Article Text

Abstract
Introduction Hard armour plates provide coverage to essential anatomical structures in the torso that, if injured, would likely be responsible for death before damage control surgery can be undertaken. Existing front and rear OSPREY plates in conjunction with Mark 2 plates used at the sides in current UK Armed Forces personal armour systems are provided in a single size, used by both female and male users.
Methods CT scans of 45 female UK military personnel were analysed. Distances between anatomical structures representing threshold (absolute minimum) and objective (the maximum level of coverage beyond which there is limited further benefit) coverage of the torso were determined and compared with OSPREY and Mark 2 plate dimensions. Sample characteristics were compared with the 2006/2007 UK Armed Forces Anthropometric Survey.
Results No statistical difference was found between sample means for stature (p=0.131) and mass (p=0.853) from those of the anthropometric survey in this sample. The height of both the front OSPREY plates exceeded the threshold coverage (suprasternal notch to lower border of the 10th rib) for all women studied. The height of the Mark 2 plate exceeds the objective coverage from the side for all women studied.
Conclusions Based on a plate height providing threshold coverage of all women up to the 50th percentile, the height of the front and rear OSPREY plates could be reduced by 36mm and 31mm respectively. Based on a presumption that a side plate should cover up to the 95th percentile, the Mark 2 plate achieves the objective height and width for the female population studied. Strong evidence was found to support the UK Ministry of Defence requirement for procurement of new front and rear plates of multiple heights for both female and male users.
- Gastrointestinal imaging
- ORAL & MAXILLOFACIAL SURGERY
- Facial plastic & reconstructive surgery
Data availability statement
Data are available upon reasonable request. No data are available.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Hard armour plates provide coverage to those essential anatomical structures in the torso that are responsible for death before damage control surgery can be undertaken.
Large OSPREY plates insert into the front and rear of the VIRTUS Scalable Tactical Vest with Mark 2 plates worn in the sides.
WHAT THIS STUDY ADDS
This study analysed CT scans in combination with information derived from an anthropometric survey to measure the boundaries of those structures in the torso requiring protection.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Strong evidence was found that multiple sizes of plate would best protect both the female and male current UK military populations.
Introduction
Essential medical coverage
War injury is characterised by high and early lethality. A recent review demonstrated that 57% of Armed Forces personnel killed in action in contemporary conflict died immediately and >90% died within 1 hour of wounding.1 This review included death from head injury, and when these patients are excluded, the proportion of immediate deaths is 29.7% and the deaths within 60 min of injury was 52.1%.1 Personal armour exists to mitigate the injurious effect of war injury and a balance must be struck between high levels of protection and the mobility and comfort of the user.
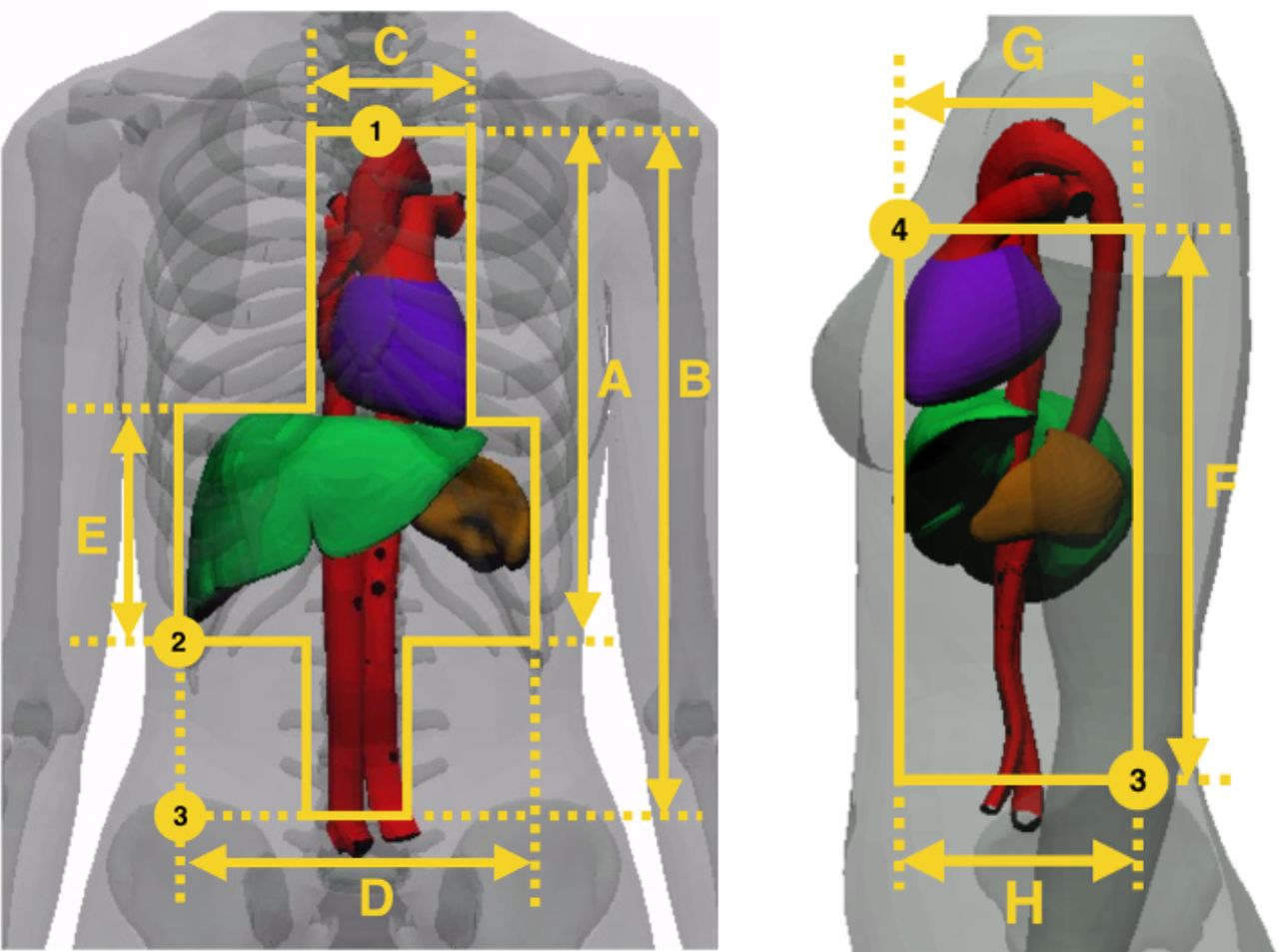
In 2016, Breeze et al defined those structures in the torso as requiring essential medical coverage by a ballistic plate as the heart, great vessels, liver and spleen.2 Such essential medical coverage reflects protection of those anatomical structures, which if injured are likely to result in death within 60 min of injury (Figure 1). This definition of essential coverage was subsequently modified to reflect those structures that would likely result in death prior to damage control surgery (DCS) being performed.3 For example, bleeding from the thoracic component of the torso cannot be compressed and requires surgical thoracotomy to arrest it. NATO doctrine recommended that DCS should be performed ‘within 60 min but no more than 2 hours post injury’.4

Female internal anatomical structures used to determine essential coverage from the front and side. Numbers are exterior landmarks and refer to the following: 1, suprasternal notch; 2, 10th rib; 3, Iliac crest; 4, anterior axillary fold. Table 2
Personal armour used by UK Armed Forces
Combat body armour (CBA) (without hard plates) was introduced in the 1980s, and enhanced combat body armour (ECBA) was introduced in 1991, which augmented the CBA vest with front and rear plates to provide ballistic protection to the heart. These plates were termed the ‘protective plate, contoured, armour, body, Mark 2’ but are colloquially known as ECBA plates. OSPREY body armour, with larger OSPREY front and rear plates, was introduced in 2005 and can also use Mark 2 plates as front and rear protection.5 Later versions of OSPREY incorporated the ability to use the Mark 2 plates as side protection.
In 2015, the VIRTUS body armour and load carriage system was issued to the UK Armed Forces. VIRTUS retains the OSPREY front and rear plates and pockets to include Mark 2 plates as front and rear plates and pouches for use as side armour. Essential medical coverage of the torso for UK Armed Forces is currently provided by the OSPREY hard armour plates secured in the VIRTUS Scalable Tactical Vest (STV). The soft armour included within the STV provides protection against low velocity fragmentation to those anatomical structures potentially responsible for mortality not fitting the requirement for essential coverage as well as those causing morbidity necessitating lifelong medical treatment or that result in significant disability, known as desirable medical coverage.1
Hard armour plates to provide threshold and objective coverage
The minimum sizes of hard armour plates should be informed by essential coverage of internal anatomical structures. These internal structures can additionally be related to external anthropometric landmarks, allowing design and fitting requirements to be communicated to non-medically trained personnel. For example, the suprasternal notch can be related to the arch of the aorta, the 10th rib to the lower border of the liver and the superior border of the iliac crest to the bifurcation of the aorta.2 The minimum size a front or rear plate must achieve has been defined as ‘threshold’, supplemented ideally with coverage of additional anatomical structures defined as ‘objective’.3 For side coverage, the maximum upper height that hard armour can physically fit is the anterior axillary fold; hence, this defines the upper limit of both objective and threshold side coverage. The lateral lower height bound is informed by the configuration of the STV.
Coverage of the torso in women
All definitions for medical coverage of the torso for female users are concordant with previous definitions agreed for male coverage.2 5 6 This reflects that the internal anatomy of the torso of women and men is identical; it is the external anatomy of the torso and the anatomy of the pelvis (containing the reproductive organs) that differs between men and women. This differing external anatomy can make threshold and objective values more difficult to measure by non-specialists. The first medical analysis of coverage specifically for female users in the world literature was an Australian pilot study of three civilian women using magnetic resonance (MR) scans of the torso, but this was too small a sample to enable any medical coverage conclusions and is likely to be unrepresentative of the UK Armed Forces population.7
The aim of our research was to derive dimensions for essential coverage to optimise future plate sizes for female users using a larger cohort of female UK Armed Forces personnel. This research represents the first clinical and scientific collaboration as part of the newly formed cross-disciplinary UK Ministry of Defence (MoD) Personal Armour Clinical Interface Group.
Method
CT scan sample identification
A search was performed to identify all female UK Armed Forces personnel who had undergone a CT scan of the torso at the University Hospitals Birmingham (UHB) NHS Foundation Trust between January 2011 and December 2018. This cohort included CT scans undertaken when the service person was deployed in a combat zone (such as to Afghanistan) with scan data being subsequently transferred to the UHB system for analysis and archiving; such scans were identified using the UK Joint Theatre Trauma Registry. These scans were cross checked with and supplemented by scans performed at UHB for disease and non-battle injury; such scans were identified using records held by the imaging department of the Royal Centre for Defence Medicine. The mass, stature and ages of these individuals were identified from their clinical record but were kept anonymised.
Sample validity
To ensure that the sample obtained from CT was representative, it was compared with the values of the 311 UK Armed Forces personnel measured in the 2006/2007 UK Anthropometric Survey.8 Mean values for mass, stature (height when vertical) and age were compared using an unpaired Student t-test with a p-value threshold for significance of <0.05. Data analysis was performed using Stata for Mac V.15.1.
Measurements used for determining threshold and objective coverage
Distances were measured between the borders of structures and associated anthropometric landmarks for threshold and objective coverage of the torso in the axial plane (Table 1) in the same manner as that used for men,5 6 as described further:
Threshold: suprasternal notch to the 10th rib (ie, the absolute minimum coverage).
Objective: suprasternal notch to the iliac crest (ie, the coverage which is aspired to).
Anthropometric measurements derived from this study of CT scans and compared with those derived from the 2006/2007 UK military anthropometric survey8
Vertical measurements were made by determining the number of slices between landmarks and multiplying that value by slice thickness used (1.0, 1.25 or 3.0 mm). Horizontal measurements were made using the intrinsic measuring tool of the IMPAX imaging program V.6.0 (Agfa, Belgium) that provides linear distances between two cursor points in millimetres (Figure 2). Measurements were made by two authors, with three attempts at each measurement made by each author with the resultant mean value rounded up to nearest 0.5 mm.

(A) Heart width (127 mm) was used as part of the determinate for the upper plate width, and the anterior border of the heart to the posterior border of descending aorta was used for the side plate width (122 mm). (B) The lower front plate width was from the most lateral borders of the liver and spleen (rounded to 266 mm). The lower side plate width is from the anterior to the posterior border of the liver (rounded to 155 mm).
Comparison of medical coverage dimensions with OSPREY plates
Linear distance measurements of the front and rear OSPREY plates and the Mark 2 plates were taken from edge to edge of the plates while resting on a horizontal surface due to the curvature of the plates (Figure 3).

{kind=link}
{kind=link}
{kind=link}
Comparison of existing plate heights to threshold coverage for female and male personnel; male data derived from a previously published study.6
Results
Between January 2011 and December 2018, 45 CT scans were identified that showed the anatomical landmarks required for analysis (Table 1). Comparison of the CT scan population versus the anthropometric survey population demonstrated no statistical difference between sample means for stature (p=0.1310) and mass (p=0.8526). The soft tissue landmarks for the coverage of the torso from the front and side for different percentiles are demonstrated in Table 2.
Percentile ranges of soft tissue measurements from CT scans, all given in millimetre.MeasurmentscorrespondwithFigure1.
The three surface bony landmarks were able to accurately represent the position of each underlying soft tissue structure as shown further:
Distance of the suprasternal notch is above the aortic arch: −56 to+48 mm (mean 3 mm).
Distance of the 10th rib is below the lower border of the liver: −3 to+46 (mean 11 mm).
Distance of the iliac crest is below the aortic bifurcation: −4 to+36 (mean 20 mm).
Table 3 and online supplemental Figures 1–3 demonstrate measurements of threshold and objective coverage for the front, rear and side compared with OSPREY front and rear plates and Mark 2 side plates. The height of the front OSPREY plate (334 mm) is larger than all threshold lengths and corresponds to the 33rd percentile objective length coverage of women in this study. The height of the rear OSPREY plate (329 mm) is larger than all threshold lengths and corresponds to the 27th percentile objective length coverage of women. The height of the Mark two plate (214 mm) was less than the threshold coverage from the side in all women in this study. The width of the Mark 2 plate (162 mm) corresponds with threshold coverage width of 92nd percentile female in this study. The lower widths (distance between outer border of liver–spleen) of the population in this study were within 2.5% of the widths of the front and rear OSPREY plates.
Supplemental material
Supplemental material
Supplemental material
Measurements required to determine essential medical coverage for the torso from the front, rear and side: SSN=suprasternal notch
Figure 3 shows a comparison of female and male threshold length coverage. The largest female threshold length in this study corresponds to an 80th percentile male, and the smallest male corresponds to the 5th percentile female threshold length in this study.
Discussion
This is the first UK female Armed Forces study conducted that provides objective evidence to quantify the potential size ranges of hard armour plates specifically for the female user population. Using CT scans of active female Armed Forces personnel is the most representative method currently available. Stature, mass and age ranges in our study were comparable to those identified in the 2006/2007 anthropometric survey.8 As with the previous male study, the external landmarks described herein have already been adopted by UK MoD to describe coverage of armour requirements, used to guide the sizing and fitting of armour, and will be used to determine threshold and objective dimensions of future hard plates when data from representative and up-to-date anthropometric datasets are available. Results for heart width and liver length were also comparable to the only other study on imaging of women in the literature where three female civilians had an MR scan.7
As with the male population data, the mean distances between anthropometric surface bone landmarks and the underlying soft tissue structures were close approximations,5 6 with the suprasternal notch situated, on average, 3 mm above the aortic arch, the 10th rib 11 mm below the lower border or liver, and the iliac crest 20 mm below the aortic bifurcation. However, there was a larger range in values for the suprasternal notch to the aortic arch (−56 to +48 mm) for women than for men (−20 to +27 mm). It is therefore possible for a very small proportion of women that a plate that sits at the suprasternal notch does not cover all of the arch of the aorta. This was, however, a small sample and was undertaken from CT scans in which the person was lying supine; further research is required to understand if this is the case when women are imaged upright.
The heights of the existing front and rear OSPREY plates were greater than the threshold coverage measurements for every female measured in this study. Hypothetically, if a plate height was designed on the 50th percentile for the threshold measurement of women, it could mean that the heights of the front and rear OSPREY plates would be reduced by at least 36mm (13%) and 31mm (12%), respectively. A previous study on men have shown that horizontal coverage does not correlate to vertical variations.6 It was postulated that should only a single width of plate be required, then one option would be to choose a plate which fits all men up to the 95th percentile. Using this premise for the female dataset in this study, we found that the width of the rear OSPREY plate could be reduced by 6% and the front plate reduced by 4%. If a smaller percentile was chosen instead, these plate widths could be reduced further. Reducing the dimensions of a hard armour plate for smaller users will reduce both its mass and thermal burden and potentially improve user fit and function in terms of mobility and equipment integration.9
With regard to side coverage, the width of the Mark 2 plate (162 mm) is very similar to the 95th percentile female measurements in this sample (166 mm). This was also found to be the case for men, showing that the width of side coverage is similar between sexes.5 The height of the existing Mark 2 side plate (214 mm) was less than the threshold height measurements of every woman in our study (the smallest value was 271 mm). This also corresponded with the side coverage analysis of men. However, just like with the male population, increasing the height of the existing side plate would likely to be unacceptable in terms of human factors for female users.
Limitations
Due to the relatively limited number of subjects (n=45) in this study, caution should be taken with basing conclusions on the extremes of the dimension predictions. This can be seen in Figure 3, where the lower and upper percentiles of the objective coverage do not follow a normal distribution. The comparison between male and female dimensions follow a similar trajectory from the 1st to the 97th percentiles. Increasing the sample size by using external anthropometric measurements of the bone landmarks will increase confidence in the extreme percentiles.
OSPREY and Mark 2 hard plates have a curved profile which was designed to provide a better fit to the chest and to improve comfort when worn. Care, however, must be taken when defining the dimensions of curved hard plates, and they are not measured along the curve of the plate itself. Instead (as was done in this paper), the plate should be measured from the linear edge-to-edge two-dimensional distance. Another important limitation of this research is that it does not account for the fit of the hard plate (while integrated with the vest), which can have a large effect for women, as the breast size and shape could alter the position of the plates and affect the anatomical coverage provided.
Conclusions
Based on a plate height providing threshold coverage of all women up to the 50th percentile, future front and rear plates could be reduced by 13% and 12%, respectively, when compared with current OSPREY plates. Based on a presumption that a side plate should cover up to the 95th percentile, the Mark 2 plate is the correct width for the female population studied; alteration of the height measurement should be informed by further human factors evaluation. This analysis of CT scan data has identified strong evidence to support a recommendation for UK Defence to procure ballistic hard armour plates of multiple heights for both male and female users.
Data availability statement
Data are available upon reasonable request. No data are available.
Ethics statements
Patient consent for publication
Ethics approval
Approval for undertaking this study was obtained from the Royal Centre for Defence Medicine (RCDM, reference number 1036.16.0456) and University Hospitals Birmingham (reference number CARMS-15201). The authors were advised that additional specific ethical approval was not required from the Defence Medicine Services Research and Strategy Group as this was a retrospective analysis of data obtained from imaging already undertaken for clinical reasons, and no patient identifiable information was promulgated in the paper. Permission to publish was individually granted by Defence Equipment and Support, Dstl and RCDM.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors JB: conceptualisation, data collection, data analysis, project administration and writing. RNF: conceptualisation, data analysis and writing. DB: writing. IG: data collection and writing. EL: conceptualisation, project administration and writing. JB acts as the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.