Article Text

Abstract
Background The COVID-19 pandemic has presented many countries with significant health system and economic challenges. The role of civil–military cooperation in a health crisis of the magnitude presented by COVID-19 remains virtually unexplored. This review aims to detect and identify typologies, if any, of associations between security or military systems and the national response measures during the COVID-19, as adopted by six European countries during the early phase of the outbreak (January to March 2020).
Methods We designed a structured qualitative literature review (qualitative evidence synthesis), primarily targeting open-source grey literature using a customised Google web search. Our target countries were UK, France, Spain, Italy, Belgium and Sweden. We employed a ‘best fit’ framework synthesis approach in qualitative analysis of the result records.
Results A total of 277 result records were included in our qualitative synthesis, with an overall search relevance yield of 46%. We identified 19 distinct descriptive categories of civil–military cooperation extending across seven analytical themes. Most prominent themes included how military support was incorporated in the national COVID-19 response, including support to national health systems, military repatriation and evacuation, and support to wider public systems.
Conclusion Findings of this review show the significance of military systems in supporting an expansive response during the COVID-19 pandemic, and our proposed methodological approach for capturing military health data in a reproducible manner and providing a comparative view on common types of interventions provided by civil–military cooperation to inform lessons from the use of military capacities during current COVID-19 outbreak.
- health policy
- public health
- COVID-19
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
This paper analyses the role of armed forces in response to the COVID-19 pandemic, based on case studies of six European countries.
We identified 19 distinct categories of civil–military cooperation across seven main analytical themes.
Results from Italy and Spain showed the highest range and frequency of civil–military cooperation categories.
Sweden showed the lowest range and frequency of civil–military cooperation categories.
The COVID-19 crisis has shown that the armed forces and military medical services should be considered as key components of national resilience.
Introduction
The topic of civil–military relations during public health emergencies has tended to focus on the relationship between international armed forces (including military medical services) and humanitarian actors on overseas intervention operations.1 While there has been increased emphasis on the importance of national resilience and civil preparedness as a component of national security, this has been perceived to be a civilian responsibility with military support as a last resort.2
The COVID-19 pandemic has presented many countries with significant challenges and extensive system-wide effects across their society. Both public and private health sectors seemed to have been overwhelmed, especially in countries worse hit by the virus or in resource-constrained settings.3–5 In some countries, the response to the outbreak during the spring of 2020 was believed to alleviate part of this strain, especially on healthcare services. However, the displacement effect of common lockdown measures has left the global economy destabilised. Baseline economic forecast from the World Bank envisions a 5.2% contraction in global gross domestic product throughout 2020, with many countries already being pulled into economic recessions.6 As countries navigate their way through this global health crisis, the expectation is that the global response to COVID-19 may benefit from stronger coordination and information sharing, both across geographies and disciplines.7
In Europe, national decision-makers sought to engage with various domestic and regional stakeholders to respond to the threats posed by the outbreak. Policy responses have extended beyond health interventions.8 Notable examples include the private sector scaling up manufacturing of personal protective equipment and ventilators9; and the military or security sector support to healthcare interventions and implementation of national COVID-19 measures such as enforcing lockdowns and maintaining public order.10–13 This cooperation was also evident across countries in the form of international aid relief, regional fiscal policies and mutual assistance to deployment of front-line healthcare resources. Such multisectoral cooperation allowed governments to provide a rapid and extensive response to meet urgent system needs.14
Putting aside issues of COVID-19, the role of military health systems in contributing to population health and the domestic health policy tends to be poorly understood.15 It is often viewed as a distinct entity from the civilian health system, though the armed forces and wider security services could play a greater role in global health and national public health.16 17 The ALMANAC Military Medical Corps Worldwide collates some data on military health systems; however, the depth and quality of the information is insufficient for international comparisons.18 With the exception of complex emergencies linked to humanitarianism and peace-keeping efforts, it is often neglected from mainstream global conceptualisations such as United Nations development system or WHO health system building blocks.19 20 Nevertheless, in many countries, the security or military health system is substantive. This is true across many domains such as budget, size (number of facilities, staff), throughput (number of patients, population served) and endowment (higher than usual availability of high-performance diagnostic and therapeutic equipment, medicines and consumables).21 The research that has been done on the Ebola outbreak in West Africa (2014–2016) emphasised the importance of military support in health provision to national population during epidemics. However, it is suggested that whatever cooperation occurred at the peak of the outbreak may have not been taken forward, in spite of the increased profile of the global health security agenda.22–25 As a result, the nature of civil–military cooperation in a health crisis of the magnitude presented by COVID-19 remains virtually unexplored.
This paper describes a structured methodological approach to explore and classify the role of armed forces and military health systems in national responses to health crises with an emphasis on data not otherwise captured in academic literature. We aim to detect and identify typologies, if any, of associations between armed forces and the national response measures during the COVID-19, as adopted by various European countries during the early phase of the outbreak (January to March 2020). This is done to create a taxonomy of potential military interventions to aid comparisons between countries. Understanding how such civil–military cooperation unfolds during the response to COVID-19 can provide valuable insights for policymakers into potential pathways for closer integration of otherwise parallel subnational health systems which nevertheless work towards the same aim. This might also be of significant importance for better international coordination of efforts to mitigate further health crises.
Methods
Design
We designed a structured qualitative literature review (qualitative evidence synthesis), primarily targeting open-source grey literature using a customised Google web search. Grey literature provides information which is produced on all levels of government, academics, business and industry. It also provides a potential viable source for military health information released by authorities that are not otherwise captured in academic literature.26 Our methodological design choices were further reinforced by two main premises. First, the objective of this study would only be met if the paucity of information available on the topic in academic databases could be mitigated by detection and collation of other public sources of information. Second, acknowledging the social nature of this study, it was thought that using a popular web search engine as Google evaluating the digital presence of military health information on public web pages may give us an idea about the relative prominence of the topic reported in each country.
Godin et al 27 highlight some inherent limitations in using Google search algorithms for literature review. These were mitigated by taking measures to standardise our method for easier multiresearcher reproducibility of results and by a review of a sample of each of the search results by a second reviewer to minimise selection bias. A standard ‘step-by-step search instructions protocol’ was developed and consistently used. This included using Google search by a generic access point (non-user defined), setting search language to native language of respective country, following exact order of insertion of search terms and adjusting search settings in Google search to display results by respective local geographical regions. More information on the search strategy is available in online supplemental material.
Supplemental material
We carried out two preparatory search rounds on eight countries on 21 April 2020. These rounds enabled us to design our study by testing various search techniques and consequently developing a search strategy suitable for our study objectives. This included refining the search criteria, time horizon, search language and target countries.
Target countries
Six European countries emerged as suitable candidates during our preparatory search rounds. These were the UK, France, Spain, Italy, Belgium and Sweden. These countries did not just show potential availability of military health information, but were also the top six European countries with the highest COVID-19 excess mortality rate reported by the Johns Hopkins University Mortality Analysis on 8 July 2020 (date range: 28 January to 21 March 2020).28
Search criteria and data sampling
A custom Google search was conducted for each of the six target countries. The search terms were: ‘name of the respective country’, ‘COVID-19’, ‘military’, ‘Army’ and ‘Security’. Our preparatory search rounds indicated that the order of search results in Google may vary at each instance of search attempt. Therefore, it was decided to conduct a single search for each country and to extract the full data set from the search results in a single ‘sitting’. To standardise the search process, it was decided to select an initial sample of the first 120 result records per country to provide a maximum of 100 records for analysis per country. This threshold was set based on observing the decay in the relevance of result records detected in preparatory search rounds. This number was considered to be exhaustive enough to ensure we included all potentially relevant results in our initial sample. The resultant records were then subsequently accessed, translated (using Google Translate), summarised and then extracted into a Microsoft Excel sheet. This was done noting record’s publication date, short description, category of response and a weblink to the record source. The exact search strings with search terms used for each of the six target countries are available in online supplemental material. The online Google searches were set to consider records that were published between 20 January and 21 March 2020. The time frame was chosen to detect military involvement during early phase of the global pandemic. The date of publication of all records was noted to enable a time analysis of the findings. The actual search was undertaken during the week beginning Monday, 15 June 2020.
Data extraction and eligibility criteria
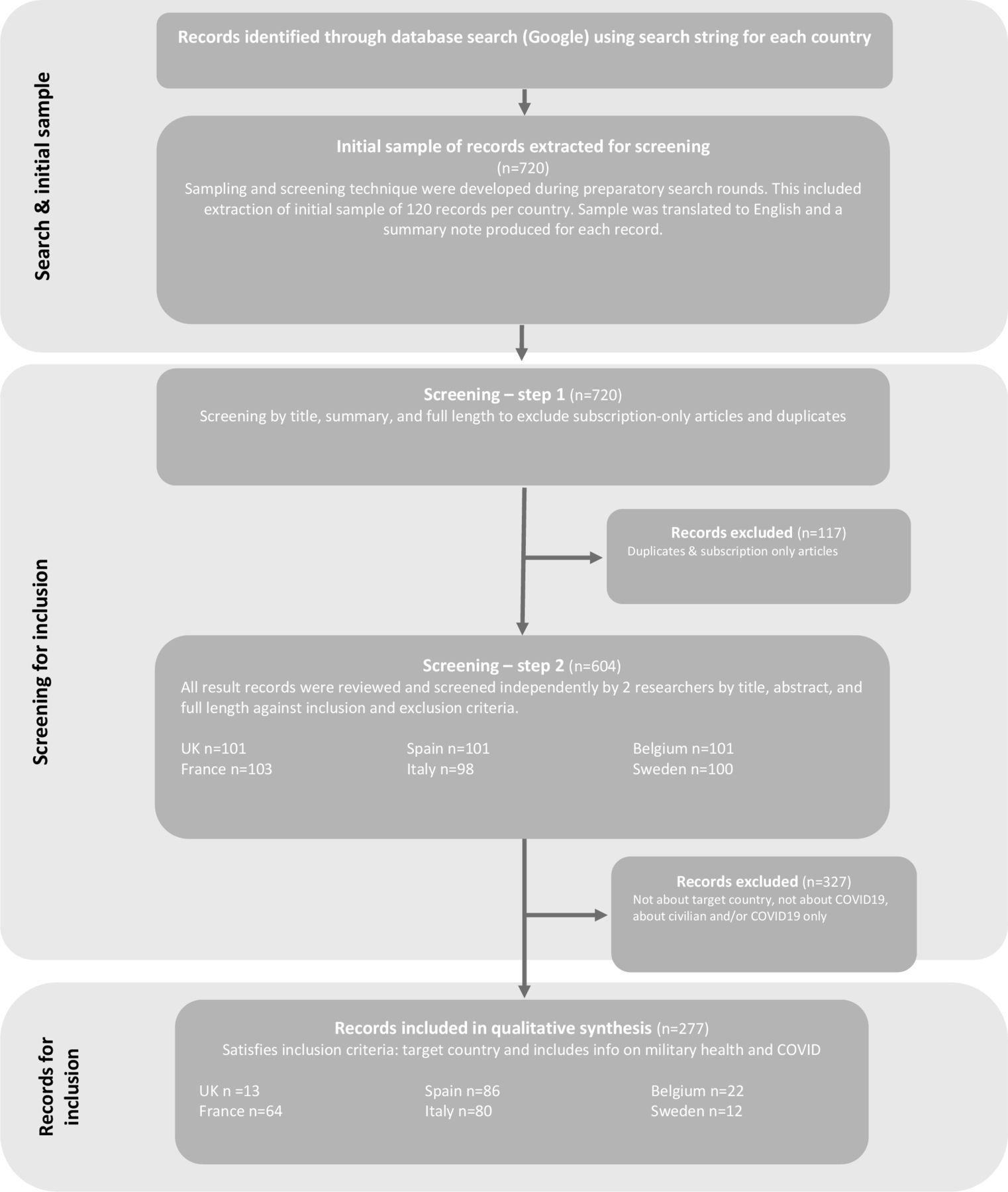
The sampled records were entered into two-step screening process. The first step involved screening by title and full length to remove any duplicates or subscription-only articles. The second step involved screening by title, summary and full article length. This was done to detect relevant records for qualitative synthesis based on our inclusion criteria. This produced a total of 277 articles across the six countries. Data extraction was conducted in line with the set inclusion criteria (see online supplemental material). The ‘search relevance’ was measured by dividing the number of included records over number of hits in initial screened sample (screening step 2). The inclusion criteria include records from open-source information, on military/security incorporation to national response, relating to current COVID-19 outbreak, and within target six countries. Records were excluded if they were in a format not instantly translatable by Google Translate (eg, PDFs), or not accessible, or were obvious duplicates. The full list of inclusion and exclusion criteria for our study is available in online supplemental material. Both screening steps were done independently by two researchers. Finally, the included records and their respective publication dates constituted a timeline of events of military involvement in each of the six countries’ national response to COVID-19. Figure 1 shows a brief illustration of the literature review process.

Literature review flow chart: data extraction and screening process.
Analysis: ‘Best fit’ approach to framework synthesis
We employed a framework synthesis approach in qualitative analysis of the result records. The approach built on a tentative conceptual model based on categories developed in the preparatory rounds of the search.29 Although the range of categories did not completely match the full range of results, it was considered a ‘best-fit’ model which used a starting point for augmentative and deductive analysis rather than relying on a complete grounded or inductive approach. Where any relevant data from included records did not translate into any existing categories, the authors applied a secondary thematic analysis grounded in data and based on methods from primary research, a similar approach to methods pursued by Carroll et al.30 31 In this way, the existing model could be developed as a tool for further analysis of the grey literature by adding or modifying existing categories.
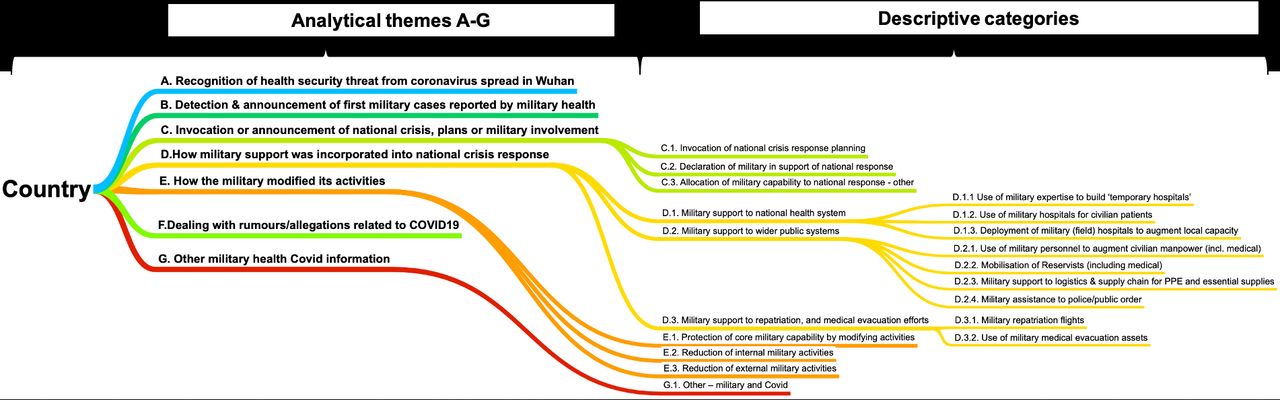
The main content of each record was coded to identify themes or constructs that lay in or across individual records. These codes were assigned to each record in one or more descriptive category(s). This was done depending on how military health information detected relates to our research question (ie, typologies of military health cooperation) (second-order interpretation). The resultant descriptive categories were organised to formulate overarching analytical themes (third-order interpretation). The nomenclature and dichotomy of the resulting descriptive categories and themes were fully reviewed, and further refinements were developed through iterative discussion during data appraisal. As such, a final conceptual model was produced and errors in indexing of data were checked by revising the categorisation process once more using the final conceptual model. The final set of descriptive categories and analytical themes is shown in Figure 2.
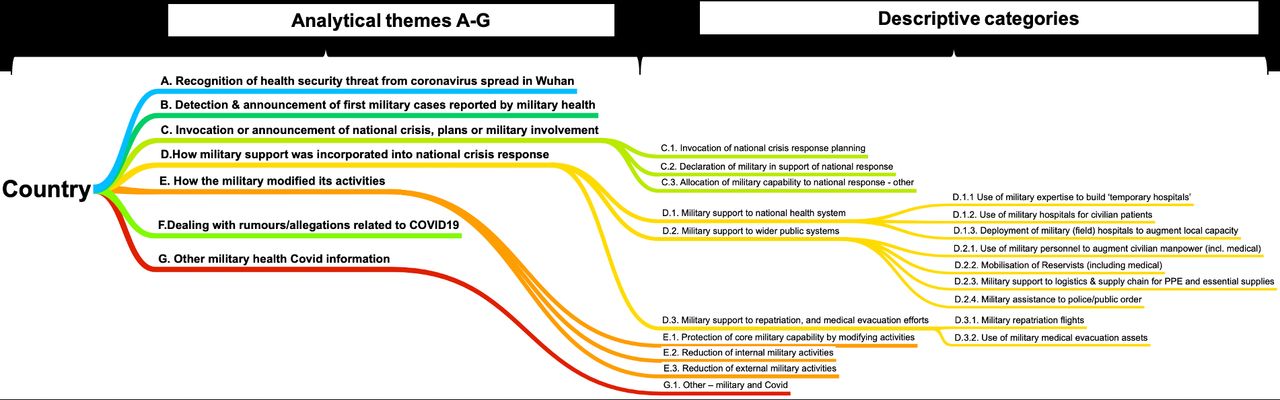
Conceptual model: descriptive categories and analytical themes. PPE, personal protective equipment.
Our qualitative analysis both enabled us to compare thematic findings for this review and to measure: frequency of elicitation of various categories and themes (which is the number of times a certain category or theme was triggered by coded records); the extent or range of findings (which is the number of distinct categories or themes triggered by the result records); and the order of emergence of these categories or themes with respect to time or country.
Results
Detection of military health incorporation in national COVID-19 responses
Search performance
A total of 277 records were determined to be relevant for our qualitative synthesis in this review. These records span across the six target countries. Information available on military health incorporation in national COVID-19 response was detected in all country searches, with an overall search relevance yield of 46%. However, information available per country varied greatly. Spain showed the highest search relevance with 85% of extracted records satisfying our inclusion criteria, while Sweden and the UK showed the lowest search relevance with 12% and 13%, respectively (see Table 1).
Overview of main themes and categories detected per country (numerical overview)
Overview of main themes and categories detected per country (categorical overview)
Qualitative synthesis of results
Our qualitative synthesis of the results was aimed at identifying the typology of information on military health incorporation in national COVID-19 response in target countries. There were a total of 19 distinct descriptive categories identified, with varied representation in terms of elicitation frequency and range. These categories extended across seven main analytical themes (A–G). They range from recognition of health security threat by military health systems to announcement of military involvement in the national COVID-19 response, invocation of national crisis planning, supporting with hospital facilities, personnel, logistics supply chain and public order. Figure 2 illustrates a conceptual model for qualitative synthesis. It denotes the nomenclature of the descriptive categories as induced from our ‘best fit’ framework analysis of the results and their overarching analytical themes (A–G). The list of descriptive category definitions is available in online supplemental material.
Results from Italy and Spain showed the highest descriptive category elicitation (Table 1). This was true both in terms of frequency, eliciting categories 128 and 119 times, respectively, and in terms of range both triggering 15 out of the total detected 19 categories, extending across six and seven different analytical themes, respectively. Meanwhile, Sweden showed the lowest number of descriptive category elicitation frequency, 13 times only, and triggered eight different categories extending across four analytical themes.
Source and type of result records
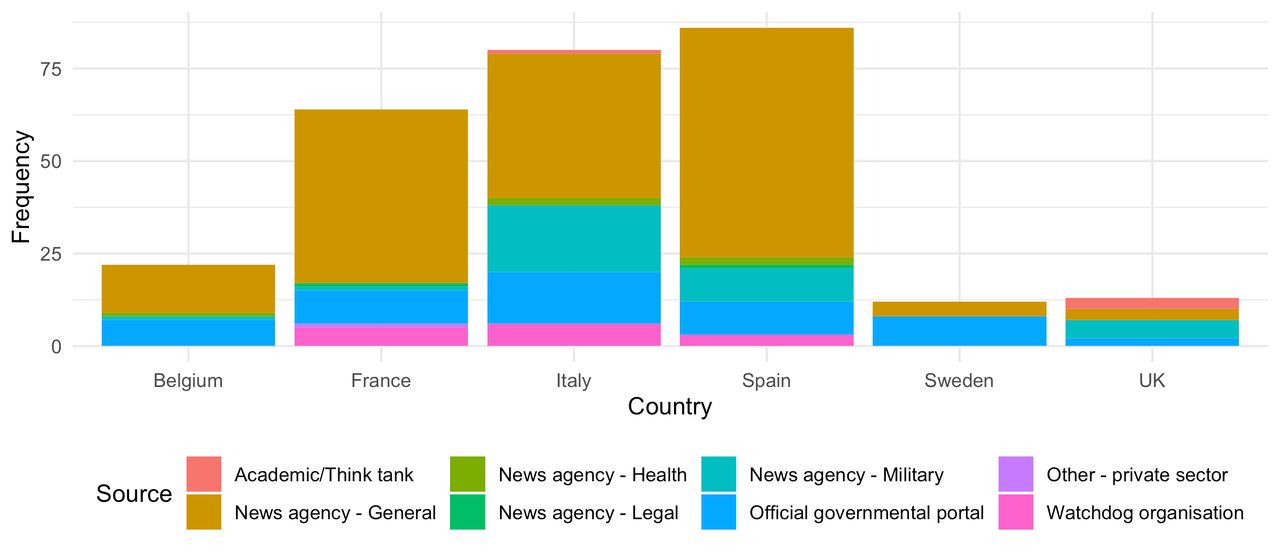
News agency articles collectively comprised 76% (n=209) of the total results. The majority were from general news agencies (61%) (n=168), while others were from military specialised news agencies (12%) (n=34) and otherwise specialised (legal or health) (3%) (n=7). Eighteen per cent (18%) of the result records originated from official governmental portals (n=49). These were mainly communications, announcements, guidance, institutional reports and other news information from official governmental institution web pages. Most common official web pages were from Ministry of Defence, Ministry of Health, Ministry of Interior, Ministry of Foreign Affairs and Local Councils, or their equivalent in each country. Finally, 5% of the records were sourced from watchdog organisations (n=14) and 1% from academic/think tank organisations (n=4).
Compared with all other countries, Italy returned the highest number of results from official governmental institutions (n=14), followed by France and Spain (n=9) (Figure 3). The UK showed the lowest number with only two records originating from governmental institutions (n=2). Meanwhile, the highest number of results from news agencies came from Spain (n=74), followed by Italy (n=59) and France (n=49). Sweden showed the lowest number, with only four records originating from news agencies (n=4). Other sources included ‘watchdog’ organisations which were most prominent in Italy (n=6), and academic or think tanks which were highest in the UK (n=4).
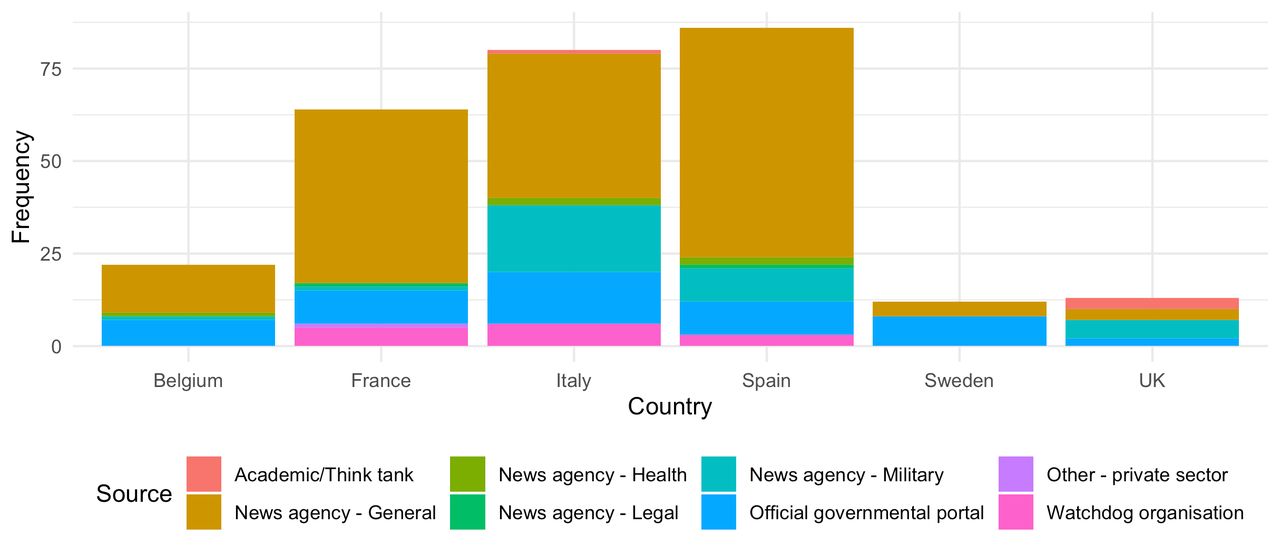
Source type—number of records per country.
Role of military health in national COVID-19 response
How the military supported health security provision
Frequency of descriptive category elicitation
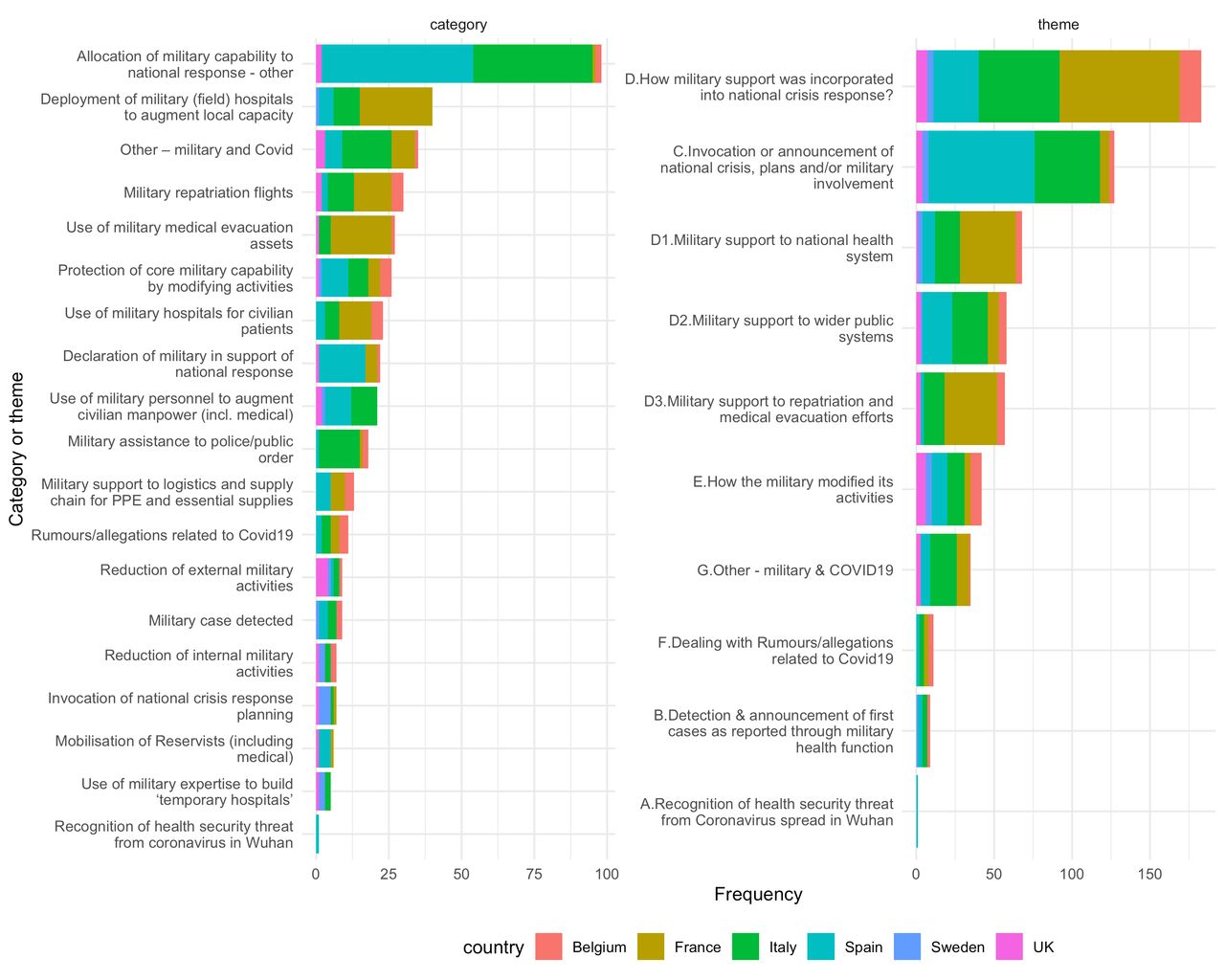
The most frequent category elicited by the search results was ‘Allocation of military capability to national response’ (n=98). This category denotes information relating to general support of military to more than one domain for national COVID-19 response and/or mentions a strategy or plan of support, including legislations or formal decisions. Results from all countries except Sweden elicited this category. Spain and Italy recorded the most frequent elicitations of this category (52 and 41 times, respectively).
‘Deployment of military (field) hospitals to augment local capacity’ returned the second most frequent elicitation (40 times). This category denotes information relating to deployment of temporary medical facilities by the military to support local capacity (ie, to add to required surge capacity). For example, on 17 March 2020 several French news media reported a new 30-bed field hospital being deployed by the French army in Alsace.32 Results from all countries except the UK and Belgium elicited this category. France returned the highest category elicitation (25 times), followed by Italy (9 times), Spain (5 times) and Sweden (1 time).
Other non-specific military information relating to stories or narratives that emerged because of COVID-19 returned the third most frequent elicitation (35 times). This includes, for example, opinion pieces about army readiness in case of being summoned to intervene, or personal stories of military personnel back dealing with COVID-19, or calls for new units or formations in military to deal with COVID-19. This category ‘Other—military and COVID-19’ was elicited in all countries except Sweden, with Italy at the top rank (17 times).
‘Military repatriation flights’ and ‘Use of military medical evacuation assets’ ranked fourth and fifth (30 and 27 times), respectively. The earlier denotes information relating to using military support to augment commercial repatriation of nationals from international destinations. The latter represents information on military support to transportation using ground ambulances, aeroplanes or trains nationally or internationally for purpose of redistribution or to meet the medical needs of patients. France came on top for these two categories (category elicited 13 and 21 times, respectively), with no mention of either from Sweden and no mention of medical evacuation from Spain. Figure 4 provides a full breakdown of category and theme frequency by country.

Frequency of theme and category elicitation per country. PPE, personal protective equipment.
Prominent themes of military health incorporation
Our descriptive analysis of the results identified seven main themes (A–G) of military health involvement during the COVID-19 outbreak in target countries (Table 2). Spain was the only country to report recognition of health security threat from COVID-19 spread in Wuhan. Meanwhile, none of the countries reported any role for military health services in COVID-19 testing.
Most categories triggered by the result records belonged to analytical theme ‘D—How military support was incorporated into national crisis response’ (183 times). It includes information on how the military provided support to national health system (D1)—for instance, deploying field hospitals or giving access to civilians to use military hospitals, supporting wider public systems (D2)—such as public order or supply chains, and supporting repatriation efforts and medical evacuation (D3). D1 and D3 were predominantly triggered by French results (36 and 34 times, respectively), while D2 was mostly triggered from Italian results (23 times).
Analytical theme ‘C—Invocation or announcement of national crisis, plans and/or military involvement’ came second with respect to frequency (127 times). This theme included information on declaration or statement of intent by various national governments to use military/armed forces as part of their national response, or reports of general details of how military interventions will be incorporated in these responses.
A breakdown of frequency of triggering analytical themes per country is provided in Figure 4 and overview of main themes detected per country is provided in Tables 1 and 2.
Time analysis: first to report
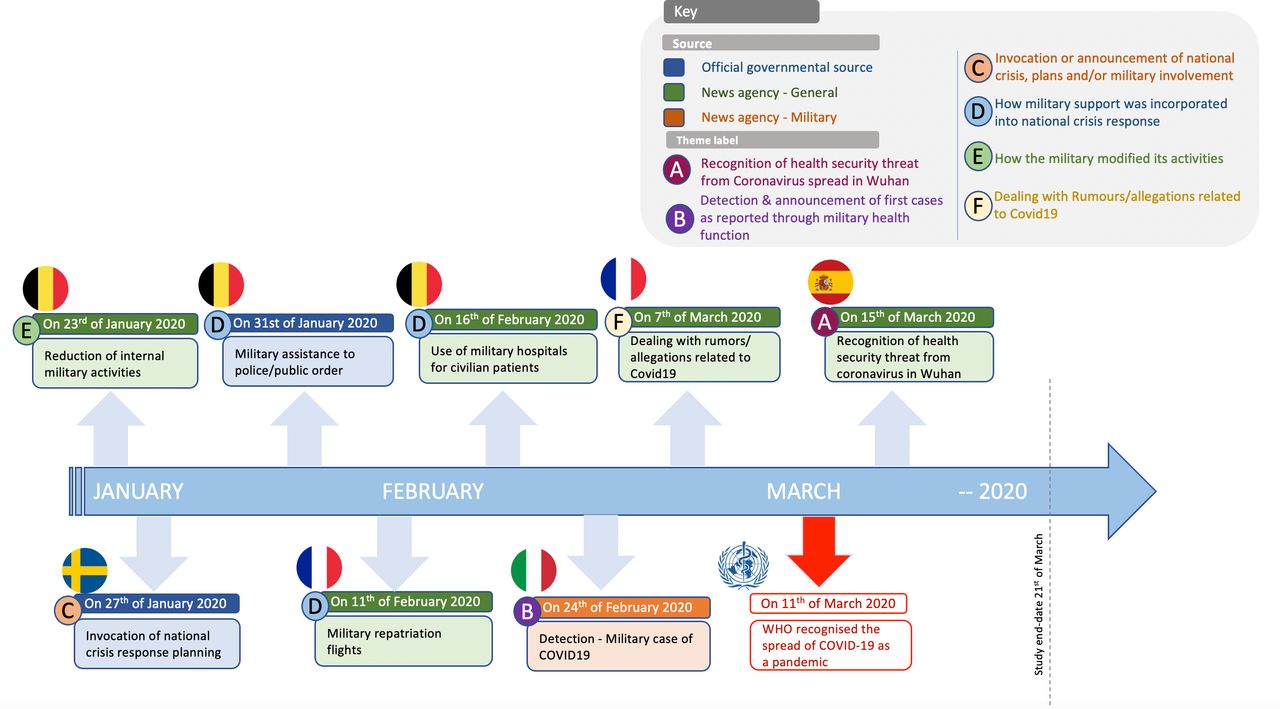
Our time analysis is based on the period from 20 January to 21 March 2020. The first relevant hit was detected in the search from Belgium on 23 January 2020. It is concerned with how the military modified its internal activities with a news report claiming that Belgium cancelled its participation in Defender Europe 2020 to stop the spread of the virus.33 The first public announcement of invocation of crisis response came 5 days later from the official defence ministry website in Sweden on 27 January 2020. This announcement described a military exercise done to practise leading and collaborating with civilian authorities in case of exposure to emergency situations.34 By 31 January 2020, the Belgian government was the first to report deploying soldiers to maintain public order and carry out surveillance missions.35
In early February, France was first to report military support to repatriation flights through news media agencies.36 Belgium followed suit on 16 February 2020, with news media reports of use of military hospitals by civilian patients.37 On the 24th of the same month, Italy was the first country to report military cases of COVID-19 in Cremona (Northern Italy).38 All other countries subsequently reported military cases except France and the UK. The first country to report results dealing with COVID-19 rumours was France as communicated by news media reports on 7 March 2020.39 Finally, recognition of health security threat from COVID-19 spread in Wuhan was barely reported by military health sources in all target countries. Spain was the only country to report results in this category as late as 15 March 2020, with a news report speculating whether declaration of a state of alarm will result in armed forces deployment in the country40 (Figure 5).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Timeline of coded result records.
Discussion
The results of our study suggest that the armed forces and military health systems have had an important role in supporting national COVID-19 measures. As suggested by our qualitative synthesis of the results, military support was detected across a wide range of descriptive categories of interventions. These categories comprise six main themes of military health support. This includes: recognition of health security threat from COVID-19 spread, detection and announcement of first military cases, invocation of national crisis plans (including announcing of military involvement), information on typologies of military support (how support was provided to specific interventions), dealing with rumours and modifying internal and external routine military activities to accommodate changes posed by the COVID-19 pandemic. However, while comparing the proportion of Google hits, this study does not provide a true comparative resource ‘denominator’ between countries. It is intended to evaluate this in further studies. Possible examples might be ‘per cent of total armed forces in support of COVID-19 response’, ‘per cent military personnel of overall national manpower response’ or ‘per cent of military medical personnel as part of national health workforce’.
The bulk of information detected relates to the question of typologies of military intervention (ie, theme ‘D—how military support was incorporated into national crisis response’). This was reflected by subthemes (D1–D3) showing that the popular types include: support to national health system such as building new hospitals or extending access for civilians to military hospitals; supporting public systems such as logistics and supply chains, mobilisation of reservists or deploying personnel to support policing and maintaining public order; and supporting repatriation and medical evacuation efforts. It is notable that Spain was the only country to show military health reports on the recognition of health security threat from coronavirus spread in Wuhan, although relatively late in date (March 2020) and that none of the selected countries reported any information on supporting COVID-19 testing campaigns. This is maybe explained by the early cut-off adopted by this study (until 21 March 2020) relative to how the crisis has unfolded subsequently.
The countries that reported the most information on the military contribution to the response were (in order) Italy, Spain and France, whereas Sweden, UK and Belgium reported the least. While these findings show what has been reported or debated in public grey literature sources, it does not provide a causal explanation for this difference. This might be due to structural factors, such as proportionally smaller armed forces, or that the armed forces were a smaller proportion of the national response. It might also be due to differences in government communication policies or media interest. Moreover, the majority of information on military health support during the pandemic was reported by news media reports, and to a lesser extent by official governmental sources. Compared with other countries, the Italian authorities were the most communicative about military health role in supporting government response. Meanwhile, watchdog organisations were the most active in Italy, and academic groups the most active in the UK. Further research is needed to assess the level and reasons for discrepancies between what has been reported, by whom and the role of military health support reported in these countries versus what has been actually implemented and missed in reporting.
Finally, different countries had different viewpoints with regard to the effectiveness of military intervention in controlling the spread of the virus. For example, in Sweden, the military exercise done to practise leading and collaborating with civilian authorities in case of exposure to emergency situations was announced as a means to plan for crisis response against COVID-19.34 Likewise, in France, participation in Operation Defender Europe 2020 was deemed suitable to simulate similar possible emergency situations posed by COVID-19.41 This was also the case in the UK where special military operations were designated to contribute to COVID-19 national response (Operations Broadshare and Rescript).42 In contrast, Italy cancelled their participation in Defender Europe 2020 to help stop the spread of COVID-19,43 and no mention of such exercises was reported in Spain or Belgium.
Strengths and limitations
Open-source grey literature review may not exhaustively capture all of the contribution of a country’s armed forces to their response to the COVID crisis. Publicly available information on an individual country’s military health system may be restricted for security reasons or to manage public perceptions. This is evident in both direct surveying of information from countries and in available academic literature. This is further compounded by the fact that academic databases are inherently characterised by a time lag in information acquisition, with a great deal of potential data loss in the process.44 However, recent methodological literature suggests that open-source grey literature is a good alternative source for obtaining military health information. This is due to its ability to give access to an array of data sources not readily available in traditional academic sources, including, for example, news media, governmental or institutional reports.44 45 In addition, grey literature helps in reducing publication bias and facilitates a more balanced view of available evidence.46 47
Conclusion
This study shows the potential significance of military systems in supporting an expansive response during the COVID-19 pandemic. Militaries and their parallel health systems can bring essential capabilities towards boosting capacity of the civilian health system in times of emergency. Reported information on the role of military in national COVID-19 responses varied greatly across the six countries, with potential low reporting in some countries requiring further research for validation. In some cases, there was extensive collaboration between military and civilian health systems, and in other cases, it was a parallel arrangement, whereby the military worked largely independent of the civilian system; for example, military field hospitals were manned by military personnel with minimal to no civilian engagement.
This paper has served three main important purposes. First, it sets out a methodological approach to capture otherwise restricted military information; second, it allows for a reproducible way to gather and interpret information on modes of military support to the COVID-19 response between countries; and lastly, it gives a comparative view on how countries have drawn on military health support and what the common interventions supported by the military in each country were. We believe there is a need for further research in order to fully understand the contribution of military health systems to a country’s health economy and how they can best complement civilian health facilities as part of civil–military cooperation both in emergency and non-emergency situations. This has the potential to inform the lessons learnt process in evaluating choices for civil–military cooperation as part of national resilience to mitigate future health crises.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @Gadosk, @MartinBricknell
Contributors MB, MG, AG, JK, EQ and ZH were involved in the planning, conduct and reporting of the work. MB provided oversight to set research objectives and supported choice of appropriate method. Research protocol was developed and reviewed by MB, MG, AG, JK, EQ and ZH. Data search was conducted independently by EQ and JK and reviewed by MG with error check and comments from MB, AG and ZH. Analysis was conducted by MG with review and comments from MB, AG, JK, EQ and ZH. AG and ZH reviewed the preparatory search rounds and provided comments on approach for main search (including target countries selection). MG wrote the first and final drafts of the manuscript. MB, AG, JK, EQ and ZH reviewed and commented on the initial and final drafts of the manuscript.
Funding AG acknowledges funding from the Research Councils UK through the Research for Health in Conflict in the Middle East and North Africa (ES/P010962/1). MG and JK are members of the MRC Centre for Global Infectious Disease Analysis (MRC GIDA), jointly funded by the UK Medical Research Council (MRC) and the UK Department for International Development (DFID) under the MRC/DFID Concord at agreement and is also part of the EDCTP2 programme supported by the European Union. Grant reference and affiliation: MR/R015600/1; MRC Centre for Global Infectious Disease Analysis, School of Public Health, Imperial College London. MB is partially funded through the UK Research and Innovation GCRF Research for Health in Conflict developing capability, partnerships and research in the Middle and Near East programme (R4HC-MENA) ES/P010962/1.
Competing interests MB and AG report grants from UK Research and Innovation GCRF Research for Health in Conflict, outside the submitted work. MB was previously the Surgeon General of the UK Defence Medical Services until 1 April 2019.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.