Article Text

Abstract
Introduction Side plates are worn by UK Armed Forces as part of the VIRTUS body armour and load carriage systems to protect the thorax and abdomen from high-velocity threats. The VIRTUS project has provided the impetus to objectively demonstrate the anatomical coverage provided by side plates.
Method CT scans of 120 male UK Armed Forces personnel were analysed to ascertain the vertical distance between the anterior axillary fold and iliac crest, and horizontal distance between anterior and posterior borders of the liver, delineating the boundaries of essential medical coverage from the side aspects. The percentage of shot-lines intersected by the existing Enhanced Combat Body Armour (ECBA) plates as well as an optimised plate based on the maximum potential dimensions of essential coverage was determined in the Coverage of Armour Tool.
Results ECBA plates were 101 mm shorter and 4 mm narrower than a plate with dimensions providing essential medical coverage for the 50th percentile subject (157×315 mm). Coverage increased by 35% when using two ECBA plates as side coverage in addition to using the front and rear OSPREY plates in the VIRTUS vest. Two side plates with dimensions providing essential medical coverage for the 50th percentile increased anatomical coverage by a further 16%.
Conclusions This analysis has provided strong evidence that ECBA plates are already optimised for side protection, despite not being originally designed for this purpose. They are correctly positioned within the VIRTUS soft body armour vest and the width of the ECBA plate is only 3% less than what would be optimum size for the 50th percentile. Although the height of the plate could be increased to further enhance the anatomical coverage, it is unlikely that this would be acceptable in terms of the human factors, equipment integration or additional mass.
- side
- plate
- protection
- ballistic
- armor
- anatomy
- coverage
- military
Data availability statement
No data are available.
Statistics from Altmetric.com
Key messages
Side plates are worn as part of body armour and load carriage systems to protect the thorax and abdomen from high-velocity threats.
The position of current Enhanced Combat Body Armour plates within the VIRTUS vest are already optimised for side protection, despite not being originally designed for this purpose.
Although side plate height could be increased, this would likely be unacceptable in terms of the human factors, equipment integration or additional mass.
Introduction
Historical development of side protection
Body armour is a type of equipment worn by military personnel that aims to prevent or reduce the damage caused by ballistic projectiles penetrating structures within the thorax and abdomen.1 Such injuries remain the leading cause of potentially survivable deaths on the modern battlefield.2 The vast majority of modern military body armour systems use two differing components to defeat the penetration of ballistic projectiles.3 The ‘soft armour’ is a flexible woven fabric (usually a para-aramid such as Kevlar or Twaron) or ultra high molecular weight polyethylene (such as Dyneema or Specra or a combination of these materials) that covers the thorax and abdomen and is designed to stop explosively propelled fragments. ‘Hard armour’ was introduced to UK Armed Forces in the late 1970s with the introduction of the Mark II plate which was used with the Improved Northern Ireland Body Armour (INIBA) soft body armour vest. This plate was subsequently modified to become the Enhanced Combat Body Armour (ECBA) plate. Hard armour is designed to defeat high-velocity bullets and is usually fulfilled by ceramic-faced and composite-backed plates worn in pockets on the front and rear of the soft body armour outer carrier. Wearing side plates in OSPREY vests started on operations in Iraq in 2007, when, after some UK Armed Forces personnel were injured in the flank, serving personnel started to innovate with their own equipment, and slid an ECBA plate into each side of their OSPREY Mark 1 vest cover (Figure 1A).

Side plates were slid into the vest of OSPREY Mark 1 (A), held in a cummerbund on the outside of OSPREY Mark 4 (B) and in a separate plate pocket in OSPREY Mark 4A (C).
As a result, the use of ECBA plates as side plates was formally adopted in subsequent iterations of OSPREY. Indeed, the most recent iterations of the OSPREY system issued towards the end of the Afghanistan conflict incorporated the ECBA plates held in a cummerbund that was worn on the inside of the soft armour (Figure 1B). Subsequently detachable side pockets that attached to the OSPREY cover were introduced in the Mark 4A Vest (Figure 1C). The first iteration of the VIRTUS personal armour and load carriage system was issued to UK Armed Forces in Autumn 2015. It uses the same (ECBA) side plates as in OSPREY, and the side plates are also positioned in the same location on the soft armour vest (Figure 2).

VIRTUS vest without (A) and with side plate in holder (B). Plate dimensions (C) comprise height (1) and width (2).
Essential thoraco-abdominal medical coverage from the sides of an individual
UK multidisciplinary consensus has recommended the structures in the thorax and abdomen that require coverage; these are the heart, aorta, superior and inferior vena cavae, liver and spleen.3 Essential coverage for side plates should be the same anatomical structures as for the front and rear plates (ie, aortic arch to aortic bifurcation). However, this is currently not possible to achieve due to the human factors challenges of using a plate in this area. For side plates, the upper border is intrinsically limited by the anterior axillary fold of the pectoralis muscle. Deformation of this muscle such as by a plate would prevent arm movement.
Sizing and fitting of plates to surface anthropometric landmarks
The most superior and inferior points of essential side medical coverage (anterior axillary fold to aortic bifurcation) for front and rear plates can be related to the anthropometric landmarks of the suprasternal notch and upper border of the iliac crest, respectively.3 Anthropometric surveys of Armed Forces personnel have the potential to provide data to size and scale body armour to an individual.4–8 The largest and most comprehensive anthropometric study of UK Armed Forces personnel to date was undertaken by QinetiQ, and measured 2159 male subjects, of which 1395 were Caucasian and 924 of these were Army or Royal Marine personnel.6 However, the only relevant value in these existing anthropometric surveys in terms of anthropometric landmarks for side plate coverage is ‘Axilla height while standing’. However, as the surveys did not measure any other landmark from which side plate coverage could be determined or secondarily derived from other landmarks (ie, iliac crests), then this value cannot be determined using measurements from existing anthropometric surveys.
Objective methods of comparing coverage provided by different plate designs
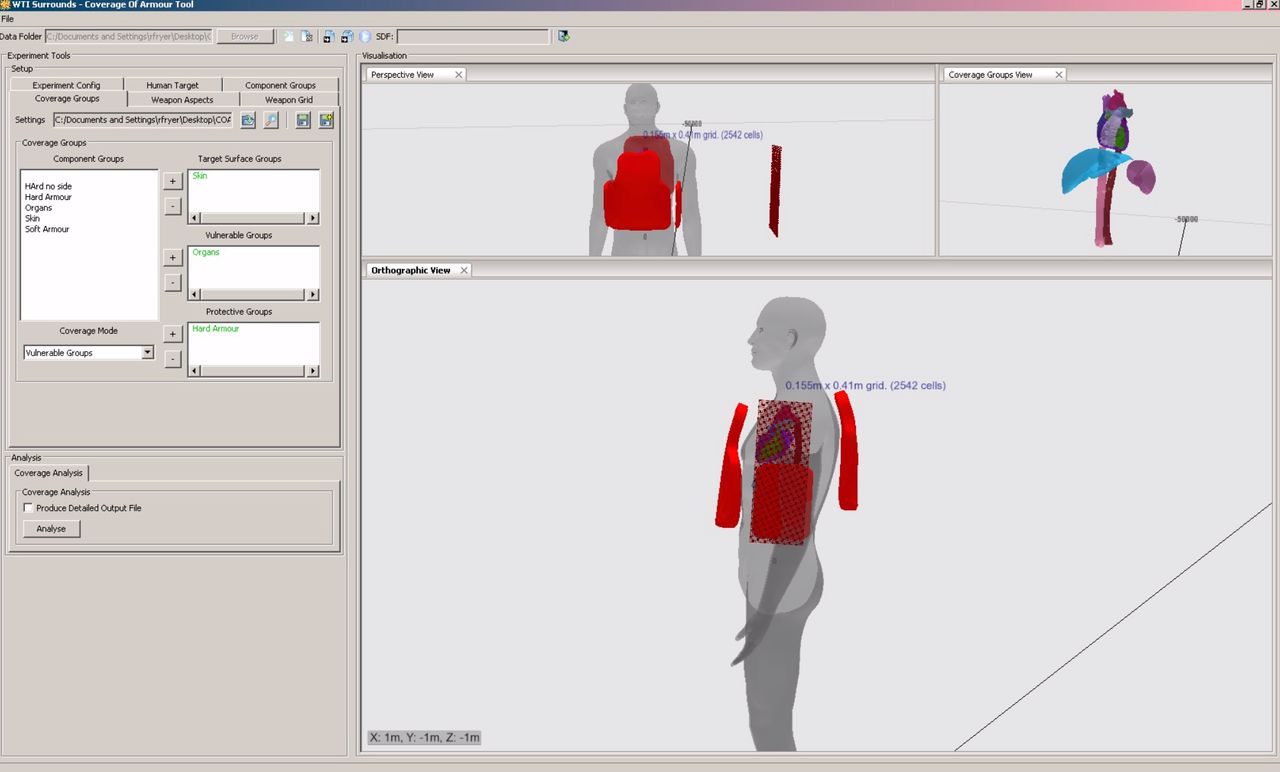
The Coverage of Armour Tool (COAT) is a geometrical analysis capability designed to objectively compare the coverage of different designs of body armour.9 It is based on the ‘Zygote’ model, in which the surfaces of anatomical structures are represented as a mesh with a fidelity down to 0.5 mm, having originally been derived from CT scans of healthy participants. Any design of body armour can be incorporated into the tool and overlaid onto these anatomical structures, either from a three-dimensional laser scan or by importing a computer-aided design file into the tool (Figure 3). COAT uses the concept of a ‘shot-line’ analysis, where projectiles are assumed to be fired from outside the body and pass through the body in an infinitely thin straight line. A mesh of these shot lines, with 2 mm spacing between them, is superimposed over the vulnerable anatomical structures. The origin of the shot lines can be altered about the participant in the horizontal (azimuth) and vertical (elevation) planes to represent different attack vectors. For example, in the horizontal plane, zero degrees corresponds to a shot-line originating from in front and 180 degrees from the rear. In the vertical plane, zero degrees represents the shot-line being directed horizontally and −90 degrees as if the projectile was directed from the ground travelling in an upwards trajectory. The direction of the shot-lines is based on best available evidence from recent conflicts in conjunction with the position that the soldier is likely to be assuming for different roles. For example, a soldier patrolling could be hit by a high-velocity bullet from any azimuth, but it is relatively unlikely that it would originate from significantly below or above the target.
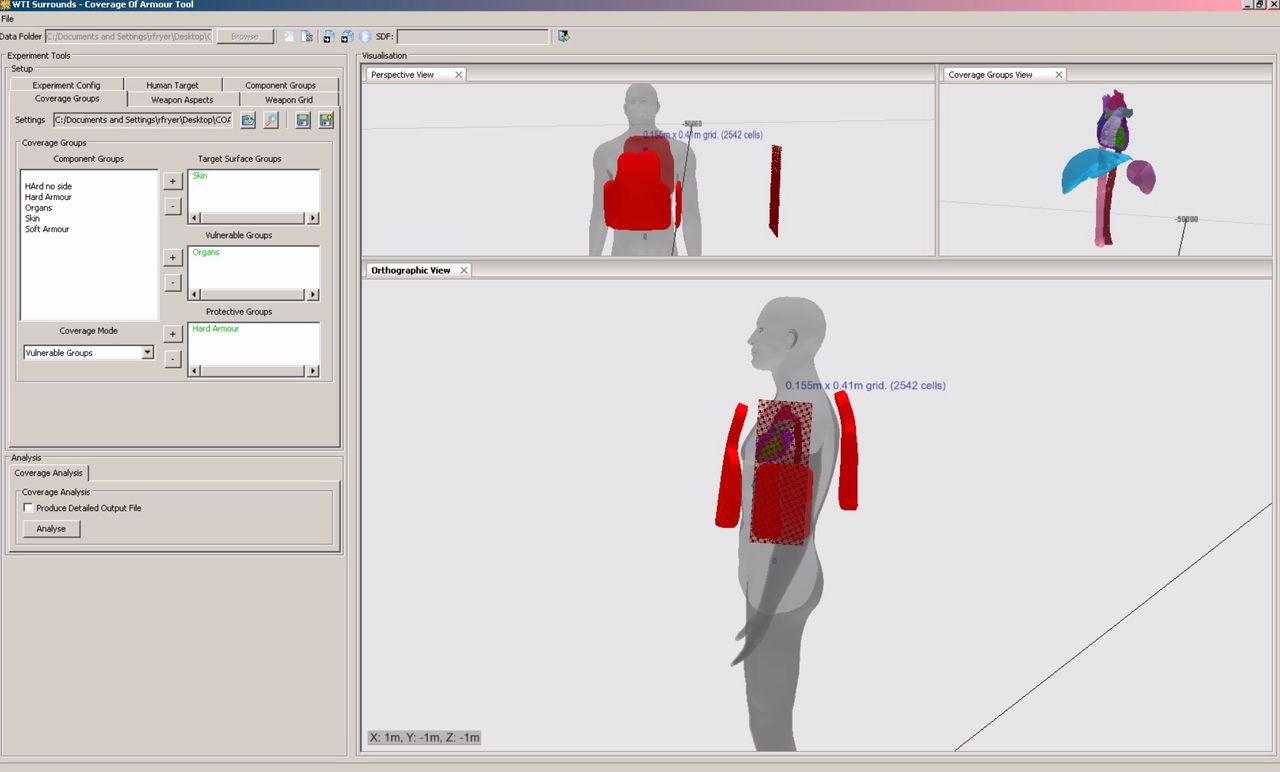
Screenshot of the Coverage of Armour Tool (COAT) being used to ascertain the essential medical coverage provided by the side plate in the OSPREY body armour system.
Aims of this research
To use CT scans to determine the dimensions of essential medical coverage for side coverage in a representative male Armed Forces population.
To use COAT to objectively compare the anatomical coverage afforded by ECBA plates and a prototype plate and to quantify how much additional coverage to essential medical structures is afforded by front, rear and side plates.
Method
Analysis of 120 CT scans to determine the dimensions of essential medical coverage from the side
Contrast CT ‘trauma’ scans of 120 consecutive UK Armed Forces personnel evacuated to the Queen Elizabeth Hospital Birmingham between 17 June 2009 and 19 March 2013 were analysed. These scans were taken as part of the trauma call protocol for all injured service personnel in Afghanistan as part of their initial assessment. Analysis of these scans was approved by the Medical Directorate of the Defence Medical Services.
Scans were excluded if there was any damage to structures within the thorax or abdomen as well as any in whom stature information was not available. To increase the statistical strength of any conclusions made, only scans of male Caucasians were used.
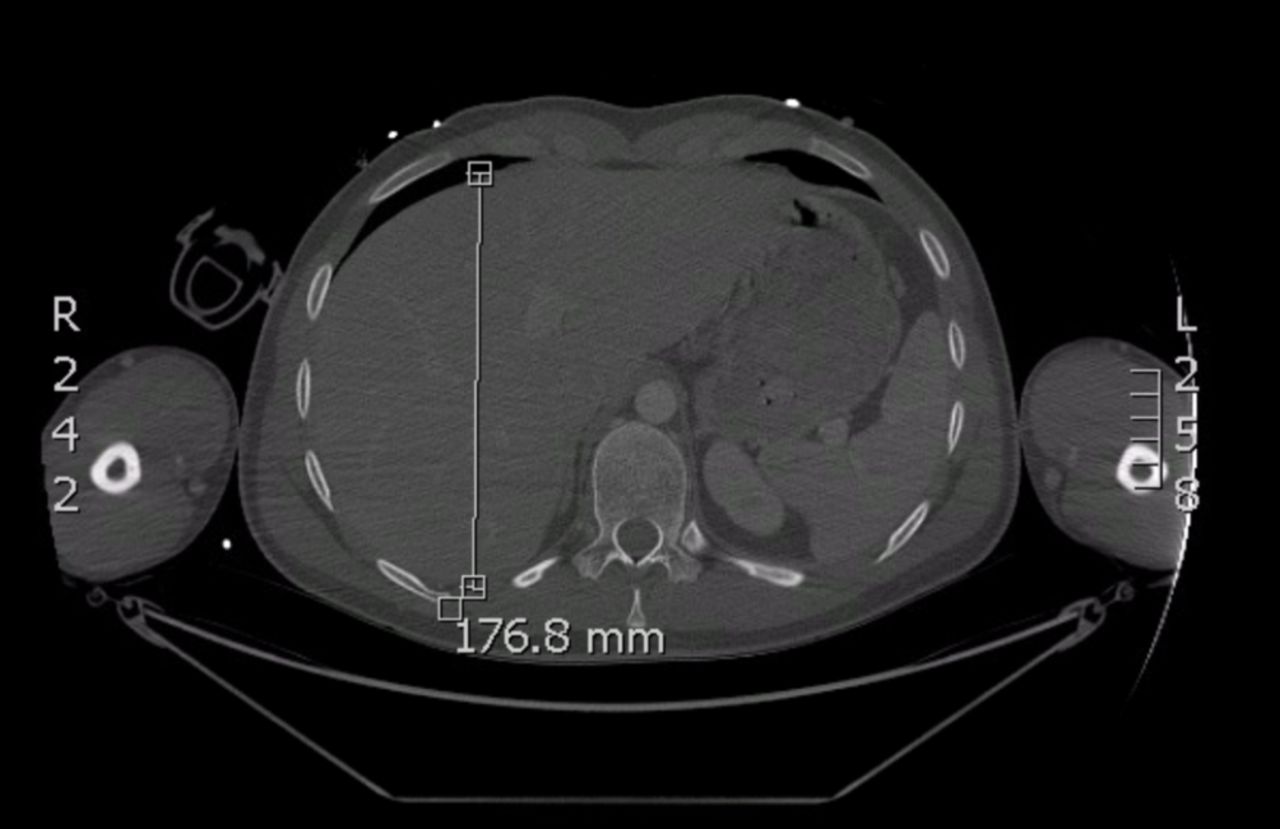
Essential vertical coverage (plate height) was determined by measuring the distance between the superior border of the iliac crest (lower border, Figure 4) and the anterior axillary fold (Figure 5). The width of the upper border of essential horizontal coverage (upper plate width) was determined by measuring the maximal distance between the anterior border of the heart and the posterior border of the aorta at the level of the anterior axillary fold (Figure 5). The width of the lower border of essential horizontal coverage (lower plate width) was determined by measuring the maximal anteroposterior depth of the liver in the axial plane (Figure 6).
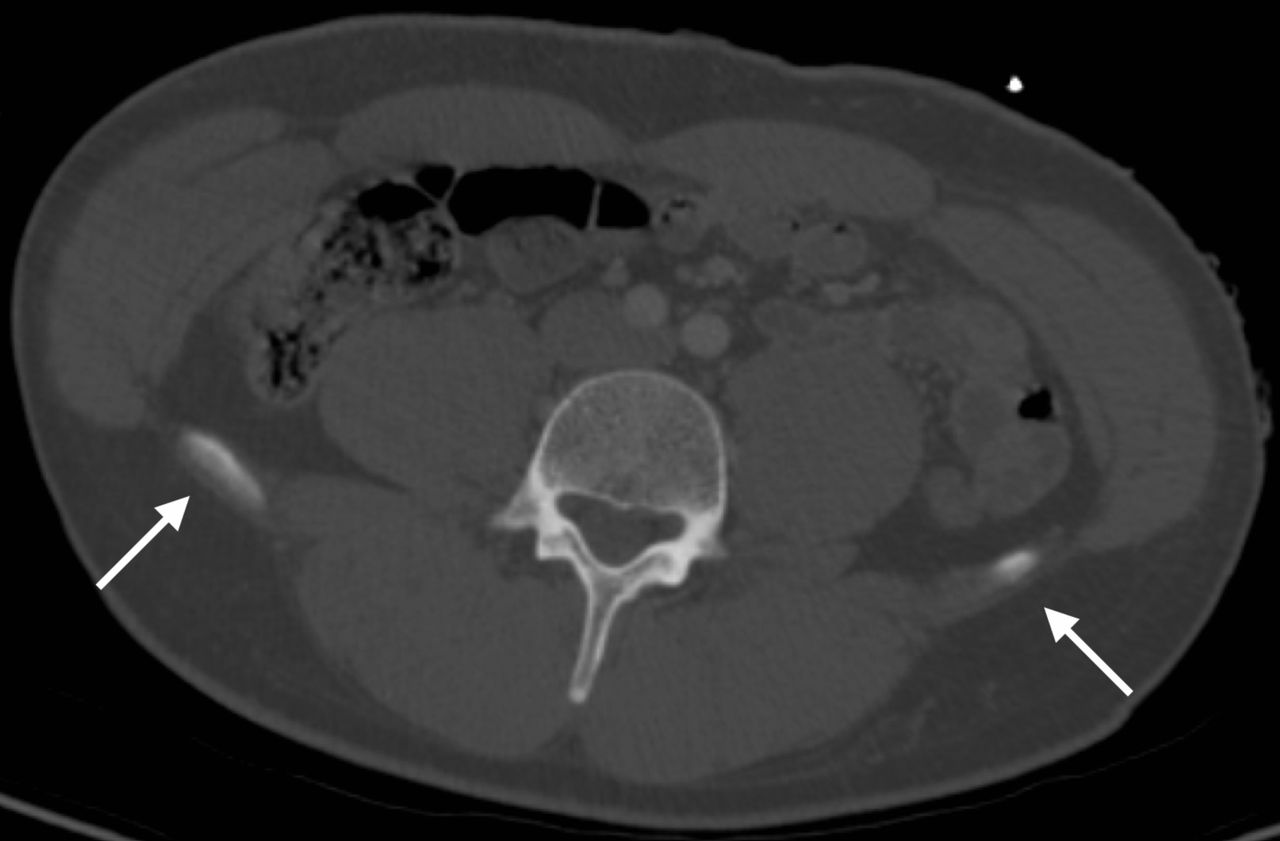
Lower boundary of side coverage at the level of the superior border of the iliac crests (arrowed) visualised on CT in axial section.

Upper boundary of side coverage at the level of the right anterior axillary fold (arrowed) visualised on CT in axial section. P, pectoralis major. Upper plate width was determined by the maximal anteroposterior distance between the anterior border of the heart to posterior border of aorta.
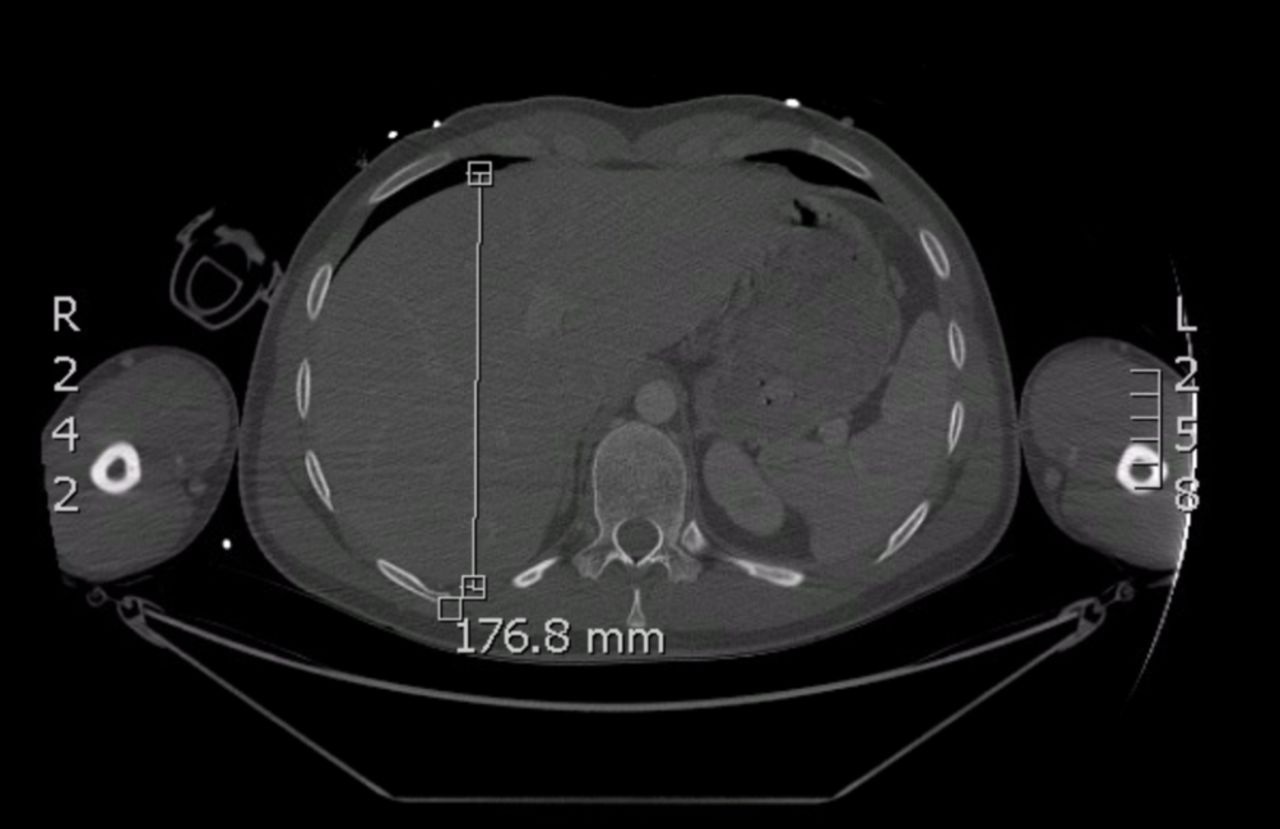
Lower plate width was determined by the maximal anteroposterior depth of the liver in the axial section.
Use of Zygote model to determine the optimal positioning of side plates within the VIRTUS vest
The anatomical structures comprising essential medical coverage were identified within the Zygote model. The ECBA plate as it currently sits within the VIRTUS vest was superimposed on the bifurcation of the aorta, which represents the lower border of essential medical coverage.
COAT analysis to determine the coverage of vulnerable anatomical structures provided by combinations of front and side plates
The following anatomical structures defined as essential medical coverage were identified within COAT: heart, aorta, super and inferior vena cavae, liver and spleen. The front and rear OSPREY plates as positioned within the VIRTUS vest were superimposed on these structures and coverage of these structures determined (Table 1). Both current ECBA side plates were subsequently superimposed and further coverage determined. Finally, a side plate was designed within the tool with a height and width based on the dimensions of essential coverage determined from the 50th percentile within the CT scan analysis. Coverage was determined in all cases in a 360-degree horizontal (azimuth) plane and from −30 to +30 degrees elevation (Figure 7).
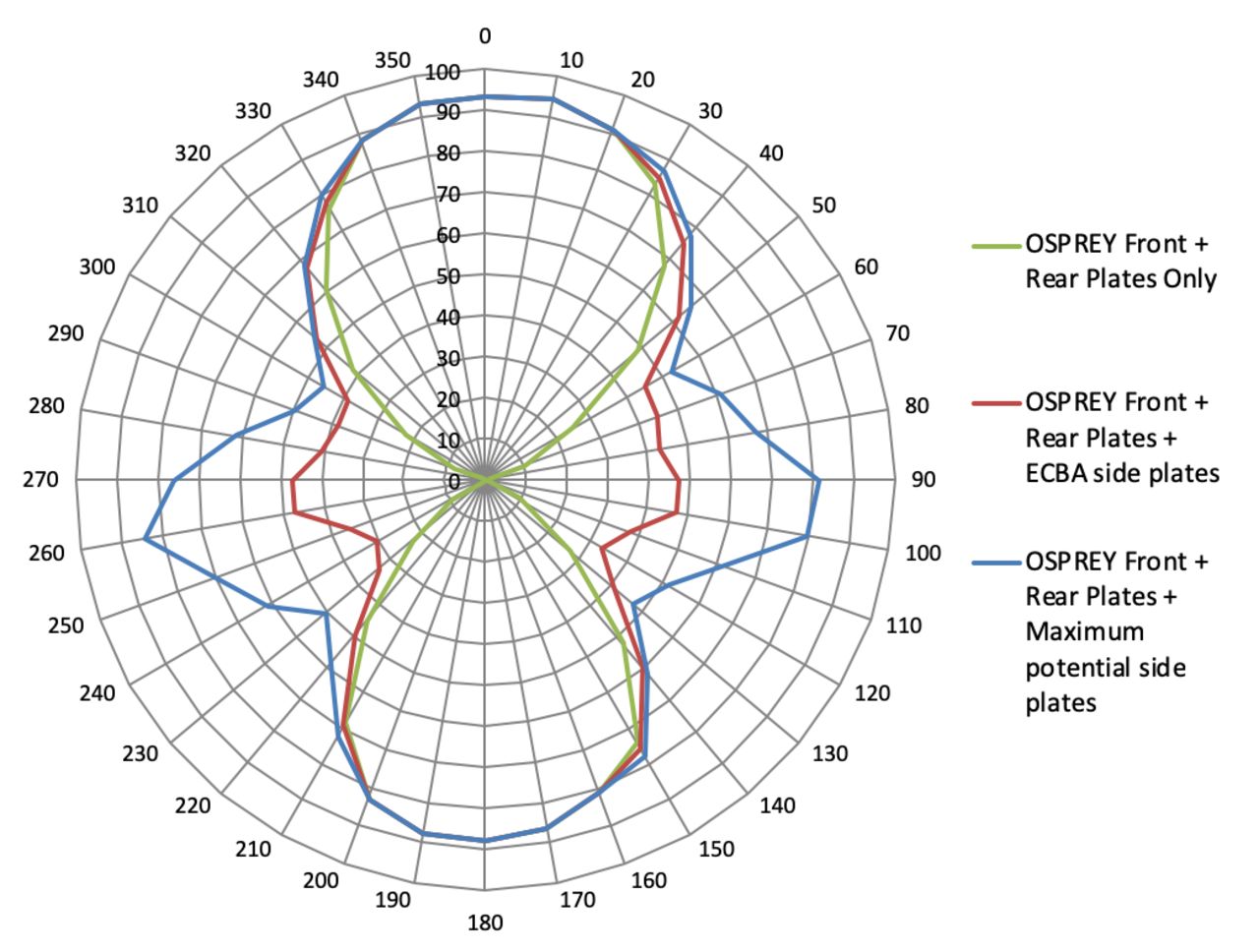
Results from Coverage of Armour Tool azimuth plot analysis to determine the different percentage coverage of anatomical structures comprising essential medical coverage within the thorax and abdomen

Azimuth plot demonstrating the coverage of anatomical structures comprising essential medical coverage using front and rear plates alone, additional current side plates and optimised side plates. Green, front and rear only; red, additional side plates; blue, additional maximum side plates.
Analysis of these scans was approved by the Royal Centre for Defence Medicine (approval reference: 1036.16.0456) and University Hospital Birmingham (approval reference: CARMS-15201).
Results
Analysis of 120 CT scans to determine the dimensions of essential medical coverage from the side
Subjects analysed ranged between 18 and 46 years old at the time of injury, with a mean body mass index of 24.8. The anterior axillary fold and iliac crest were visible in all 120 scans (Table 2). The lower border of the ECBA plate lies on the iliac crest, and therefore is correctly positioned for providing the lower border of essential medical coverage. The width of essential coverage was measured as 157 mm for the 50th percentile, 4 mm (3%) less than the ECBA plate. The height of the ECBA plate of 214 mm is 101 mm (47%) less than that required for essential medical coverage for the 50th percentile based on CT.
Results of vertical distances between anthropometric landmarks ascertained from 120A CT scans of male UK Armed Forces personnel (in millimetres)
Use of Zygote model to determine the optimal positioning of side plates within the VIRTUS vest
When side plates are placed in the pockets of the VIRTUS vest as visualised in the Zygote, the lower border of the plates lie at the same horizontal position as the bifurcation of the aorta. This is the lowest border of essential medical coverage; therefore, the current ECBA plates are already in the optimum position (Figure 8).

Geometric anatomical representation scaled to a 50th percentile male member of the UK Armed Forces; structures comprising essential medical coverage (left), current ECBA plate (middle), a theoretical plate with maximal dimensions (right).
COAT analysis to determine the coverage of vulnerable anatomical structures provided by combinations of front and side plates
When the front and rear OSPREY plates were inserted into the VIRTUS soft armour vest, the COAT analysis demonstrated that this provided 46% coverage of the anatomical structures defined as essential to cover. The addition of ECBA plates to provide side coverage increased the coverage to the essential anatomical structures by an additional 35% for the 50th percentile. A theoretical medically optimised plate, extending the coverage to the outer borders of the anatomical structures defined in essential medical coverage for the 50th percentile (157×315 mm), increased coverage by a further 16% (Table 1).
Discussion
ECBA plates have been used to supplement the protection in the side of the body armour vests since 2007. Although this was instigated as a ‘quick win’ for the threat at the time by OSPREY body armour users in Iraq, it was acknowledged that ECBA plates provided an acceptable solution for side plates, and body armour vests were optimised accordingly. The use of ECBA plates as side protection was carried over into the VIRTUS body armour and load carriage system, but coverage analysis was never undertaken to quantify the additional coverage of anatomical structures that they provide.
The Zygote model was used to determine how well positioned the current ECBA side plates are within the pockets of the VIRTUS soft body armour vest, with respect to the anatomical structures defined as requiring coverage. The lower border of the ECBA side plates was shown to lie on the iliac crests, an anthropometric landmark for the bifurcation of the aorta, which in turn corresponds to the lower point of essential medical coverage. Therefore, this analysis has showed that the ECBA as side plates are already in the optimum position and no amendments are required.
CT scans of representative service personnel were used to determine the dimensions of essential medical coverage from the side aspect and were compared with the dimensions of the ECBA plates. The width of the current ECBA side plate is almost identical to that required for essential medical coverage. For the 50th percentile male in this study, the ECBA plate is only 3% less than the actual width required to cover all the essential anatomical structures. Therefore, there is minimal justification to alter the width of the current plate.
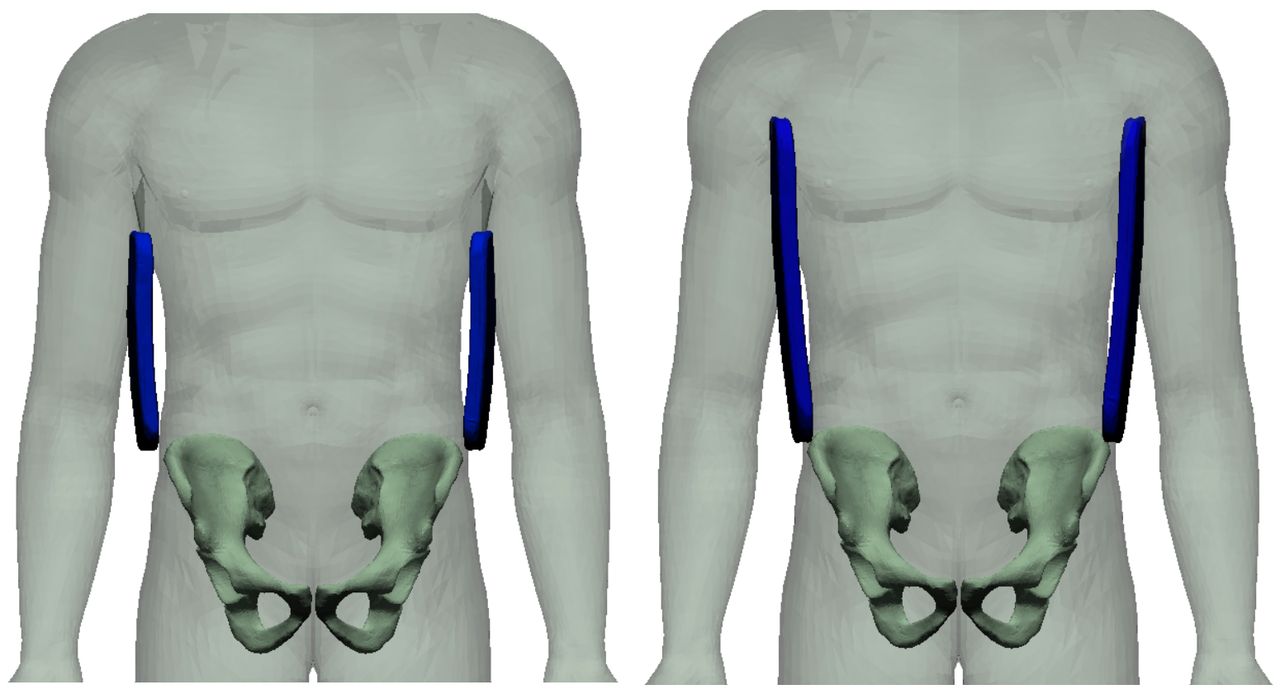
The height of the ECBA plate is 47% less than that required for essential medical coverage if based on a 50th percentile male. This, however, must be taken in context; in that if a side plate was to be positioned as high as the axillary folds, it would be highly unlikely to be acceptable in terms of human factors and equipment integration (Figure 9).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Zygote model (scaled to the 50th percentile) demonstrating the fit and position of the plates. ECBA plate (left), theoretical maximal plate (right).
The COAT tool was used to determine the percentage coverage provided by the combinations of front and rear OSPREY plates and the subsequent percentage increase in coverage provided by incorporating the ECBA plates as side protection. ECBA plates increase the coverage to the anatomical structures defined as essential to protect by 35% over the front and rear OSPREY plates alone. If the size of side plates increased to the outer borders of medical coverage for a 50th percentile male, this would increase the percentage coverage by a further 16%. This COAT analysis was based on the assumption that a projectile might hit the body at any angle equally likely as one another. However, in reality, it is likely that more shots would occur from the front of an individual than from the sides or rear. Currently, however, there is little evidence to support this. Gofrit et al demonstrated that 94% of bullet hits to the torso in the Lebanon war were to the front of an individual.10 It is therefore recommended that damaged armour returned from combat operations in Iraq and Afghanistan are analysed to assist with predicting the shot angulation at the time of impact, in conjunction with surface wound mapping analysis of gunshot wounds to the thorax and abdomen in this cohort.
Conclusions
This analysis has provided strong evidence that ECBA plates used as side protection already provide excellent coverage to the structures defined as essential medical coverage. This is despite the fact that ECBA plates were procured for front and rear protection and were not originally envisioned to be used for the purpose of providing side protection. They are correctly positioned within the VIRTUS soft armour vest and the width of the plate is only 3% less than what would be considered the optimum width for the 50th percentile male. Although the height of the plate could be increased enhance the coverage further, it is unlikely that this would be deemed acceptable for human factors and equipment integration reasons or the for additional plate mass likely to be incurred. Even were it acceptable in terms of these factors, the maximal height for a 50th percentile male would only provide a further 16% increase in coverage of the anatomical structures.
Data availability statement
No data are available.
Footnotes
Contributors JB, EL and RNF are all responsible for the production and reporting of this paper.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.