Article Text

Abstract
Introduction Modern military combat helmets vary in their shapes and features, but all are designed to protect the head from traumatic brain injury. Recent recommendations for protection against energised projectiles that are characteristic of secondary blast injury is to ensure coverage of both the brain and brainstem.
Method Graphical representations of essential coverage of the head (cerebral hemispheres, cerebellum and brainstem) within an anthropometrically sized model were superimposed over two standard coverage helmets (VIRTUS helmet, Advanced Combat Helmet (ACH)) and two ‘high-cut’ helmets (a Dismounted Combat Helmet (DCH)) and Combat Vehicle Crewman (CVC) helmet), both of which are designed to be worn with communications devices. Objective shotline coverage from representative directions of projectile travel (−30 to +30 degrees) was determined using the Coverage of Armour Tool (COAT).
Results VIRTUS and ACH demonstrated similar overall coverage (68.7% and 69.5%, respectively), reflecting their similar shell shapes. ACH has improved coverage from below compared with VIRTUS (23.3% vs 21.7%) due to its decreased standoff from the scalp. The ‘high-cut’ helmets (DCH and CVC) had reduced overall coverage (57.9% and 52.1%), which was most pronounced from the side.
Conclusions Both the VIRTUS and ACH helmets provide excellent overall coverage of the brain and brainstem against ballistic threats. Coverage of both would be improved at the rear by using a nape protector and the front using a visor. This is demonstrated with the analysis of the addition of the nape protector in the VIRTUS system. High-cut helmets provide significantly reduced coverage from the side of the head, as the communication devices they are worn with are not designed to provide protection from ballistic threats. Unless absolutely necessary, it is therefore recommended that high-cut helmets be worn only by those users with defined specific requirements, or where the risk of injury from secondary blast is low.
- trauma management
- neuroradiology
- oral & maxillofacial surgery
Data availability statement
Data are available on reasonable request.
Statistics from Altmetric.com
Key messages
Modern military combat helmets vary in their shapes and features, but all are designed to protect the head from traumatic brain injury.
The aim of this research was to objectively compare the head coverage provided by a selection of four representative combat helmets.
Both the VIRTUS helmet and the Advanced Combat Helmet provide excellent overall coverage of the brain against ballistic threats.
Coverage would be improved at the rear by using a nape protector and the front using a visor.
High-cut helmets provided significantly reduced coverage from the side of the head, which is the most susceptible of all the brain from ballistic threats.
Introduction
Military combat helmets are designed to protect the wearer against the effects of traumatic brain injury (TBI). The requirements for helmets include prevention of perforation the helmet shell by energised fragments (secondary blast) and prevention of the transmission of blunt impact (tertiary blast). In addition, most helmets have a requirement to protect against bumps and low-velocity bullets as well as providing attachments for items such as communications devices.1 More recent iterations of combat helmets incorporate additional components such as communications devices, mandible guards, side rails, multi-functional adaptors and visors (Figure 1). Their use in conflicts since World War 1 has resulted in significant reductions in both mortality and morbidity.2–7 Fatal head injuries are primarily due to bullets overmatching helmets or from fragments penetrating through the face.2 8–11 The literature refers to risk from behind helmet blunt trauma injuries,12 13 but no evidence for such injuries was identified in a recent systematic review.2

Modular components of a helmet system; (A) nape protector on VIRTUS (partly hidden by rear helmet fastenings), (B) visor with mandible guard on VIRTUS, (C) communications device worn with a high-cut helmet.
The coverage provided by a helmet against threats is determined by the position of the helmet edges (trimline),14 the distance between helmet and scalp (standoff),15 and the direction of threat for projectiles (shotline). As technology has advanced, the ability to objectively compare the medical coverage provided by different designs of helmets has improved. Anatomically accurate and anthropometrically representative models of the components of medical coverage enable helmets to be visually and objectively compared. These demonstrate large differences in coverage between commonly used helmets, including between different sizes of the same helmet type (Figure 2). The Coverage of Armour Tool (COAT) is the latest iteration of coverage models, and enables shotline comparisons between armour types from differing horizontal (azimuth) and vertical (elevation) planes.16 COAT was first used to validate new designs of neck collar for the UK personal armour system,16 and was subsequently used as part of the selection of the winning design for the VIRTUS personal armour and load carriage system.17

Representative selection of modern military combat helmets; (A) VIRTUS helmet, (B) Advanced Combat Helmet (ACH), (C) Dismounted Combat Helmet (DCH), (D) Combat Vehicle Crewman (CVC) helmet.
Medical coverage for military helmets against projectiles was defined anatomically in 2015 as protection of the brain and the brainstem.1 This coverage requirement was used in the procurement of the VIRTUS helmet used by UK forces,17 and has also been adopted in version three of the NATO Standardised Agreement (STANAG) 2902 published in 2019.18 This document provides recommendations for helmet design and testing of helmets used by NATO military forces. Although the STANAG is followed for helmets used by the vast majority of military users, it is recognised that other users may use helmets that do not conform to these coverage recommendations because of differing requirements. There are clearly medical implications in the use of helmets with reduced anatomical coverage against projectiles, meaning that they should only be used when absolutely necessary.
The aim of this research was to objectively compare the coverage provided by a selection of current representative helmets using the recommendations specified in NATO STANAG 2902.18 This would demonstrate the potential medical effectiveness of each helmet against ballistic projectiles.
Method
Four helmets were chosen to be representative of a broad selection of those currently worn on current military operations (Figure 2). The Advanced Combat Helmet (ACH) is a commercially available shell shape, iterations of which have been used by the US Department of Defense.19 The VIRTUS helmet has since 2015 progressively replaced the previous Mark 7 combat helmet as the standard UK military helmet.17 20 Both the ACH and VIRTUS helmets are examples of ‘full-cut’ helmets. The Dismounted Combat Helmet (DCH) and Combat Vehicle Crewman (CVC) helmets have a ‘high cut’ design to save weight and enable integration of communications equipment.14 21
Within the male version of the Zygote adapted for use within COAT,22 the head circumference is 57 cm. This can be compared with the mean head circumference of 57.9 cm, found in the latest UK military anthropometric survey.23 The geometries of the four helmets were imported into COAT using .stl files provided by the manufacturers of each helmet. Helmet sizes were chosen that according to the manufacturer fitted that head size. Each helmet was positioned so that the helmet pads or retention straps would sit passively onto the scalp skin.
The anatomical components comprising coverage for helmets in this analysis were the brain (comprising the cerebral hemispheres and cerebellum) and the brainstem.1 The brainstem becomes the spinal cord as it exits the foramen magnum of the skull, and the cut-off between structures was chosen as the most inferior point on the skull adjacent to the foramen.
COAT was used to undertake a shotline analysis comparing the four helmets in 360 degrees (10-degree horizontal azimuth steps) and 10-degree vertical elevation steps (−30 to +30 degrees). A mesh comprising hundreds of infinitely thin straight lines with 2 mm spacing between them was superimposed on the aforementioned anatomical structures. Coverage was described as a percentage, with higher values representing greater coverage. An additional analysis was undertaken to determine the influence of a nape protector on the coverage provided by the VIRTUS helmet (Figure 3).

Close-up of the nape protector on the VIRTUS helmet, with measurements used to enable accurate importation into COAT. The helmet retention system makes the nape difficult to visualise.
Results
Superimposition of the helmets within the Zygote male human anatomy within COAT demonstrates pictorial coverage from a horizontal vector (Figure 4). The ACH and VIRTUS helmets pictorially in the Zygote appear to provide almost identical coverage from the front and side. The CVC provides similar coverage from the front to ACH and VIRTUS. The VIRTUS has slightly reduced coverage from the rear than ACH. From the front, the brain is not covered by any of the four helmets, with coverage the worst for the DCH helmet. All four helmets have similar coverage from the rear, with only part of the cerebellum and brainstem exposed. Coverage differences between helmets are most different from the side.
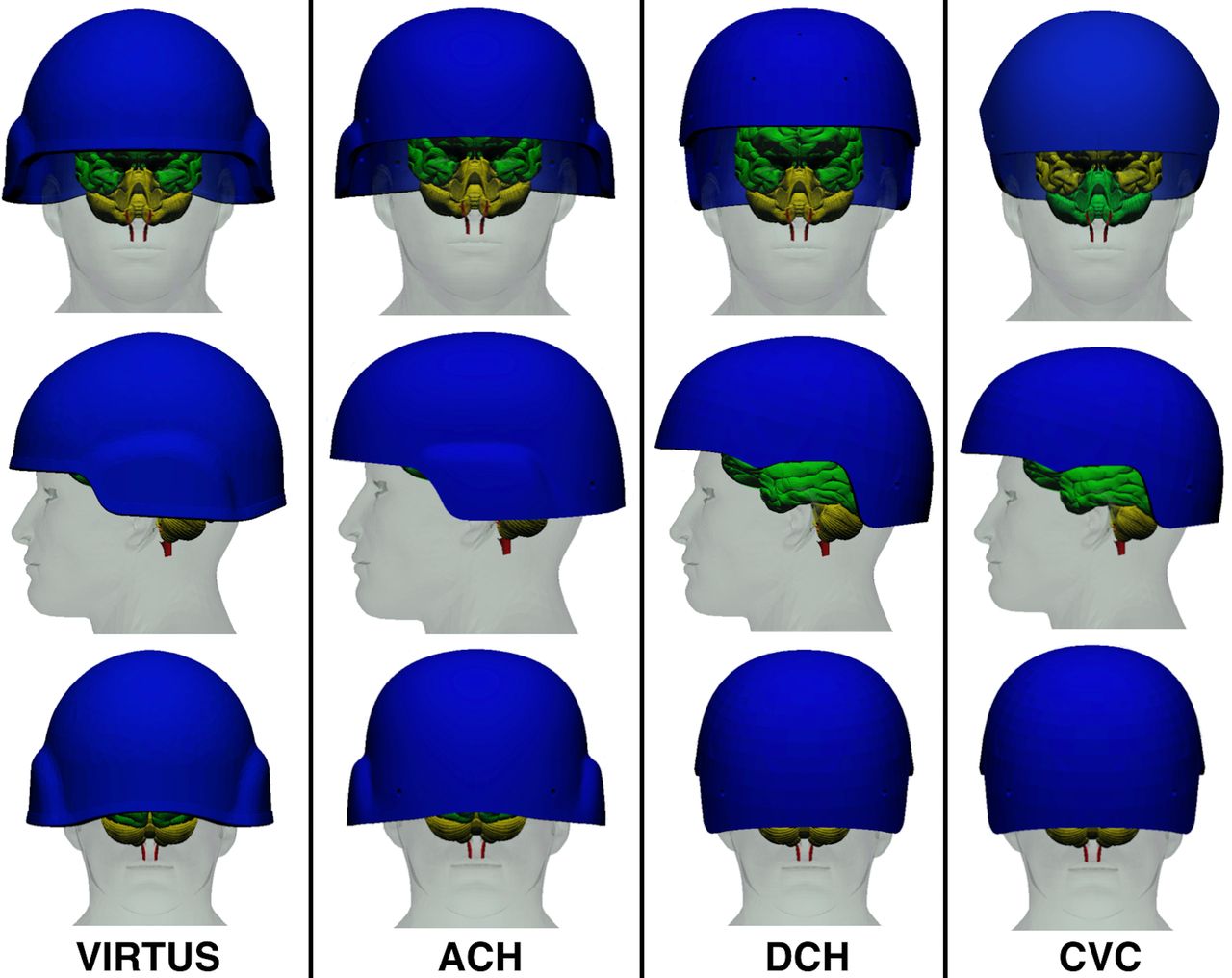
Graphical representation of differing coverage provided by the four helmets of the cerebral hemispheres and cerebellum (green) and the brainstem (brown) in a horizontal plane.
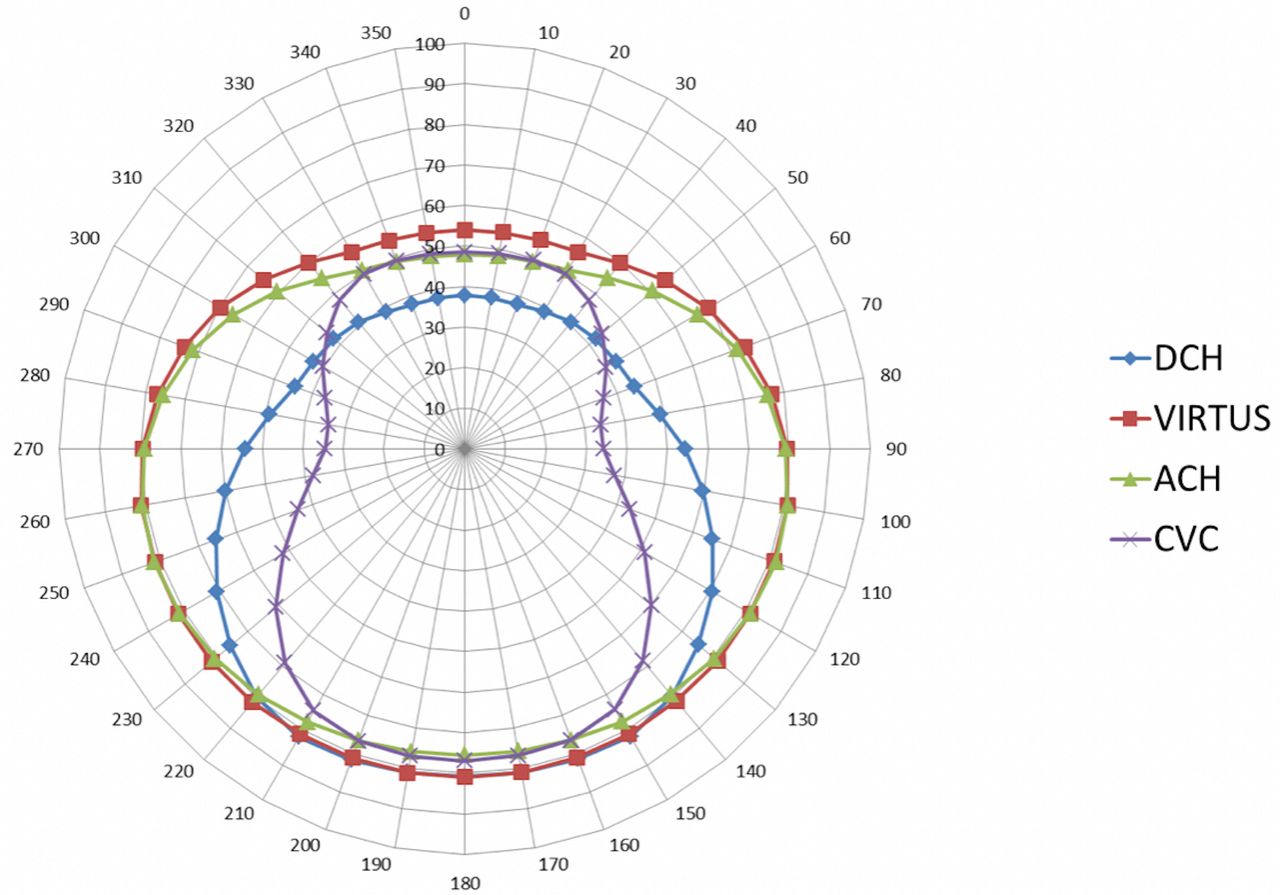
All four helmets demonstrated similar coverage from the front and rear. An example of the coverage provided by the VIRTUS helmet alone is demonstrated in Figure 5. This demonstrates that coverage is greatest from above (elevations of +20 and +30 degrees). From these elevations, coverage is similar from all horizontal azimuths. Coverage is reduced when shotlines originated from below (eg, −30 degrees, dark blue line), which is least from the front. This trend was seen when all four helmets were compared (Figure 5), but coverage was further reduced in the CVC and DCH helmets from the side.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Objective comparison of the four helmets using the Coverage of Armour Tool.
When coverage of all four helmets analysed at all directions were compared (Table 1, Figure 5), the highest coverage was found in the ACH helmet (69.5%) followed closely by the VIRTUS helmet (68.7%), which was greatest when wearing the nape (75.5%).
Comparisons of the per cent coverage of the brain and brainstem provided by four helmets in different angulations of shotlines
Discussion
Contemporary combat helmets protect the brain and brainstem from TBI in addition to other secondary roles, of which TBI is the most common cause of death on the modern battlefield.9 Head coverage should be further subdivided into the cerebral hemispheres, cerebellum and brainstem. This brings the definition of head coverage in line with the more specific anatomical descriptions used for essential coverage to other parts of the body.24 Helmet design has evolved over the years to reflect changes in threats (materials science) but also advances in medical knowledge.3 Although there is a commonly held belief that the majority of head wounds from both bullets and fragments are from the front,4 5 such information is historical and potentially of limited application to current conflicts. Impact locations of head injuries sustained by military forces should be analysed to ascertain if there is variation in the susceptibility of the brain to various threat orientations.
The graphical overlays in Figure 4 demonstrated that following multiple stages of evolution, the VIRTUS helmet and the ACH shells are now almost identical in shape. The objective coverage assessment using COAT confirms that this is reflected in very similar coverage from projectiles in the horizontal plane. The two helmets differ from below due to the reduced stand-off of the ACH from the skin and the higher cut at the rear in the VIRTUS helmet. This may reflect differing requirements of the ACH and VIRTUS towards blunt impact protection and integration with other equipment. The use of a suspension and liner system with VIRTUS increases stand-off from the skin, compared with the pad system used in the ACH,15 and provides improved coverage from threats directed from underneath.
Analyses since WW2 have demonstrated that the temporal and occipital regions are particularly susceptible.3 25 This is an important consideration in so-called ‘high-cut’ style helmets, as it has long been recognised that helmet appearance is often fundamental to user acceptability.3 6 High-cut helmets provide significantly reduced coverage from the side of the head, as the communications devices they are generally worn with are not designed to provide protection from ballistic threats. Unless absolutely necessary, it is therefore recommended that high-cut helmets be worn only by those users with defined specific requirements, or where the risk of injury from secondary blast is low.
This analysis confirmed the positive effect of a nape protector, particularly on the brainstem, which is potentially the most vulnerable region of the brain.9 It is recognised that not all helmets can use nape protectors. However, assuming there are no human factors issues, these results suggest that inclusion of a nape protector in future helmet designs should be encouraged.
A number of limitations to this analysis are acknowledged. One assumption of this analysis is that all of the components of the brain and brainstem are equally susceptible to penetrating injury, and that projectiles are based on 2 mm wide shotlines. However, factors affecting outcome from TBI include volume of injured brain tissue, energy transmission and entry location. It is recognised that the ballistic protective materials used in the nape pads may not be commensurate with the helmet materials or protection levels.
In conclusion, this analysis has demonstrated that both the ACH and VIRTUS helmets provide excellent coverage of the brain and brainstem against ballistic threats. This could potentially be further improved by using a nape protector, and further analysis is recommended to objectively determine the additional effect of this. Although the DCH and CVC helmets provided significantly less medical coverage, this is balanced against their differing requirements in that they are designed to integrate with communications devices. It is, however, recommended that unless there is a specific need to use a high-cut helmet, the use of full-cut helmets will provide much better protection against a threat that remains the most common cause of death on the modern battlefield.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Acknowledgments
Approval for undertaking and publishing this study was obtained from Dstl (Ref: DSTL/CP121059) and the Royal Centre for Defence Medicine (Ref: RCDM/Res/Audit/1036.19.0514 and CC1-20200040). Content includes material subject to © Crown copyright (2019), UK Ministry of Defence. This material is licensed under the terms of the Open Government License. Approval to publish was granted by Defence Equipment and Support.
References
Footnotes
Contributors Design: JB, RNF, JR. Methodology: JB, RNF, JR. Reporting: JB, RNF, JR.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.