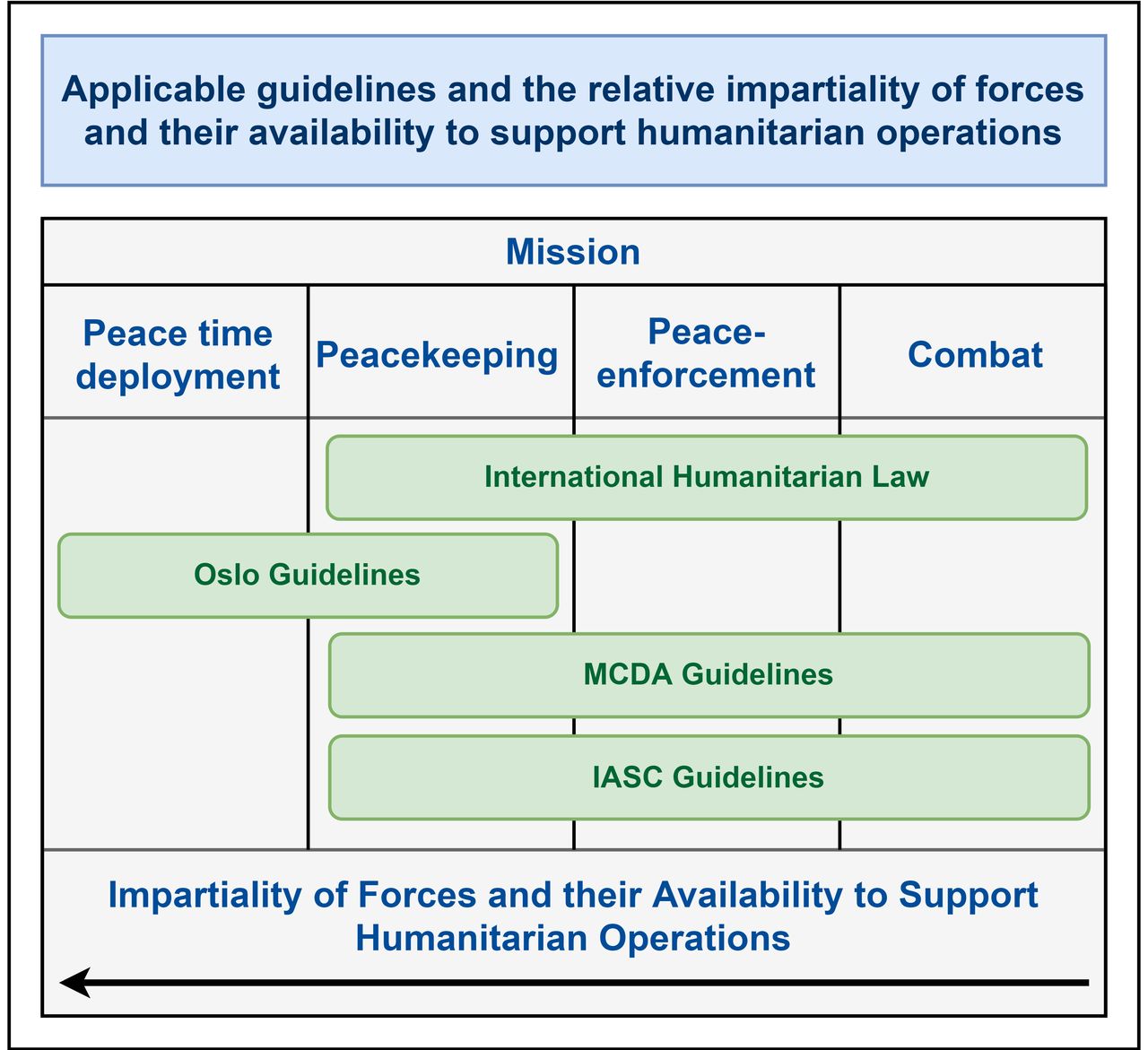
They are intended to establish ‘the basic framework for formalising and improving the effectiveness and efficiency of the use of military teams and expertise in international disaster relief’.7 Unlike the Oslo Guidelines, the MCDA Guidelines presume a viable host state or government, and also provide civil-military guidance in contexts of peace-enforcement and combat (Figure 2).8
{kind=link}
{kind=link}
Applicability of the Office for the Coordination of Humanitarian Affairs guidelines. MCDA, Military and Civil Defence Assets.
The Oslo Guidelines
The Oslo Guidelines, developed in 1994, underpin most global policies and ‘were intended to establish principles and standards that would improve (the) coordination and use of military and civil defence assets in response to natural, technological and environmental emergencies in peacetime’.5 Emerging under the auspices of the Consultative Group on Humanitarian Civil-Military Coordination, they enjoy a unique status of being internationally agreed and IASC-endorsed and are the ‘leading international instrument concerning the role of militaries in the response to natural disasters’.9
Key elements of the Oslo Guidelines are mentioned in Box 3.
Key principles of the Oslo Guidelines
‘Last resort’: ‘foreign military and civil defence assets should be requested only where there is no comparable civilian alternative, and only when the use of foreign military or civil defence assets can meet a critical humanitarian need. The foreign military or civil defence asset must therefore be unique in capability and availability’.17
Foreign military and civil defence assets should ‘be seen as a tool complementing existing relief mechanisms in order to provide specific support to specific requirements, in response to the acknowledged “humanitarian gap”’.26
Military and civilian defence assets ‘can be mobilised and deployed bilaterally or under regional or alliance agreements as “other deployed forces” or as part of a United Nations operation as “UN MCDA”. All disaster relief… should be provided at the request or with the consent of the Affected State and, in principle, on the basis of an appeal for international assistance’.17
All relief actions ‘remain the overall responsibility of the (Affected) State and are complemented by a foreign (military or civil defence force) operating (bilaterally or) within an international relief effort’.7
‘Distinction’: military personnel should be unarmed, but remain in military uniform.
Foreign military and civil defence assistance ‘should be provided at no cost to the Affected State, unless otherwise agreed between concerned States or as regulated by international agreements’.17
‘An Assisting State deciding to employ its (military and civil defence assets) should bear in mind the cost/benefit ratio of such operations as compared to other alternatives, if available. In principle, the costs involved in using (military and civil defence assets) on disaster relief missions abroad should be covered by funds other than those available for international development activities’.17
‘As a general principle, UN humanitarian agencies must avoid becoming dependent on military resources and Member States are encouraged to invest in increased civilian capacity instead of the ad hoc use of military forces to support humanitarian actors’.17
Recommendations
Identify appropriate actor(s) and convene a high-level conference, possibly hosted by the Office for the Coordination of Humanitarian Affairs, with a view to reviewing existing civil-military guiding documents collectively, rather than addressing revision processes guideline by guideline.
Consider new guidelines or frameworks that specifically address the deployment of a foreign military to a public health emergency response, as distinct from a natural or sudden-onset disaster response, or identify ways of adapting existing guidelines that can accommodate these contexts; ensure this takes the changing international environment into account.
Alternatively, consider the development of a set of principles against which civil-military cooperation can be planned and assessed for each specific operation and intervention, in lieu of relying on guidelines to inform all civil-military activities.
Adapt civil-military guideline terminology and make it more flexible, so that it can accommodate the fluid environments and contexts in which protracted public health emergencies unfold.
Identify and address military, security and other armed groups not covered in existing international guiding documents.
Revisit the principle of ‘last resort’, to provide and include a more nuanced understanding that includes considerations weighed against the humanitarian imperative.
Ensure maintenance of civilian leadership in humanitarian activities, but consider military involvement as part of a multisectoral approach.
General themes shared among the guiding documents
These guiding documents are consistent in emphasising compliance with two humanitarian (rather than public health) principles: they emphasise action based on impartial needs assessments, free from discrimination; and the use of military assets only as a ‘last resort’. They discourage dependency, encourage maximal civilian operational independence and control and advocate distinction between military and civilian activities. These principles should be maintained, even if they may circumstantially disadvantage beneficiaries. They are intended to regulate international third-party interventions and do not address the consequences of a host nation taking a different view. Health is placed within a broader humanitarian context, rather than defining public health emergency contexts.
A related and recurring theme is that associating civilian organisations with military bodies may undermine civilian humanitarian activity and endanger the safety of civilian personnel.10 This is particularly relevant in conflict environments when civilians might be considered parties to the conflict.10 In such circumstances, CMR guiding documents suggest complete separation through co-existence.
However, even in complex emergencies, the delivery of aid by a military body may be legally or ethically mandated: the Office of the UN High Commissioner for Refugees’ Guidelines cites Geneva Convention IV and the requirement for an occupying power to ‘supply food and medicine’ and ‘maintain hospitals, and public health and hygiene’.11 Consequently, the IASC argues that guidance must be ‘balanced by sound pragmatism’.10
A changing policy geography: discussion and results
While key guiding documents offer a relatively consistent position regarding the role of militaries, their practicability is increasingly challenged. Experiences in countries like Haiti, Myanmar, Pakistan, Afghanistan and Iraq ‘have all demonstrated continuing weaknesses in civil-military coordination’.12 Furthermore, ‘military and humanitarian actors have consistently failed to reach a common understanding of the role that each plays, the challenges they face and, critically, the priority needs of affected populations and how these can or should be addressed’.12
Crucially, the guidelines have not yet considered five imbricating complexities, which were all raised at the 2017 Chatham House roundtable, namely:
The changing international environment.
Civil-military public health emergency responses.
The assertion of state sovereignty and voice.
Non-military armed groups that are partner to CMR.
A lack of consensus on the ‘principle of last resort’.
These core issues are discussed in turn in the context of the UN CMR guiding documents, in order to robustly explicate these omissions and their consequences.
The changing international environment
The IASC Guidelines establish four mission scenarios (Figure 2), with differing policy frameworks that shape CMR and are adapted to the specific circumstances, mandates and rules of engagement of military actors.5 However, the scenarios raises a number of issues, both in terms of the categorisation of conflict, the actors that are addressed by the frameworks and the propensity for operational environments to experience substantive and dynamic political changes over the course of a protracted public health emergency compared with a natural disaster.10
The reality rarely matches the IASC’s scenarios. For example, the 2004 Aceh Tsunami response placed humanitarians alongside a host-nation military that was both a responder to the crisis and an active participant in a counterinsurgency, akin to UN peace enforcement troops in North Kivu, Democratic Republic of the Congo responding to the ongoing Ebola outbreak there. These responses pose peculiar but increasingly common challenges: one force can be simultaneously subject to a mandate that bridges the IASC Guideline’s ‘peaceful’ and ‘conflict’ mission contexts, posing significant challenges for humanitarian organisations. One recent typology found six unique operational spaces that CMR can exist within and between, including iterations of CMR across and even outside the mission contexts described in Figure 2.13
The guidelines also predate the increasing role of international militaries engaged in governmentally endorsed development work, for example, the United States Africa Command provision of militarised assistance in conflict-prone areas which are also subject to natural disasters. In this area of quasi-war, frequent humanitarian emergencies and state fragility, positioning humanitarian responders in relation to troops is inadequately addressed by existing guidelines.
Civil-military public health emergency responses
The failure to address public health factors or emergencies is a crucial omission and was consistently raised at the 2017 Chatham House roundtable.1 Humanitarian responses in the 1980s and 1990s generally involved assistance to states that lacked significant public health infrastructure. Responses were generally limited to basic and temporary life-sustaining assistance such as evacuations or the provision of trauma care and food packages. However, increasingly assistance is to states which have developed infrastructure essential to public health (eg, power, water, communication and sanitation) with population public health interventions (eg, immunisations and environmental interventions to interrupt parasitic infections). There is also the emergence of ‘pure’ infectious disease emergencies, such as the 2013–2016 West Africa Ebola Epidemic and the ongoing COVID-19 outbreak.
The response to such emergencies includes the maintenance or repair of essential infrastructure, securing or initiating public health programmes and repairing or constructing new healthcare, laboratory and quarantine/isolation facilities.
The breadth of this support requires a cross-sectoral approach, including health, security, economy, education and infrastructure. No one organisation can provide all components, and foreign and domestic militaries have become increasingly involved in supporting various health-related response elements such as coordination, logistics, information management, laboratories and communications, or through tactical interventions by helping secure or supply quarantines, hosting isolation facilities or providing armed escorts for civilian response workers. Crucially, this support is often provided over a sustained period of time, rather than temporary relief in response to a singular natural disaster, involving both militaries and NGOs. Many public health NGOs do not strictly adhere to humanitarian principles, instead choosing context-specific alignment with them. For example, the NGO GOAL Global provided accommodation and facilities to British military troops in the 2013–2016 West Africa Ebola Epidemic. This diversity of position is reflected by many non-UN guidelines: many are concerned with minimising civil-military overlap, some with maximising co-operation and some on addressing specific issues.2
There are ongoing efforts to develop appropriate frameworks that consider public health emergencies, including one by WHO, but this is neither published nor tested, and leaves significant gaps by not addressing the array of non-medical components of a public health emergency response (eg, logistics or coordination) that a military may support. UN OCHA has published a two-page document on understanding UN-CMCoord documents during COVID-19, but is extremely brief and ad hoc: it does not constitute core CMR guidance.14 At best, this reflects a diversity of position and opinion. At worst, this represents ‘inconsistent and contradictory’ stances.5 In short, ‘while simultaneously calling for respect for humanitarian principles, in the recent past many humanitarian organisations have also willingly compromised a principled approach in their own conduct through close alignment with… military activities and actors’.15 This may have been necessary, but is not addressed in guidelines.
The assertion of state sovereignty and voice
The guiding documents are silent on how to align the UN’s mandate to support national governments and the common leadership or inclusion of a host nation’s health authorities in responding to an emergency when foreign militaries are involved alongside domestic military and security services.
The Oslo Guidelines in particular apply to foreign militaries, providing no guidance on relations with domestic militaries, despite being ‘one of the most problematic (CMR) areas…, particularly (in) a conflict in which the domestic military are a party’.9 In such contexts, several dominant civil-military norms such as ‘last resort’ are inappropriate or inapplicable, especially in contexts where partnerships between foreign and domestic militaries exist pre-crisis, or when military support is requested by the sovereign host nation, such as in Sierra Leone’s Ebola response.16 Host-nation requests for military support are particularly problematic to CMR in an environment including a civilian response where the state authority is military.
The legitimacy of the CMR guiding documents are also undermined as the original drafting of the Oslo and MCDA Guidelines included only one sub-Saharan African country between them.7 17 There is therefore a real risk that the guidelines are (or are viewed as) a western construct imposing humanitarian norms on ex-colonies or in inappropriate contexts and ignores the increasing assertion of state sovereignty. This issue was raised by a number of participants from lower-income and middle-income countries at the Chatham House roundtable. Militaries were also excluded, and the guidelines thus enjoy only limited recognition among global militaries. Furthermore, the principle of co-production with potential beneficiaries is notably absent. This calls into question the guiding documents’ relevance to many nations, including those at high risk of experiencing public health emergencies.
Other unaddressed military and security groups
Existing international guiding documents also fail to address numerous other armed groups, such as civil protection and defence groups, private security companies (PSCs) and non-state armed groups (NSAGs). This is particularly problematic when addressing infectious disease outbreaks which requires a response which involves all actors.
Civil protection and civil defence groups
The IASC Global Health Cluster Paper (2011) highlights the absence of an internationally agreed definition of civil defence or civil protection actors relationship(s) with host-nation military forces.10 The profusion of definitions and the increasing reliance on these actors as humanitarian responders has created a need to redefine and reconsider where these fit within the CMR context. Guiding documents should also address ‘where these are civilian actors explicitly operating on the basis of humanitarian principles’ such as with some police and gendarmerie.10
Private security companies
PSCs are increasingly involved in protecting humanitarian staff and facilities, have an increasingly role supporting military forces and are increasingly ubiquitous. Where acceptance, ‘low profile’, and remote programming strategies have failed or are deemed inappropriate, some humanitarian agencies ‘have opted for a deterrence model using armoured vehicles, fortifying offices and hiring armed security’.5 One estimate suggests that all major international humanitarian organisations have used armed PSCs at least once.5 The guiding documents do not address how civilian organisations can appropriately relate to PSCs in public health contexts.11
Non-state armed groups
NSAGs are increasing in numbers and some control territory where civilian and humanitarian organisations operate. Historically, relationships between civilian groups and NSAGs were limited to issues surrounding humanitarian access, but some NSAGs are themselves providers of health and relief assistance, such as the so-called Islamic State’s health services, and direct support to NSAGs has occurred in some relief efforts.16 Relations with NSAGs is complicated by difficulties in identifying the boundary between NSAGs and crisis-affected community leadership. Civilian actors are increasingly engaging with these groups but doing so is fraught with ethical challenges and legal risks exacerbated by developments in counterterrorism legislation, international sanctions, money laundering regulations and domestic legislation which at times contradict international humanitarian law.18 Importantly, militaries involved in public health emergency response may have a concurrent mandate to deter or combat NSAGs, complicating CMR for both military and civilian organisations operating across both domains. Matters are further complicated by the proliferation and dynamism of NSAGs and by occasional and often temporary alliances between militaries and some of these groups. While detailed guidance may be difficult to develop, nonetheless, it is a significant gap which means that current arrangements are ad hoc and legally questionable.
The principle of last resort and the humanitarian imperative
While a recurring theme of guidelines is that of military only as a ‘last resort’, there remain differences between practice and reality, not least because in sudden-onset emergencies, militaries (domestic and foreign) are often first responders simply because they can deploy quickly and the humanitarian need exceeds civilian capabilities. Civilian organisations may be poorly prepared or equipped, or they may choose not to intervene for reasons of cost, risk or politics, or capacity.19 Therefore, compliance with the principle of ‘last resort’ may preclude military support to crisis-affected populations when it is the most practicable, exigent and life-saving resource available. The issue is compounded by ambiguity and confusion in guideline language and interpretation. For example, when guidelines state that ‘military and civil defence assets of belligerent forces engaged in combat shall not be used to support humanitarian activities’,7 they appear to contradict Geneva Convention responsibilities.
Incorporating the principle of ‘last resort’ into national doctrine also differs. For example, Canada and the UK have national CMR guidelines directly informed by the Oslo Guidelines, while Belgium, the Netherlands and the USA’ CMR policies are not, unless requested by OCHA.20 This ambiguity is also reflected in humanitarian positions. At the 30th International Conference of ICRC (2007), the Guidelines for the Domestic Facilitation and Regulation of International Disaster Relief and Initial Recovery Assistance (the ‘IDRL Guidelines’) were adopted. These suggested that ‘military assets should be deployed for disaster relief or initial recovery assistance only at the request of and with the express consent of the affected state, after comparable civilian alternatives have been considered’.21 This is a weaker position than ‘last resort’, and is a divergence from the humanitarian absolutism of the 1990s, even if it is a limited and reluctant embrace.
The principle of last resort is further complicated by the mechanisms for triggering the deployment of military resources. In theory, on the request of a disaster-affected state, a UN Disaster Assessment and Coordination team deploys to conduct an initial needs assessment, including an evaluation for the prospect of military support. However, states, UN agencies and other organisations ‘routinely choose alternative means for channelling military assets’.5 Thus, even requests made through the correct channels may not consider CMR arrangements. This is further complicated in areas of NSAG control, where a Humanitarian or Resident Coordinator holds no practical authority. More challenging is the finding that many key stakeholders are unaware of the guiding documents: for example, one evaluation of the response to the 2004 Aceh Tsunami found that very few actors—civilian or military—knew of the guidelines, and that ‘some “humanitarian actors” by their actions appeared unaware of even the basic concerns regarding association with military forces’.22
Any globally focused guideline will have limited relevance without significant consensus between concerned groups and actors and there is a compelling need to challenge the powerful institutions of humanitarian governance to incorporate other voices in discussions over principles such as ‘last resort’. Ultimately, the principle is arguably impracticable in the dynamic and urgent context of a rapid onset disaster, nor during the fluidity and unpredictability of a protracted public health emergency. Furthermore, it is impracticable when myriad military and security groups intervene with or without invitation, or as deployed by a host-nation government. This reality has largely been accepted by governments and militaries and is increasingly recognised and accommodated among international organisations (IOs) and NGOs.
Conclusion
At times, the existing guidelines, frameworks and guides offer duplicating, imbricating or conflicting guidance; at others, they do not adequately address existing or probable CMR in the context of a health emergency; neither have they kept pace with geopolitical developments. As such, while existing guidelines, frameworks and guides provide utility in many circumstances, none are consistently satisfactory. The myriad CMR guiding documents produced independently by other agencies and militaries do address some of these concerns, but nevertheless, the UN CMR guidelines should, but do not, represent cogent, consistent and aligned principles for CMR in the international arena.
While the guiding documents struggle to appropriately address the new challenges of CMR, their existence undoubtedly serves a purpose, as they should provide a common platform for humanitarian positions. There is evidence of the guidelines beginning to shape the strategic cultures of IOs, including within the UN and European Union which has committed to adherence to the MCDA guidelines, and has affirmed that its ‘capacities must be deployed in a way compatible with the work of humanitarian organisations’.23
However, these processes will remain inadequate for public health emergencies unless the criticisms and gaps of existing UN guiding documents are addressed including the lack of non-Western or military voices in the documents’ drafting process; the difficulty adhering to some humanitarian principles in an increasingly dynamic and complicated space; a lack of consideration for the increasing assertion of state sovereignty or for different professional and regional cultures; geopolitical developments including the increase in NSAGs and legal developments such as in counterterrorist legislation and the confusing, overlapping nature of the guidelines themselves.1 Specific consideration is required for public health emergencies as a distinct phenomenon and consideration for various relevant actors. These gaps are compounded by a poor consensus regarding the ‘principle of last resort’, a lack of awareness or understanding of the guidelines by key actors, and by the proliferation of specifically public health emergencies.
Existing UN guiding documents must either be revised, or new documents created, which include public health requirements. While the 2018 IASC Recommended Practices for Effective Humanitarian Civil-Military Coordination of Foreign Military Assets in Natural and Man-Made Disasters represents an attempt to create new and practicable guidance, it still does not centrally consider or address any of these issues.24 Given the increasing complexity and frequency of situations that involve concurrent civilian and armed-actor responses, a viable alternative may be to move away from guideline or guideline-type documents altogether, and to identify a set of internationally agreed principles against which civil-military cooperation can be planned and assessed for each specific operation and intervention. Developing principles may also overcome the argument that seeking to revise international documents that took significant effort and compromise to develop is a major and perhaps inadvisable process. UN OCHA’s October 2014 briefing document Civil-Military Interaction and the Use of Foreign Military and Civil Defence Assets (MCDA) in the Context of the Ebola Crisis in West Africa is short, does not include a number of the gaps identified here, and is limited to only one operational context, but does indicate that the agency is prepared to address their global guidance according to new developments and concepts.25 Similarly, while only two pages long and therefore extremely nascent in development and adoption, their March 2020 briefing document on CMR during COVID-19 ‘considers lessons observed from the SARS outbreak in 2002–2003 and the Ebola outbreak of 2014, among others’ and is therefore further promising indication of willingness to substantively engage this discussion.14
In short, while it is inevitable that this complicated space will remain controversial and key elements of CMR guidelines will remain contested, it is crucial that these criticisms and gaps are considered and addressed in future CMR guideline and framework dialogue, revisions and development.
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study.
Ethics statements
Patient consent for publication
Footnotes
Twitter @samuelboland, @LLillyhwite
Contributors STB was primarily responsible for manuscript writing and revisions. CM and SG assisted with drafting and initial research development. LL was the primary focal point for guiding the writing process, and also assisted with (re)drafting and editing throughout the development of this manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests L Lillywhite is also Master-General of the Army Medical Services, but this contribution is in his role at Chatham House.
Provenance and peer review Commissioned; externally peer reviewed.