Article Text

Abstract
Purpose The extent and types of ophthalmic disease and non-battle injury (DNBI) seen by expeditionary ophthalmologists at deployed military medical treatment facilities have not previously been reported. We aim to characterise the extent and type of ophthalmic pathology including DNBI at a US military medical treatment facility in Afghanistan.
Methods We conducted a retrospective non-interventional cohort study of all patients seen by ophthalmologists at Craig Joint Theater Hospital at Bagram Airfield (BAF), Afghanistan, between 1 October 2018 and 31 August 2019.
Results There were 281 patients seen in 540 separate encounters, of which 146 patients seen were active duty military stationed at BAF with DNBI, of a population at risk of 6000 personnel. Diagnoses managed included open and closed globe injury, bacterial and herpetic keratitis and retinal detachment, with the most common being dry eye, corneal abrasion/foreign body, blepharitis, chalazion and uveitis. Thirteen patients (5%) required aeromedical evacuation out of theatre and 39 patients were aeromedically transferred within theatre for assessment. Expert consensus estimated that 89 patients (36%) would be likely to require aeromedical evacuation out of theatre without ophthalmic input.
Conclusions The rate of ophthalmic DNBI among deployed US, UK and coalition forces at BAF was 2.65% per year, of whom 97% were returned to duty (95% of all patients). We estimate that evacuation and loss to unit would increase from 5% to 36% without an ophthalmologist present. The low number of within-theatre aeromedical transfers suggests that the local presence of an ophthalmologist at a patient’s deployed medical treatment facility affects access to deployed ophthalmic care.
- ophthalmology
- epidemiology
- clinical governance
Data availability statement
No data are available. The data are clinical data and it would not be appropriate to share it, nor do we have permission to do so.
Statistics from Altmetric.com
Key messages
In a deployed Role 3 medical treatment facility, ophthalmology comprised 4.5% of the total outpatient workload including primary care and emergency medicine.
The rate of ophthalmic disease and non-battle injury (DNBI) among deployed US, UK and coalition forces was 2.65% per year.
Three per cent of ophthalmic DNBI required evacuation out of theatre, which we estimate would increase to at least 36% without an ophthalmologist present.
Introduction
Military ocular trauma is well characterised, with many papers from around the world reporting the types, management and outcomes of military battle injury, including the recent conflicts in Iraq and Afghanistan.1–7 Historically, and anecdotally, disease and non-battle injury (DNBI) is the most frequent cause of morbidity in deployed forces.8 9 Non-traumatic ophthalmic disease is the most common presentation to civilian ophthalmologists, and when ocular trauma does present it is often from injuries sustained during sports.10 Although the expeditionary ophthalmologist’s primary role during deployment is usually considered to be the surgical management of battle injury, significant numbers of DNBI cases are encountered in a deployed eye clinic. The expeditionary ophthalmologist must have a wide range of knowledge, skills and abilities to diagnose and manage DNBI, including military-unique and tropical conditions. However, the full extent and breakdown of ophthalmic DNBI at a Role 3 military treatment facility has not previously been reported. Heier et al 11 reported ophthalmic complaints at a deployed emergency department (ED) in support of Operations Desert Shield and Desert Storm (not including primary care and outpatient visits).11
US ophthalmologists have been deployed at the Role 3 military treatment facility Craig Joint Theater Hospital (CJTH) at Bagram Airfield (BAF), Afghanistan, in support of US, UK and North Atlantic Treaty Organization (NATO) operations since 2002–2003, providing care at that location for local forces and patients transferred from other areas in theatre. UK ophthalmologists first deployed to CJTH in September 2018. We describe the recent extent, diagnosis and management of ophthalmic DNBI presenting to CJTH from October 2018 to August 2019.
Methods
We conducted a retrospective chart review, examining all electronic medical records from 1 October 2018 to 31 August 2019 made by the ophthalmologists stationed at CJTH during that period and additionally examining the diagnosis codes for all patients seen in the ED in the same period to identify ophthalmic diagnoses. There was a UK ophthalmologist stationed at CJTH from October 2018 to August 2019. There was also a US ophthalmologist stationed at CJTH from April 2019 to August 2019. Data extraction was performed by two authors (MTK and RJB) and the data were cleaned and rechecked by RJB using the data collection tool in online supplementary figure 1.
Supplemental material
Cause of presentation was divided into: battle-related injury, defined as any injury caused by or related to enemy action; non-battle injury, defined as any injury not related to enemy action; disease, defined as as any other, non-traumatic, aetiology. Cause of presentation was taken from the determination made by the reviewing clinician in the electronic medical record.
To identify previous reports of ophthalmic DNBI, OVID Medline was searched for: [Ophthalmology/ OR Ophthalmology.mp] AND [Military Personnel/ OR Military.mp] AND [Disease/ OR Disease.mp OR Diseases.mp], 27 results of which none were relevant English language papers after 1960; Google Scholar was searched for ‘ophthalmology disease and non-battle injury’, 708 results of which only Heier et al detail ophthalmic DNBI at a deployed facility.11
Descriptive statistical analysis was performed in SPSS (V.21, IBM). Categorical analyses were performed using χ2 test for 2×2 and 2×4 tables, with diagnostic categories collapsed to: anterior segment pathology/closed globe injury; minor conjunctival/ocular surface pathology/chalazion/corneal abrasion/foreign body/no pathology seen/occupational encounters; neuro-ophthalmic/orbital pathology; vitreoretinal pathology.
Results
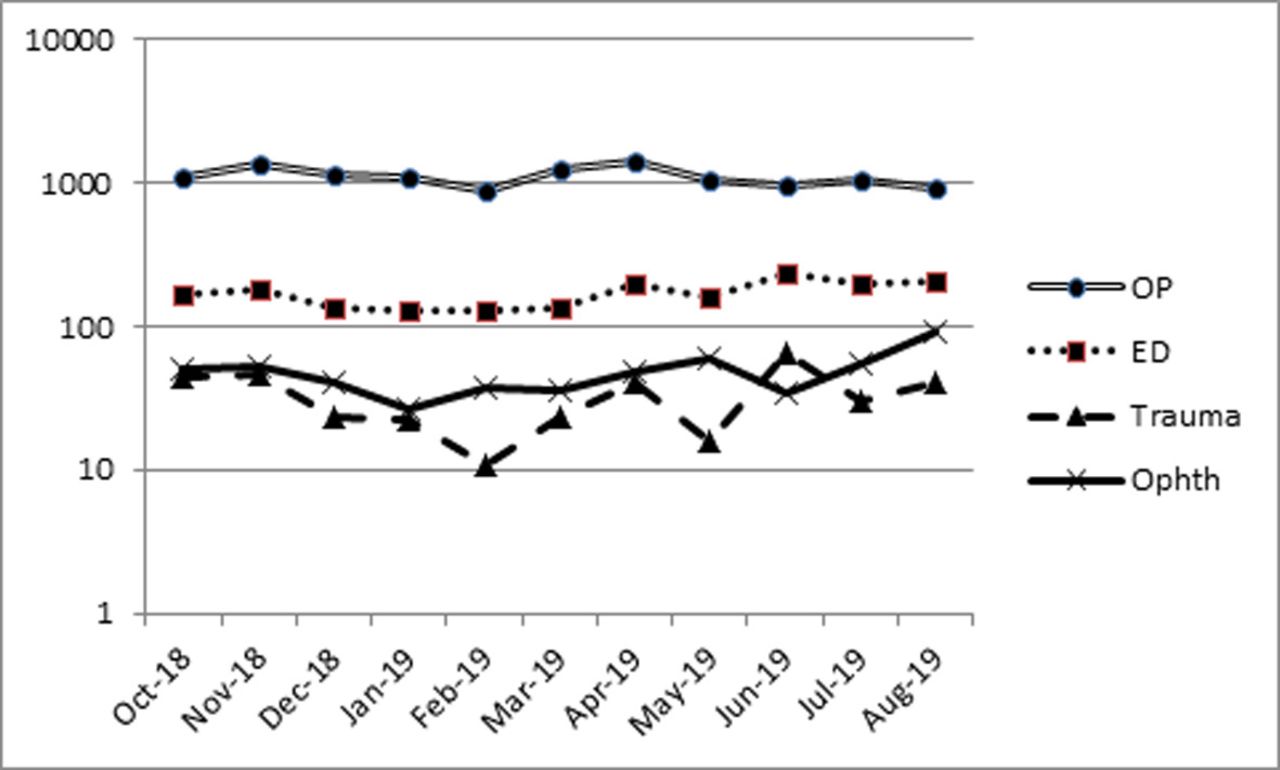
In the period from 1 October 2018 to 31 August 2019, there were 12 000 outpatient encounters at CJTH including primary care, physical therapy, psychology and surgical specialties. There were 1868 ED patient encounters, of which 362 were trauma encounters (Figure 1). Over the same period, there were 540 separate ophthalmology encounters with 281 patients, representing 4.5% of the total hospital outpatient and ED workload (Figure 1).
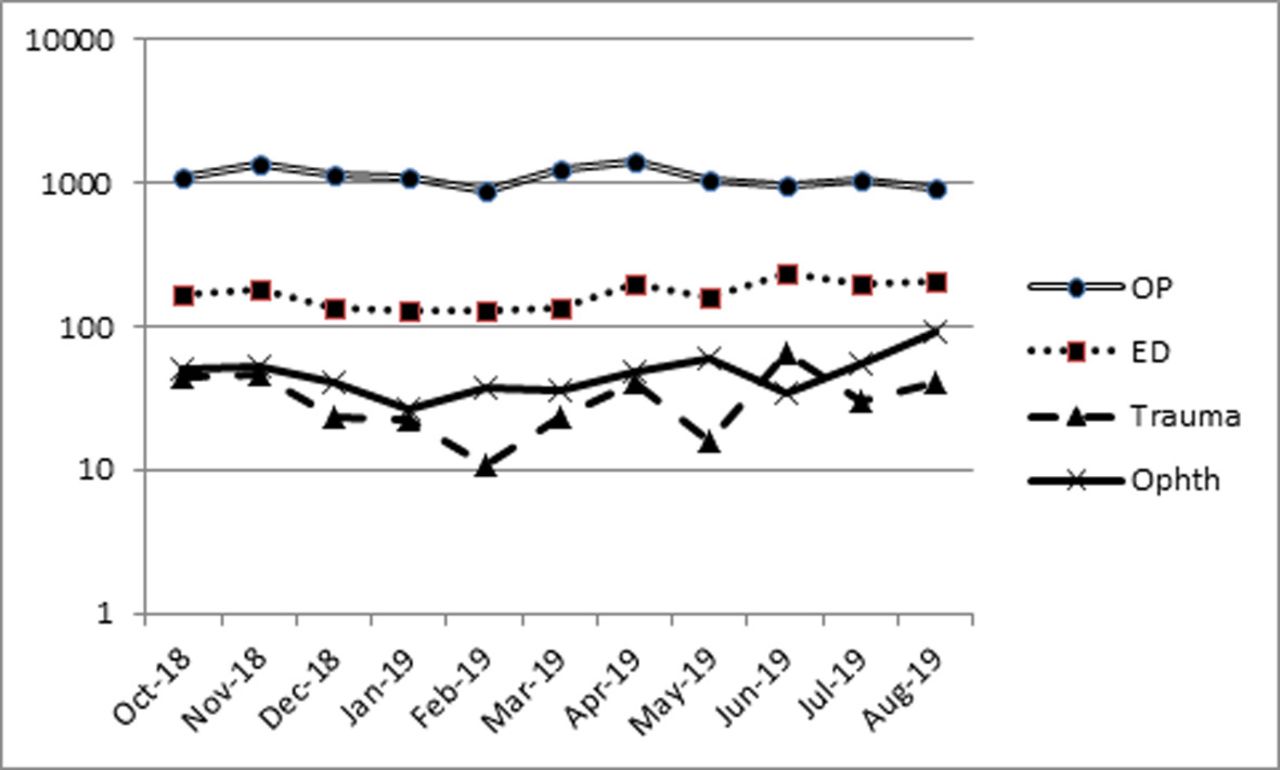
Patient encounters by month of presentation broken down into outpatient encounters (OP; including ophthalmology), emergency department (ED) encounters (including trauma), trauma cases presenting through ED (Trauma) and ophthalmology encounters (Ophth).
Patient demographics are summarised in Table 1. The presenting complaints are summarised in Table 2. A summary of the principle diagnosis for each patient is listed in Table 3.
Patient service branch, gender and age
Frequency of principle presenting complaint for each patient
Frequency of principle diagnoses for each patient (n=281)
Rate of DNBI and evacuation
Of 247 active duty or contractors seen in consultation, 208 were stationed at BAF and 39 were transferred by air within the theatre of operations. Of these, 175 were active duty military personnel seen with DNBI, of whom 29 (17%) were transferred (by air) within the theatre of operations for consultation. Therefore, of the 6000 military personnel stationed at BAF, 146 presented with DNBI, giving a DNBI rate among the local military personnel of 2.65% per year.
Thirteen patients were evacuated out of theatre (eight military, five of whom were stationed at BAF), all for ophthalmic disease (Tables 2 and 3), meaning that 95% of all personnel (234/247) and 96% of military service members (202/210) and 97% of military service members stationed at BAF (170/175) were returned to duty.
Origin of non-local patients within the theatre of operations
Compared with the total distribution of personnel in the theatre of operations, in which approximately 70% of all personnel were present at a different location to CJTH, the proportion transferred for review was significantly lower (χ2; p<0.001). Of all 247 active duty or contractors, there was evidence that the case mix transferred had fewer cases in the category ‘minor conjunctival/ocular surface pathology/chalazion/corneal abrasion/foreign body/no pathology seen/occupational encounters’ at 15/39 (38%) vs 111/208 (53%) and more cases in the neuro-ophthalmic/orbital pathology category at 10/39 (26%) vs 23/208 (11%; χ2 for a 2×4 table 7.95; p=0.047; Table 4).
Proportion of diagnoses in US and coalition military and contractor patients stationed at Bagram Airfield (BAF) and transferred for evaluation from elsewhere
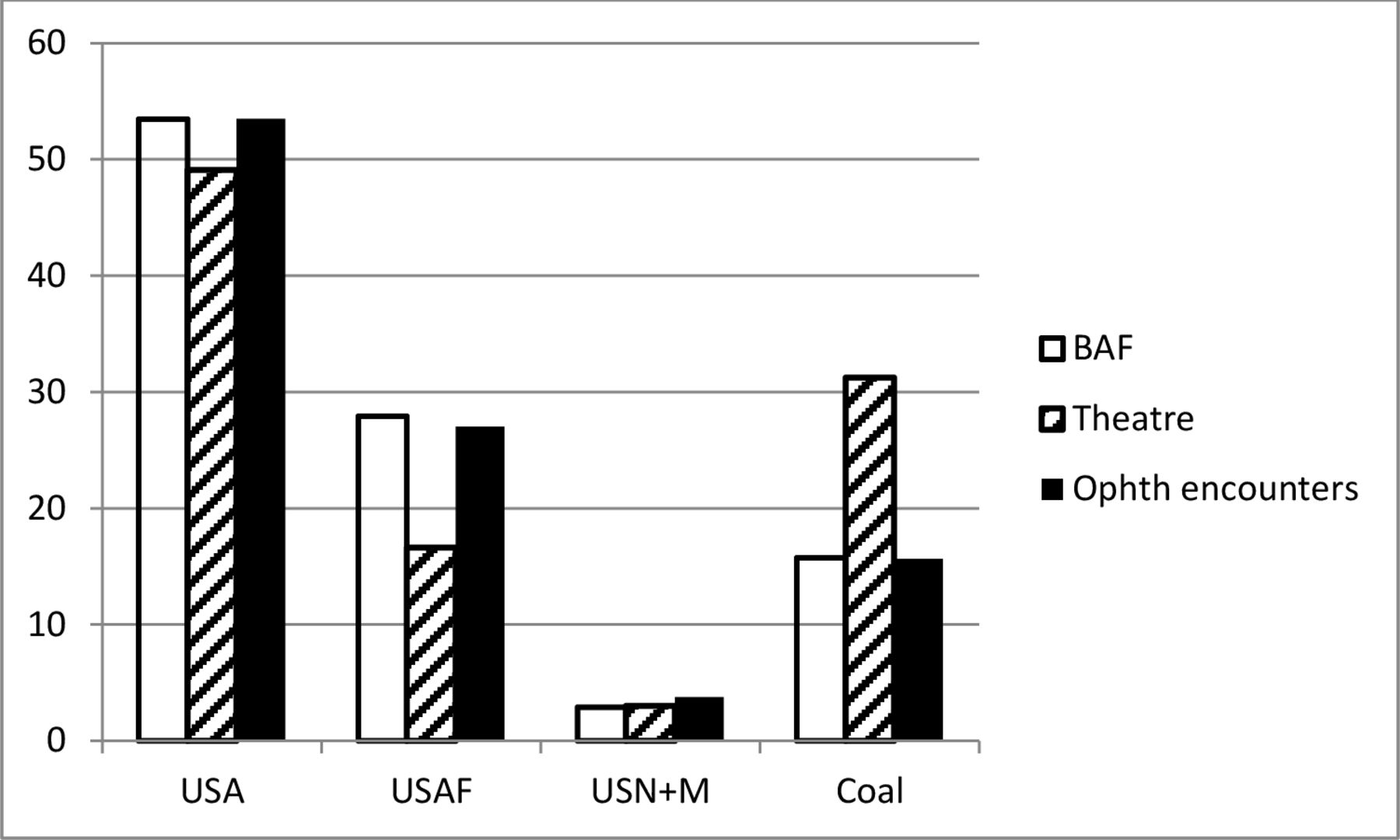
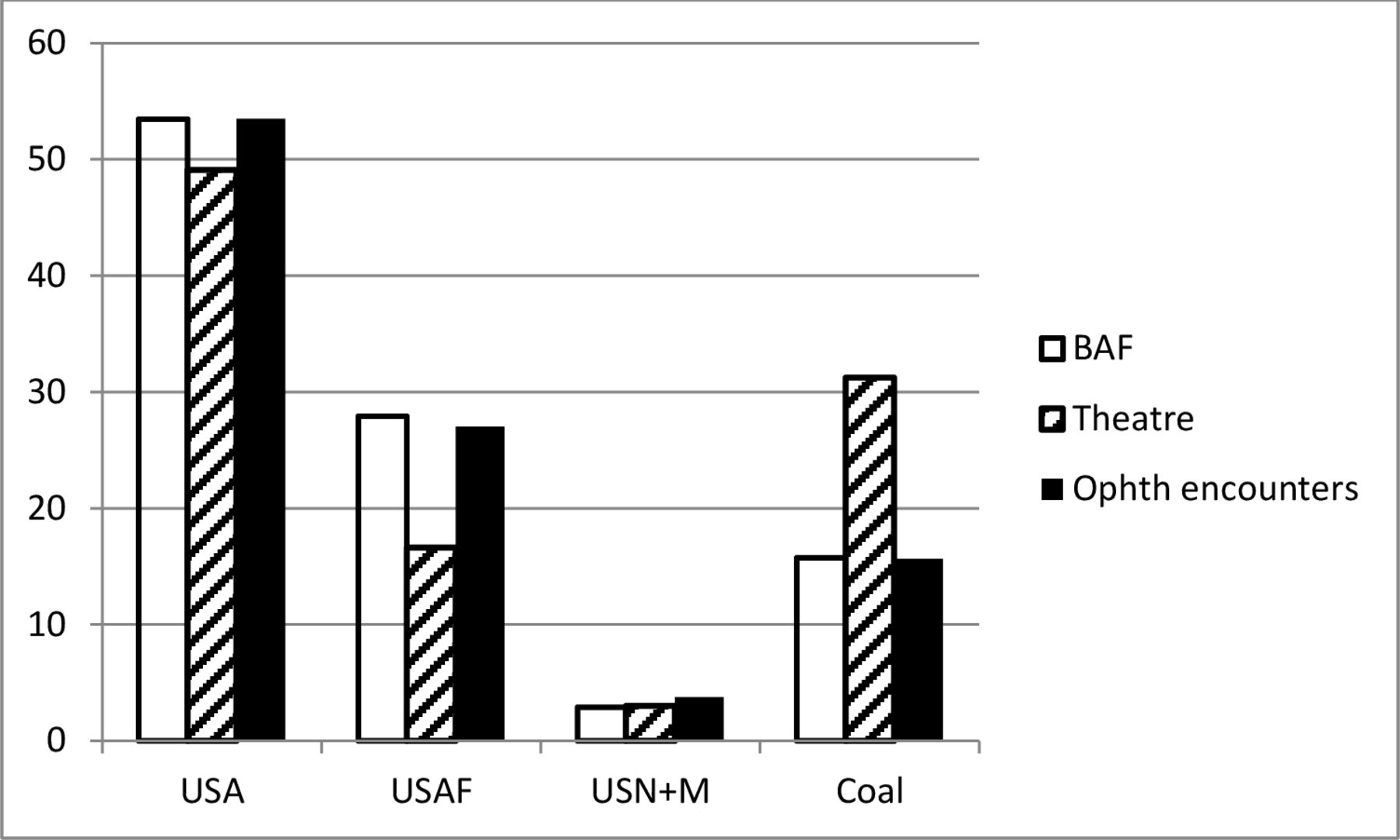
The branch of service of the patients seen provides further evidence of the effect of access to care by location (Figure 2). There was no evidence of a difference in proportion of personnel in each branch of service between those stationed in BAF and those seen by ophthalmology (χ2 0.545; p=0.909), but there was strong evidence for a difference between the proportion of personnel in each branch of service throughout the theatre of operations and those seen by ophthalmology (χ2 27.3; p<0.001).
{kind=link}
{kind=link}
Proportion of personnel in each branch of service at different locations within Afghanistan compared with the proportion of patients seen from each branch of service. BAF, Bagram Airfield; Coal, coalition forces; USA, US Army; USAF, US Air Force; USN+M, US Navy and Marine Corps (collapsed to a single group for statistical purposes because of small numbers).
Aeromedical evacuation out of the theatre of operations
Cases that would be likely to require aeromedical evacuation were an ophthalmologist not deployed to assess and manage their ocular disease in theatre, excluding local nationals, were identified based on expert consensus by a UK and US ophthalmologist (RJB and WGG). These cases included closed globe injury with hyphaema only, posterior vitreous detachment, uveitis, laser exposure with symptoms of visual disturbance (two cases), central serous chorioretinopathy, bacterial and marginal keratitis, cataract, orbital cellulitis, recurrent erosions, retinal detachment, herpetic keratitis, herpes zoster ophthalmicus, neuro-ophthalmic pathologies, retinal vascular disease and keratoconus. We also included cases with refractive problems that may not have been recognised as such and would be unlikely to be resolved without an ophthalmology or optometry consultation. We also included cases of viral and chlamydial conjunctivitis (the cases of viral conjunctivitis had impressive mostly unilateral subepithelial infiltrates and corneal oedema and/or reduced vision that did not respond to initial treatment and required ophthalmology consultation). On this basis we identified 89 patients (36% of 247) who would be likely to require evacuation, were an ophthalmologist not deployed in theatre, compared with the 13 who were actually evacuated. We considered this a conservative estimate, as there were likely other cases that would have required evacuation, such as closed globe injury (without hyphaema), chemical injury and several patents who required in theatre aeromedical transport for corneal foreign body removal. Patients without pathology identified may also sometimes be evacuated for symptoms. Patients with migrainous visual symptoms or dry eyes often were referred, and sometimes aeromedically transferred within theatre, as were other visual disturbances including transient monocular visual loss.
Discussion
During the time covered by the study there were approximately 6000 US and coalition service members local to BAF for whom CJTH was their main provider of healthcare, of whom 146 had consultations for ophthalmic DNBI (Figure 1), giving an ophthalmic DNBI rate of 0.2% per month or 2.43% per year and of whom 97% were returned to duty in theatre (95% of all military and contractors returned to duty). We estimate that without an ophthalmologist present, 36% of patients would require aeromedical evacuation out of theatre, compared with the 5% evacuated with an ophthalmologist present. At 30–90 consultations per month, ophthalmology was the busiest of all the surgical and outpatient secondary care specialties and second only to primary care in the number of consultations per physician.
Psolka et al reported the distribution of diagnoses for 107 ophthalmic DNBI cases evacuated to Walter Reed,12 of which the most common diagnosis was uveitis (13.1%; four cases anterior), followed by retinal detachment (11.2%), infectious keratitis (4.7%) and choroidal neovascularisation (4.7%), similar to our data in which 12 patients had uveitis (11 anterior). In contrast, to our data, we only evacuated one case of bilateral intermediate uveitis with elevated intraocular pressure, the rest being treated in theatre and returned to duty. The diagnosis list of patients evacuated in the paper of Psolka et al is notable for 19 patients who were evacuated for minor and self-limiting problems, including dry eye, subconjunctival haemorrhages, corneal abrasions, foreign bodies, conjunctivitis, blepharitis, pterygia, physiological anisocoria, chalazion and refractive error, which suggests that in these cases initial assessment occurred at a location without an expeditionary ophthalmologist, but may also reflect less mature and less well-equipped Role 3 facilities at an earlier stage in the conflict. In estimating the number of aeromedical evacuations avoided by in-theatre ophthalmology assessment, we did not include many of these minor conditions such as corneal foreign bodies and blepharitis, therefore the true number of aeromedical evacuations prevented was probably much greater than our estimate of 76.
The presence of a single ophthalmologist within the theatre of operations over this 11-month period therefore prevented at least 76 military personnel and contractors being evacuated. In the current environment of small unit deployments and significant limits on the number of personnel deployed, the loss of even one or two soldiers can have significant effects on unit capability and deployed ophthalmology is therefore critical in maintaining operational readiness and combat effectiveness.
The low proportion of cases transferred for evaluation from other locations and the similarity in branch of service between patients seen at CJTH and service personnel stationed at BAF suggests that access to ophthalmic care for DNBI is dependent on the presence of an ophthalmologist at the deployed location, as previously demonstrated for ocular trauma.13 ‘Minor’ pathologies were less likely to be transferred for evaluation than potentially serious pathologies (such as retinal and neuro-ophthalmic disorders). However, the proportion of cases seen from other locations was lower than expected, given that only 30% of personnel in the area of operations were stationed at BAF, while only 15% of those seen in ophthalmic consultation were stationed outside of BAF. It is possible that commanders and medical personnel at other locations took into account the risks to patients and aircrew of in-theatre transfers and were reluctant to transfer patients for complaints that they perceived to be minor. While this is a valid concern, the number of serious pathologies seen from outside of BAF was also lower than expected and there is a risk of morbidity such as permanent corneal scarring or perforation after bacterial or herpetic keratitis and raised intraocular pressure associated with hyphaema or uveitis. We do not have data on the ophthalmic presentations to other medical facilities in the area of operations or the rate of aeromedical evacuation from those locations and it is therefore likely that the figures reported here most accurately reflect ophthalmic DNBI for the service population at risk around CJTH, numbering roughly to 6000 personnel.
For the period of conflict in Afghanistan from 2002 to present, ophthalmology has been a theatre-level asset, provided only at BAF to cover the entire area of operations in Afghanistan, except for 2010–2012, when a US Navy ophthalmologist was also stationed at Kandahar. It is possible that improved access to teleophthalmology consultations could improve access to care at remote locations and mitigate some of this risk.14 An expeditionary ophthalmologist at a Role 3 could possibly extend ophthalmic care to Role 1, Role 2 or Role 3 in theatre using teleophthalmology. With increasing subspecialisation in ophthalmology, it is also possible that teleophthalmology could benefit the local ophthalmologist, who is often practising outside his own area of expertise, to extend subspecialist opinions and reduce out-of-theatre evacuations. Current communication with the Role 3 ophthalmologist is often limited to non-secure or secure Defense Switched Network phone, satellite phone or cellular phone if Wi-Fi is available. In less time-sensitive cases, the web-based HIPAA (Health Insurance Portability and Accountability Act of 1996) secure teleconsultation systems developed by the Navy called Health Experts Online Portal or Pacific Asynchronous TeleHealth are available.
Heier et al found that 108/767 ED visits (14%) were for ophthalmic complaints,11 with a comparable case mix, but only one patient with dry eye (keratoconjunctivitis sicca) and more frequent corneal foreign bodies (18 patients of which one required medevac) and ocular surface burns (14 patients of which four required medevac). The proportion of patients evacuated out of theatre was higher (20/108 vs 13/281) and detail on diagnoses was limited by the lack of an expeditionary ophthalmologist (eg, six patients with diagnosis listed as ‘decreased visual acuity’) and ophthalmic equipment as currently provided.
Stalker et al reported 565 ED encounters with eye problems to the UK Role 2 enhanced treatment facility at Camp Bastion, Afghanistan, between 2006 and 2009, which formed 5.1% of the total ED workload in that period, but did not report the diagnostic breakdown.15 Our figures are comparable to that.
The limitation of this retrospective study is the potential for incomplete data collection. We were able to detect all ophthalmology outpatient notes, but were unable to search inpatient notes. Therefore, if patients admitted from clinic had notes made on the inpatient system only, we may not detect these cases; however, such patients would usually attend through the ED and have ED consultation notes with an ophthalmic diagnosis, which we would have detected. We consider that very few patients would have been missed in this way, as no examples occurred in the period from July to August 2019 when RJB and WGG were at CJTH.
Contact lens-related eye infections were reported in five cases by Heier et al in 1993 and were flagged as a significant problem in British operations in Iraq and Afghanistan in 2010 by Musa et al, who reported 27 cases.11 16 Despite clear advice from UK and US chains of command not to wear contact lenses on deployment and the ready availability of refractive surgery options to US service personnel, we report three cases of contact lens-related bacterial keratitis (two US Army, one contractor). Of note, we report no complications of refractive surgery in US military personnel despite its widespread uptake.
The high number of local nationals seen for trauma presentations highlights an additional role for deployed ophthalmology. While these patients are entitled to care within the deployed medical facilities, they are not usually entitled to evacuation out of country and would therefore have limited access to ophthalmic care were deployed ophthalmology not present.
We report for the first time the ophthalmic DNBI rate of deployed US and coalition forces, defining the need for deployed ophthalmology in terms of DNBI management. We have also estimated the value of deployed ophthalmology in terms of a sevenfold reduction in aeromedical evacuation and a greater return-to-duty rate after ophthalmic complaints.
Data availability statement
No data are available. The data are clinical data and it would not be appropriate to share it, nor do we have permission to do so.
Ethics statements
Patient consent for publication
Ethics approval
This project was approved as a performance improvement initiative by the US Central Command (CENTCOM) command surgeon. It was reviewed by the US Army Medical Research and Development Command’s Office of Research Protections, Institutional Review Board Office, and given a Not Research Determination.
References
Footnotes
Contributors All authors collected the data and reviewed and edited the final version of the manuscript. RJB and WGG conceived, obtained approvals and ran the study. RJB wrote the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.