Article Text

Abstract
Undifferentiated febrile illnesses present diagnostic and treatment challenges in the Firm Base, let alone in the deployed austere environment. We report a series of 14 cases from Operation TRENTON in South Sudan in 2017 that coincided with the rainy season, increased insect numbers and a Relief in Place. The majority of patients had headaches, myalgia, arthralgia and back pain, as well as leucopenia and thrombocytopenia. No diagnoses could be made in theatre, despite a sophisticated deployed laboratory being available, and further testing in the UK, including next-generation sequencing, was unable to establish an aetiology. Such illnesses are very likely to present in tropical environments, where increasing numbers of military personnel are being deployed, and clinicians must be aware of the non-specific presentation and treatment, as well as the availability of Military Infection Reachback services to assist in the management of these cases.
- fever of unknown origin
- disease and non-battle injuries
- military personnel
- South Sudan
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
Undifferentiated febrile illnesses present a continuing diagnostic and therapeutic challenge for UK military medical personnel.
Despite an enhanced laboratory, no in-theatre diagnoses were made in this case series of 14 patients, the majority with non-specific symptoms and full blood count abnormalities.
Returning acute samples to the Firm Base presents a logistical challenge, and results from acute and convalescent samples (even from Role 4 facilities) may not be diagnostic.
Next-generation sequencing technology is rapidly miniaturising and may at some point be deployable, potentially providing vital information in these cases.
Introduction
Undifferentiated febrile illness (UFI) describes an acute illness with documented fever, usually of less than 2 weeks’ duration, with no obvious clinical, radiological or microbiological focus. The definition of this term, unlike that of pyrexia/fever of unknown origin, has not been conclusively established, but tends to focus more on infectious causes and is particularly used in tropical settings.1
Operation TRENTON is the UK contribution to the United Nations Mission in South Sudan (UNMISS). UK Defence Medical Services personnel provided, in addition to ongoing integrated Level 1 Medical Treatment Facilities (MTFs), an enhanced Level 2 MTF in Bentiu from 2017 to 2018, with enhanced laboratory and radiology capability. We previously outlined a snapshot of clinical activity at this hospital2—this paper aims to describe a case series of UFI seen during this time.
During the period of June–August 2017, a Relief in Place of troops took place on Op TRENTON. Coinciding with the rainy season, living conditions were difficult, with significantly increased standing water, insect numbers and increased numbers of consultations by UK and UN personnel at MTFs. Logistical support to the deployed hospital, including supply of laboratory consumables, was a major challenge.
Case vignette
A British soldier presented to the Level 2 MTF in Bentiu, complaining of feeling hot and sweaty, as well as a headache and all-over body aches. There were no focal symptoms. He was normally very fit and well, taking malarone prophylaxis with no missed doses and no allergies.
On examination, he looked unwell, with a temperature of 39.5°C, pulse 100 bpm and BP 110/70 mm Hg, and he appeared dehydrated. Cardiac, chest and abdominal examinations were unremarkable; there were no neurological signs and no rash. His white cell count (WCC) was 3.0×109/L (neutrophils 1.6×109/L, lymphocytes 0.6×109/L) and platelets 175×109/L. C reactive protein (CRP) was 24 mg/L; creatinine was 130 μmol/L. Chest radiograph was unremarkable. He was suspected to have an undifferentiated febrile illness, and so was admitted and commenced on doxycycline.
Over the course of the next 24–48 hours, his condition deteriorated, becoming more hypotensive, maintaining a temperature >39.5°C and WCC dropping to 2.6×109/L (neutrophils 1.3×109/L, lymphocytes 0.4×109/L). To cover sepsis, he was treated with ceftriaxone before switching to meropenem when his BP continued to sag and he was moved to be observed on the intensive care unit.
Over the next 5 days, his condition improved, with normalisation of his vital signs and blood results. Blood cultures were negative. However, he developed severe nausea preventing eating, initially suspected to be giardiasis (evidenced from the stool) treated with metronidazole, but which only resolved with stopping doxycycline. He was discharged on day 8 to finish a course of co-amoxiclav.
Case series
Over a 6-week period, 14 UK military personnel were admitted to the L2 MTF with an acute fever. After clinical, microbiological and radiological examination (when available), no definitive diagnosis could be made, and so these cases were labelled as UFI. Radiological investigation included plain chest radiograph and ultrasound when available. Laboratory testing included full blood counts (ABX Micros ES60; Horiba), CRP, renal and liver function (NX500; Fujifilm), lactate (i-STAT; Abbott), blood cultures (BacT/ALERT; Biomerieux) and malaria rapid diagnostic tests (BinaxNOW Malaria; Abbott), as well as syndromic testing using the FilmArray platform (Biomerieux), if symptoms indicated and the appropriate clinical sample was available. Serum samples were saved at −20°C in case recovery to the UK became possible.
On return from deployment, patients were invited for review at the Role 4 Infectious Diseases and Tropical Medicine Clinic in Birmingham, and convalescent serum was taken for testing at the Rare and Imported Pathogens Laboratory, PHE Porton.
Clinical and laboratory data were collected in real time by the deployed clinicians during the Relief in Place of TRENTON 2 by TRENTON 3, in a non-protocolised manner.
All fourteen cases were male, with seven aged 20–29, five aged 30–39, one was 40–49 and one 50–59. All were admitted for observation (median 3 days, range 1–8 days).
Table 1 details the presence of symptoms in this cohort, as well as the occurrence of abnormalities in laboratory or radiological investigations. All cases (by definition) had a temperature >38°C, with a mean peak fever of 38.9°C (range 38°C–39.9°C). Nearly all cases had headaches, with the majority having myalgia, arthralgia and back pain.
Symptomatology and investigations in patients admitted with UFI
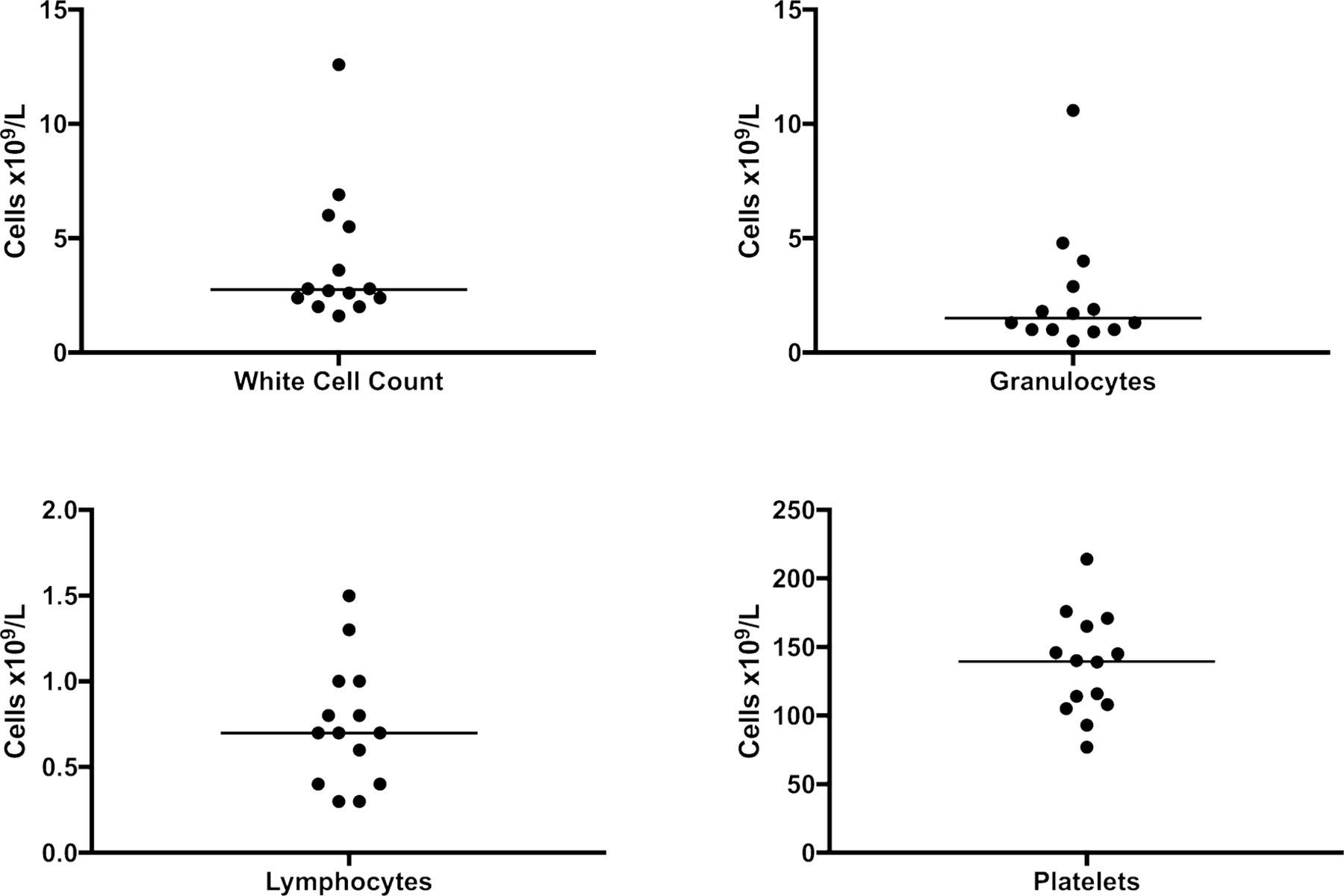
All cases were negative for malaria, and the majority had abnormalities with WCC components being below the lower limit of normal for the analyser used. Figure 1 details this further, revealing a median result for the WCC of 2.75×109/L, granulocytes 1.5×109/L, lymphocytes 0.7×109/L and platelets 139×109/L. CRP was mildly elevated in seven patients (median 12 mg/L, IQR 3–24 mg/L). Of the three lactate samples taken, all were within the normal range. No radiological abnormalities were observed.

{kind=link}
Plot of white cell count and component results in 14 patients with undifferentiated febrile illness. Median (IQR) of the white cell count was 2.75×109/L (2.3–5.6), granulocytes 1.5×109/L (1.0–3.2), lymphocytes 0.7×109/L (0.4–1.0) and platelets 139×109/L (107–167).
The FilmArray respiratory panel was used in three cases with upper respiratory tract (URT) symptoms—one sample was positive for rhinovirus, but this was felt clinically not to be responsible for the severity of illness observed.
Doxycycline was administered in 12 of 14 cases, particularly to cover the possibility of rickettsial infections, Q Fever and leptospirosis. The sickest case (described), who was admitted for 8 days, was given a combination of five antibiotics, as well as precautionary observation in the intensive care unit. As his clinical picture evolved, towards the end of his stay he appeared to develop a moderate adverse reaction to doxycycline.
Of the 14 cases, 13 were reviewed in Role 4 after their return. Samples taken at this time were tested for convalescent serology, with the results shown in table 2. All samples were positive for yellow fever virus IgG because all UK personnel were vaccinated against yellow fever prior to entry to South Sudan. Of the five positive results, the positive dengue and tick-borne encephalitis virus IgG were thought to represent flavivirus cross-reaction with the yellow fever vaccine, the positive (borderline) dengue IgM was considered non-specific and the Toscana virus IgG representative of past exposure.
Results of testing on acute and convalescent sera
Acute serum from 14 patients reached the UK 9 months after the end of the deployment (due to aforementioned logistical difficulties) and were tested by PCR for Ebola virus and Crimean-Congo haemorrhagic fever virus; all tests were negative. Four of these samples were selected for further PCR testing as detailed in Table 2 (based on convalescent results), but there were no positives.
Twelve acute samples (with sufficient remaining sample volume) were selected for next-generation sequencing (NGS) to establish aetiology. No genetic material of bacterial, viral or parasitic origin was detected.
Discussion
Infectious diseases have long been a significant cause of morbidity and mortality to the British military.3 Previous data have demonstrated that, second to infective gastroenteritis, UFI presented a significant caseload for deployed MTFs in both Iraq4 and Afghanistan,5 as well as at Role 4.6 The recent response to the Ebola crisis in West Africa demonstrated that UFI continues to be a significant reason for admission.7 Op TRENTON demonstrated a continuation of this trend, with cases of gastroenteritis being the greatest workload for the medical team (37%) followed by UFI (12%). Non-malarial UFI represented the largest proportion of emergency department consultations (17%).2
Non-malarial undifferentiated febrile illness is increasingly recognised as a significant issue in sub-Saharan Africa. A recent review found that studies investigating multiple causes of fever were few in number and generally reported a large proportion of patients without an aetiological diagnosis.8 This was suggested to be due to a combination of insensitive tests, the difficulty in ascribing causality when multiple tests results were positive and the potential for undiscovered novel pathogens to be responsible for illness. A further review highlights the already large number of potential pathogenic arboviruses in Africa, not all of which are routinely or easily detectable.9
Our series demonstrates that ascribing an aetiological diagnosis to cases of UFI in an austere environment may not currently be possible. The Centre of Defence Pathology is well versed in providing advanced laboratory diagnostic solutions as far forward as possible,10 but despite this expertise we were unable to ascribe causality. With respect to the FilmArray, this was mainly due to the lack of appropriate sample to test (eg, diarrhoea, positive blood cultures etc) which is not surprising in cases of UFI. Where a potential focus was suspected (eg, URT symptoms) results from the FilmArray were not conclusive for diagnosis. This is in contrast to testing diarrhoea samples, for example, where FilmArray provided real-time results which affected clinical management.11 It should therefore be noted by providers that qualitative PCR (especially without appropriate interpretation) is not a solution to every testing conundrum.
Previous investigations on Op HERRICK (Helmand, Afghanistan) were able to find causative pathogens in febrile patients12 and identify seroconversion in well volunteers.13 Research in Mongolian troops serving in South Sudan showed seroconversion to Rickettsia, West Nile Fever, Q Fever and Leptospira, although it is unknown how many of these volunteers had symptoms.14 However, the Op HERRICK studies relied either on a frequent and reliable airbridge to return samples to the UK, or on sampling in the UK pre-deployment and post-deployment. In this theatre, returning samples to the UK was a particularly difficult logistical challenge. Although sample return via a reverse cold-chain was eventually agreed with the host nation, it is possible that sample degradation may have affected the results, although it is unusual that NGS was unable to detect any organism. Also, as the viraemia is short in many viral fevers, samples taken early in the illness may not yield a result before the immune response reduces the circulating viral load.
The majority of our cases received doxycycline—those who did not were felt by Infectious Diseases physicians to be unlikely to have antibiotic-sensitive disease. For isolated practitioners without infectious disease expertise, advice on difficult diagnostic and treatment decisions like these is available through Military Infection Reachback services. This is also relevant as one of our cases appeared to develop an adverse reaction to doxycycline which was challenging to manage. Patients with UFIs should be followed up by the Military Infection Service, particularly in the context of screening for diseases with long-term sequelae, such as Q Fever.
There has been rapid development of portable sequencing technology such as the MinION (Oxford Nanopore), which can detect viral genomes directly from clinical samples and has been tested in the field,15 as well as other near patient PCR-based molecular diagnostics. It may well be possible that future laboratory deployments will be equipped to be able to ascertain the aetiology of UFIs that present to MTFs. While existing constraints such as the enormous volume of data produced and the need for specialist bioinformatics support to analyse said data currently preclude any deployment of NGS, advances in miniaturisation may overcome this leading to information that could guide the administration or withholding of antibiotics in real time, as well as providing valuable epidemiological data from remote parts of the world.
Ethics statements
Patient consent for publication
Ethics approval
This Service Evaluation was approved by the Healthcare Governance Committee, Op TRENTON, and all data collected were anonymised and stored securely according to Caldicott principles.
Acknowledgments
We are grateful to personnel of the Centre of Defence Pathology for their expert advice, as well as the Genomics teams at PHE Porton and PHE Colindale. We are also grateful to the patients and staff of the UK Level 2 Medical Treatment Facility, Bentiu, South Sudan, during the period of this study.
References
Footnotes
Contributors JSB, JL, NEH and MSB looked after the patients in South Sudan. DSB and MSB reviewed patients at Role 4. EJH provided reachback microbiology and logistical support. JCO and AJS provided reference laboratory testing and interpretation. JSB drafted the manuscript, which was reviewed and approved by all authors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer The views expressed in this article are those of the authors and do not reflect the official policy of the Defence Medical Services, Ministry of Defence or British Government.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.