Article Text

Abstract
As an organisation, locality or nation, there is a growing need to respond to a wide range of incidents and emergencies that could affect health and the care of patients. Responses to both domestic and international incidents have shown that collaboration, understanding and joint responses across organisations have improved the outcome of those affected by incidents which impact on health. Emergency response is something that is of increasing importance and has been tested on multiple occasions during recent events in the UK. Regarding health, the aim is to respond rapidly and efficiently, reducing potential morbidity and mortality to the lowest possible level in a given circumstance. This paper discusses what is meant by EPRR (Emergency, Preparedness, Resilience and Response), types of potential incidents, how we collectively prepare for responding and what has been learnt during recent events. It concludes with an outline of some selected current activity and highlights the likelihood of increased cross-sector working in EPRR.
- public health
- organisation of health services
- risk management
- trauma management
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
Threats requiring EPRR continue and are likely to increase.
Cross-organisational response is shown to be effective, particularly when there are large numbers of casualties.
Problems regarding communication and data sharing are frequently cited as issues by multiple response organisations.
A commonly understood language between all organisations is vital.
Regular exercising and stronger links between responders will improve future responses.
Trauma response has often been a stimulus in developing EPRR, alternative responses such as those to pandemics, natural disasters and CBRN should also be considered.
EPRR has become the term used among government organisations and category 1 responders involved in threat assessment and subsequent response to emergency incidents.
Responsibilities for EPRR in the health sector are outlined in a paper by the Department of Health to ‘ensure that the health sector can provide an effective response to the whole range of incidents and outbreaks’.1 The Civil Contingencies Act 20042 is the central legislation on which EPRR is based on and uses the following definitions:-
E Emergency
An event or situation which threatens serious damage to human welfare in the UK or in a part or region.
An event or situation which threatens serious damage to the environment of the UK or of a part or region.
War, or terrorism, which threatens serious damage to the security of the UK.2
P Preparedness
The extent to which emergency planning enables the effective and efficient prevention, reduction, control, mitigation of and response to emergencies.3
R Resilience
Ability of the community, services, area or infrastructure to detect, prevent and, if necessary, to withstand, handle and recover from disruptive challenges.
R Response
Decisions and actions taken in accordance with the strategic, tactical and operational objectives defined by emergency responders.
The full scope of EPRR therefore ranges from threat assessment and training, through to exercising and responding to incidents. The roles, responsibilities and required action from various agencies are in the form of standard operating procedures which are continually reviewed and adapted as experience and techniques are gained from sequential responses. The scope of each response ranges from a local level through to an international multiagency response, depending on the type of incident and the resources required.
Types of incident
Incidents can be classified as simple or compound, compensated or uncompensated and natural or man-made. Most incidents are ‘simple (environment intact), compensated (patient load less than capacity available) and man-made’.4 EPRR response can be involved in any of these types of incident, although it often focuses on uncompensated situations where the ‘business as usual’ capacity is exceeded and emergency arrangements and action are required. Divisions regarding the type of incident are often inconsistent across the literature and organisations. Subjective interpretation is common and multiple subdivisions of category are often applied.5 Although these subdivisions are often self-descriptive, incidents are also referred to by ‘type’, examples of which are shown in table 1.
Types of events
Risk of event
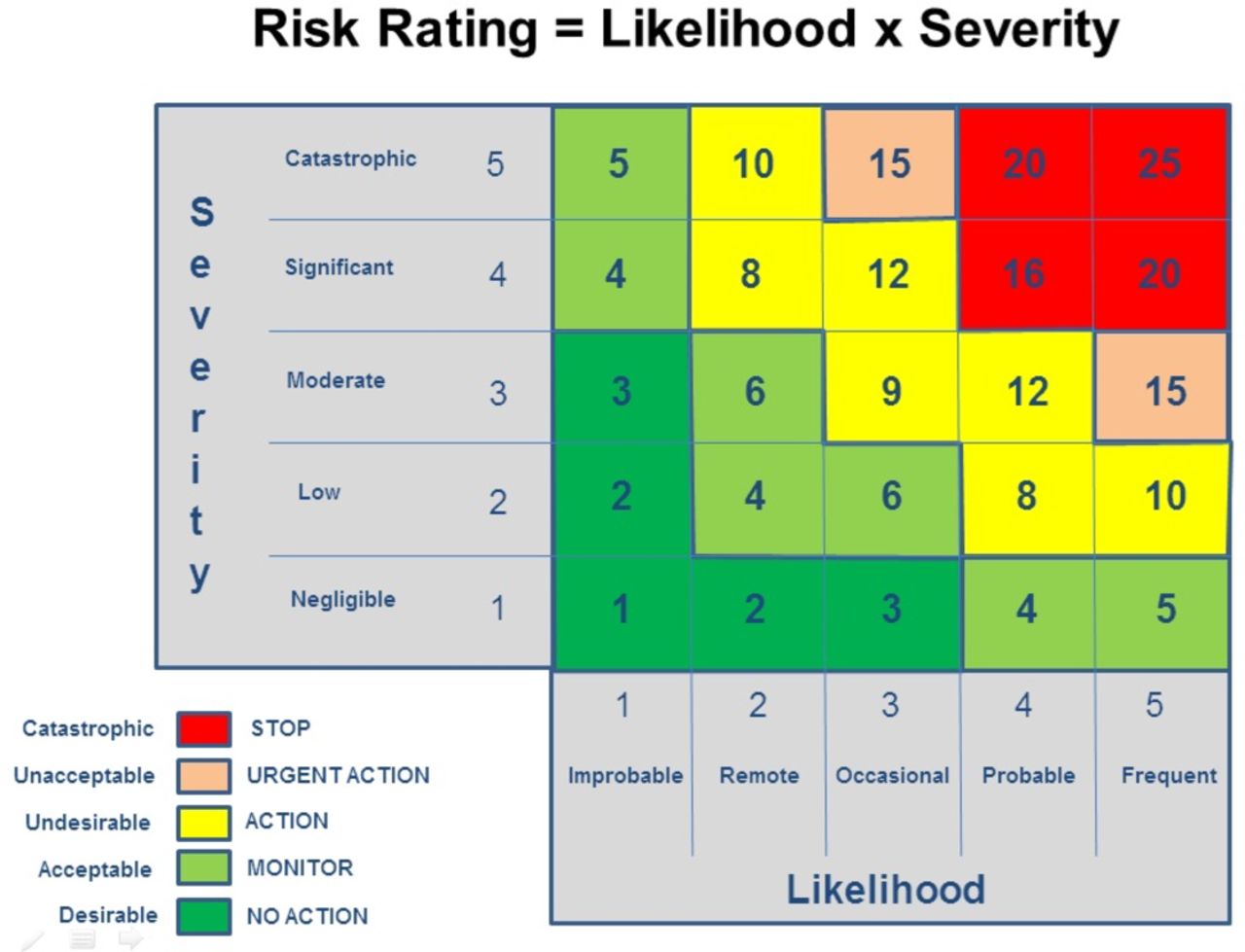
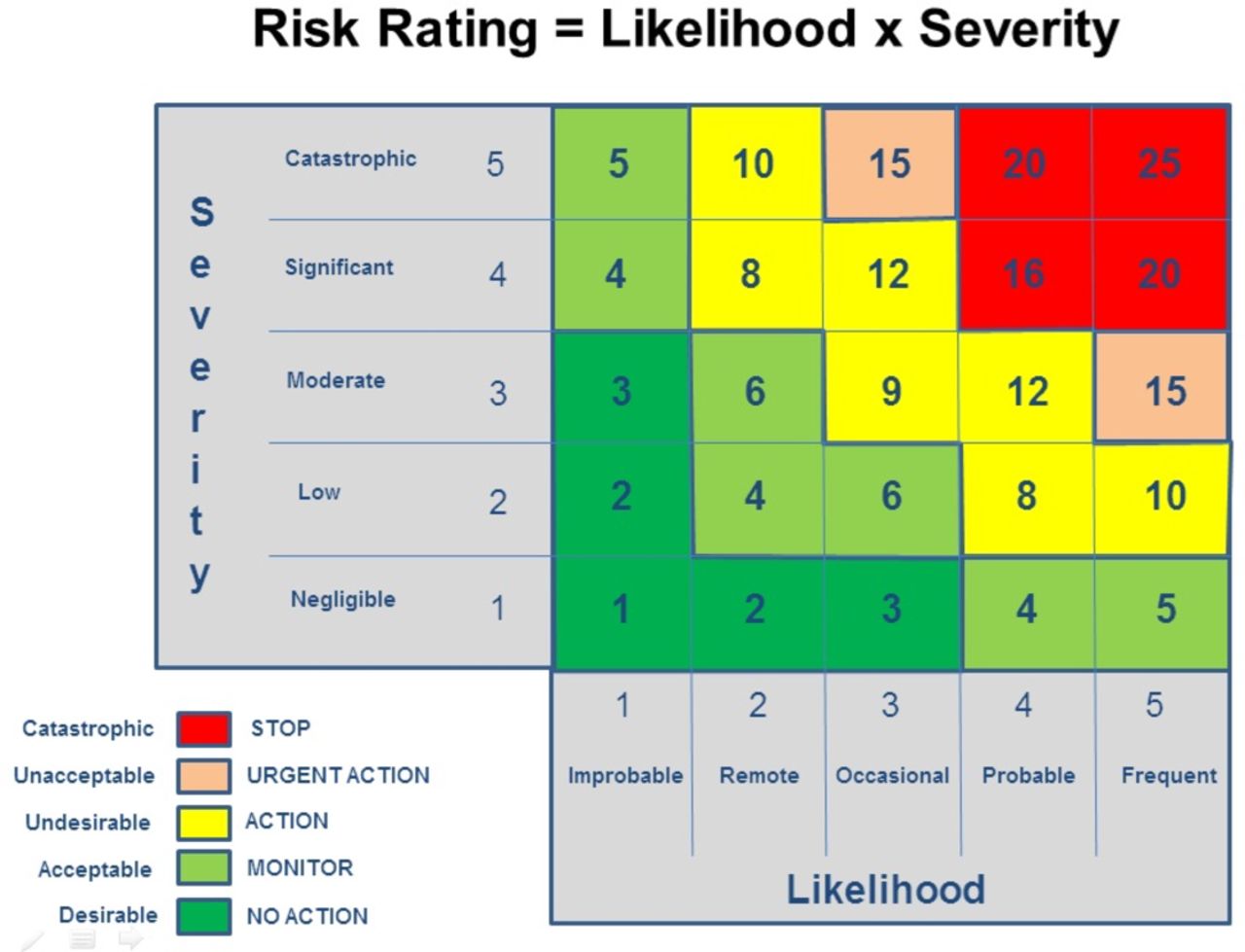
The National Risk Register of Civil Emergencies (figures 1 and 2)6 is produced regularly and uses a standard risk matrix (figure 3) which plots the potential impact of a given event against the likelihood of its occurrence. This technique of risk estimation is used across academia, government and business and is straightforward to understand, although the interpretation of likelihood is open to wide subjective interpretation. An obvious advantage is the production of a one-page illustration of a given situation that can be shared across an organisation and beyond. Regarding National Civil Risk, pandemic influenza has consistently ranked as one of the most severe threats with the greatest potential impact since the inception of the register in 2008.7
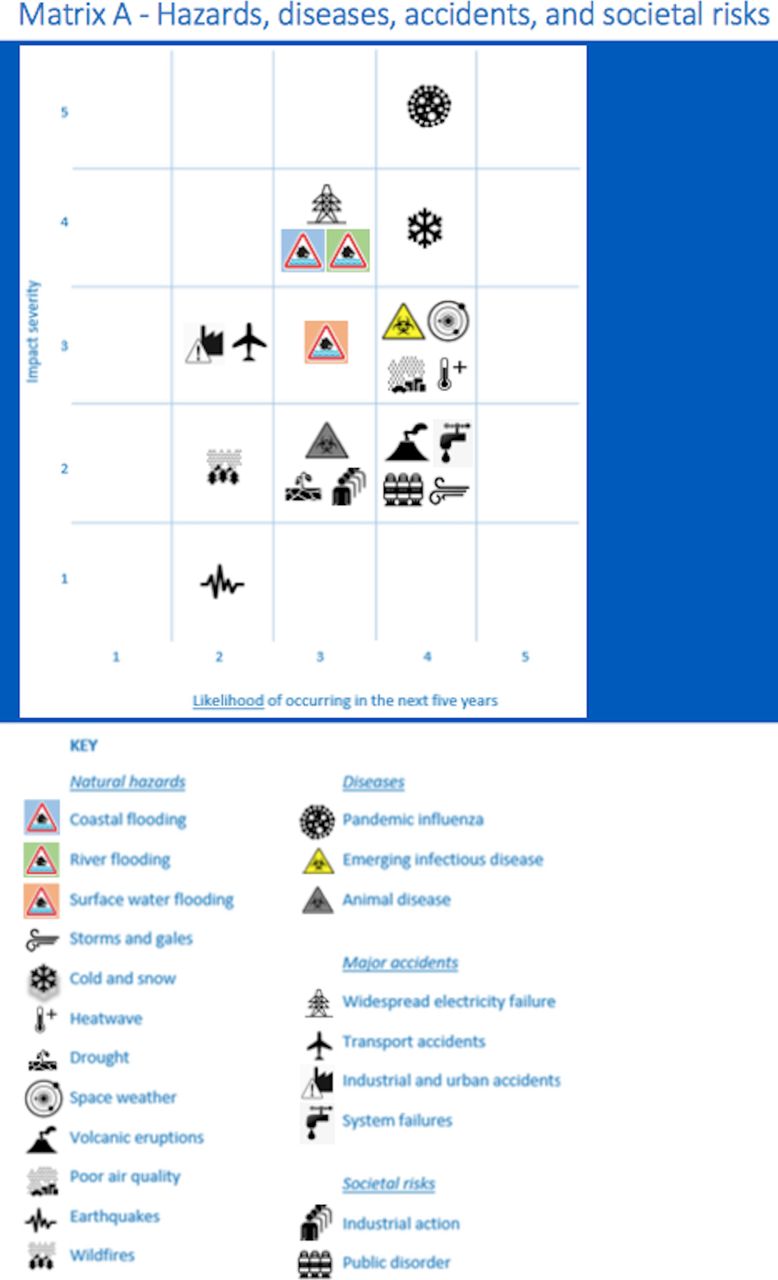
National Risk Register for hazards, diseases, accidents and societal risks.

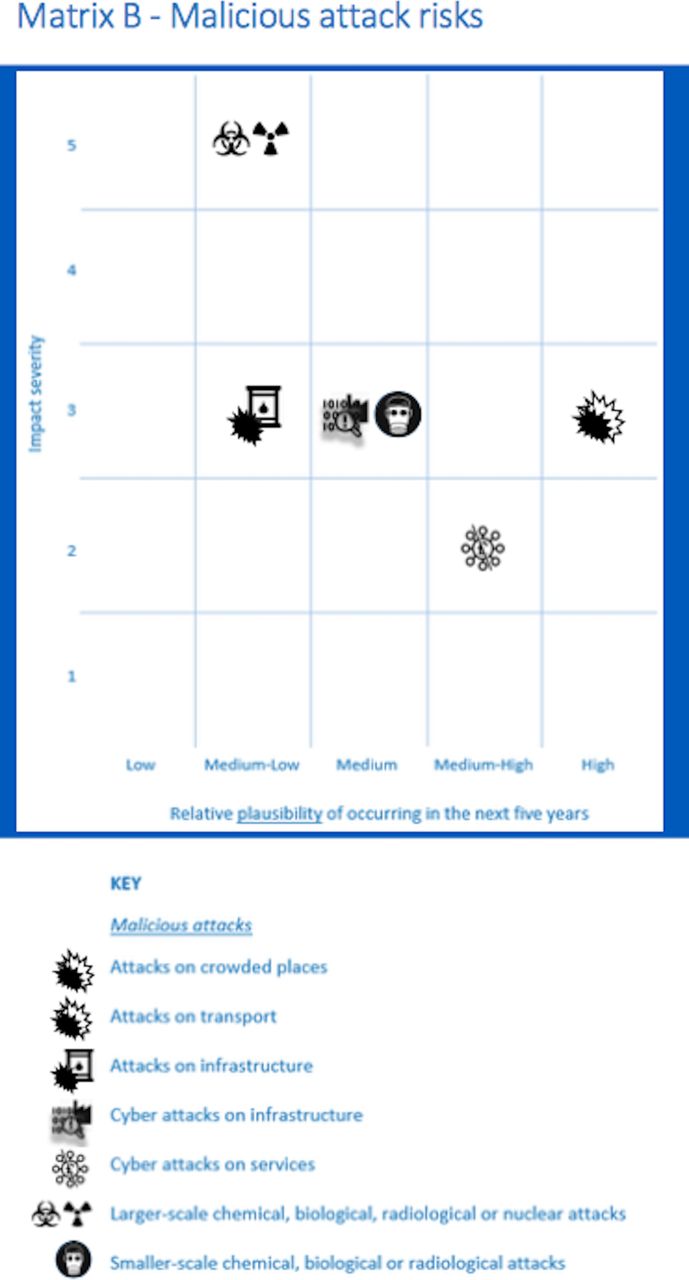
National Risk Register for malicious attacks.
{kind=link}
{kind=link}
{kind=link}
Example of a typical risk matrix.
National collaborative work across multiple organisations helps to review threats and how to subsequently address them. The recognition and understanding of these risks will influence the subsequent work which will develop national preparedness against them. Often the risk cannot be eliminated but the aim of EPRR is to take steps to ensure that these threats are known and acted on throughout the continuum of the EPRR pathway.
The inherent nature of these incidents means that the national threat profile is evolving continually both domestically and internationally. An example is the recent increase in likelihood of ‘attacks on crowded places’. The current national terrorism threat level is continually assessed by the Joint Terrorism Analysis Centre that comprises representatives from 16 government department and agencies, forming a key element of the national intelligence machinery.8 There are five levels which are designed to give an indication of the likelihood of a terrorist attack which agencies use in order to set their respective levels of readiness. The threat system is closely aligned with the US Department of Homeland Security rating system but allows domestic control and assessment according to current threats. The levels as shown in table 2 9 are often seen displayed in locations such as governmental buildings.
UK threat levels
The declared threat level depends on current available intelligence, terrorist capability, terrorist intentions and time scale, resulting in what is described as a responsive system which allows a real-time indication of the current situation.
Local, regional and national response
Health and governmental organisations have different levels of resilience which is often determined by their available resources and their experience in a given incident. To prevent becoming overwhelmed in a given situation, increasing amounts of collaboration have occurred to help improve the effectiveness of response while continuing to conduct ‘business as usual’. This expansion was arguably accelerated by the recognition of the need for Regional Networks for Major Trauma in 2010 which has seen a significant improvement in the probability of surviving major trauma.10
National Category 1 responders have revised their scope of response, depending on the type and scale of threat. Public Health England (PHE) uses separate command and control arrangements depending on the scenario and use the classification shown in table 3.
PHE scenario classification
For each type of incident, PHE now operates at one of two possible levels of response: standard or enhanced. This relates to the requirement for either local or national leadership, command and control. Irrespective of the level of incident, an Incident Director will be identified immediately the incident is declared. If there is initial uncertainty regarding this role, then the individual declaring the incident assumes the role until a suitable person is identified.11
National Health Service England (NHSE) uses the incident levels as shown in table 4, which help to indicate the degree of support required.
NHSE incident levels
Although current categories of response are different across various organisations, there has been attempts made to align the geographical boundaries for NHSE, PHE, Local Resilience Forums and Local Health Resilience Partnerships. To enhance these relationships and improve cross-agency understanding, training and exercises are conducted together wherever possible.
The importance of this collaborative work has been seen in recent events such as the Manchester Bombing and London Bridge attacks. Some of the receiving Emergency Departments had recently undergone bespoke training12 delivered by the Emergency Response Department of PHE which was reported to be useful in understanding interoperability. Regular reassessment of current threats and continued inter-organisational exercises have been recommended to enhance preparedness and future response.
Military Aid to the Civil Authorities (MACA)
During regular levels of activity, the NHS is expected to manage emergency response within its own capabilities.13 MACA is provided via a request which requires ministerial authorisation, unless there are extremely exceptional circumstances. The principles behind the request should be:
A definite need to act with the tasks for the Armed Forces made clear.
Where all other options have been discounted.
If the NHS lacks the required level of capability to fulfil the task.
The need to act is urgent and the NHS lacks available resources.
Collaboration and the pooling of expertise has been particularly applicable in assistance with blast and high-velocity injuries, as the Defence Medical Services (DMS) remains the expert cohort regarding these injuries and their treatment. This includes specialties such as anaesthetics, emergency medicine, trauma and orthopaedics, plastics and radiology. DMS specialists were able to work collaboratively and add their expertise in the aftermath of the Manchester bombing incident, working with regional specialist surgical groups in order to improve outcomes and enhance cross-organisational experience and learning.
MACA requests and action are often noteworthy and attract public attention. A joined-up communications strategy with NHSE, DH and Defence media is required and should be used to improve future collaboration and enhance organisational reputation.
Communication and information sharing
Under the Civil Contingencies Act 2004,2 responders have a duty to share information with partner organisations. This is a crucial element of civil protection work, underpinning all forms of corporation.3 However, from exercises and training through to real-life responses, interagency communication is often beseeched by problems during the period of response.
Future direction of response
The future direction of EPRR is continually evolving. It is both domestic and international with multiple potential causes for future responses. These range from terrorism to humanitarian with recent examples ranging from the Ebola response and the hurricane relief work undertaken in the Caribbean, to the terror events in Manchester and London in 2017.
Regarding Defence, the biggest change is the prioritisation of Defence Engagement, the use of military people and assets to prevent conflict, build stability and gain influence. For the first time, the key importance of this work has been noted in SDSR and is a funded, core MOD task. This demonstrates a step-change in strategy14 and helps the UK to respond to threats and crises as they emerge, strengthening soft power, building multinational relationships and contributing to future security and prosperity. This may involve initial interaction with foreign military partners but seeks to engage a broader base among civilian colleagues as initiatives develop to build capacity at the widest level.
EPRR must be able to shift from regional and national, to global action as required. A key attribute to facilitate this is to ensure that the personnel and logistic support required for a response are rapid to assemble, and flexible in scaling up and then back down. Continuing challenges remain for the longer term response and ongoing capacity building. An example of this would be improvements made in initial trauma response but uncertainty regarding longer term psycho-social support. Continued interest in this collaboration and scaling up and down of action is becoming better understood by all parties involved, with multiple civilian–military summits and exercises occurring through 2018. These events aim to include as wide a range as possible of those involved in EPRR, exercising current plans with local, regional and national partners to ensure these plans are robust, widely understood and can be performed with confidence and efficiency when they are called into action.
Review of previous isolated responses show improved outcomes with a joined-up collaborative approach. The emphasis should be on all parts of the EPRR model which will help early detection as well as more efficient response. As the broad spectrum of EPRR continues, it should be remembered that ‘intelligence is always imperfect, not everything can be stopped’,15 but marginal and continual improvements are capable of paying dividends. In health, these improvements correspond to a reduction in morbidity and mortality of our population, something that should always be the ultimate aim, regardless of specialty or organisation.
Footnotes
Contributors OQ was the sole author of this article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Commissioned; internally peer reviewed.