Article Text

Abstract
Aim Combat-related extremity injuries are regularly associated with long-term complications such as chronic infection, especially osteomyelitis. Clinical examination and laboratory parameters do not usually allow reliable diagnosis. In contrast, imaging techniques enable constructive assertions to be made about the location and extent of an infection of the peripheral musculoskeletal system. The aim of this study was therefore to determine the diagnostic reliability of three-phase bone scanning and antigranulocyte scintigraphy using Tc-99m-sulesomab (Leukoscan) in the diagnostic clarification of infections associated with combat-related extremity injuries.
Methods Twenty-seven male patients (mean age 33.9 years) with suspected combat-associated infections of the extremities were included in this retrospective analysis. All patients underwent three-phase bone scanning using Tc-99m-HDP followed by antigranulocyte scintigraphy with Tc-99m-sulesomab. In 26 of the 27 patients, a CT scan of affected limb was obtained, where the secondary fusion with single photon emission CT data set was possible. The diagnostic reliability of imaging techniques was validated against microbiological samples obtained during surgery and used as gold standard.
Results Three-phase bone scanning yielded a positive result in all patients, with 18 scans classified as true positive (TP) and nine scans as false positive (FP). This produced a sensitivity of 100%, a specificity of 0% and a positive predictive value (PPV) of 67%. Antigranulocyte scintigraphy recognised 13 patients as TP, 1 patient as FP, 8 patients as true negative (TN) and 5 patients as false negative (FN), which gave a sensitivity of 72%, a specificity of 88%, a PPV of 93%, a negative predictive value (NPV) of 62% and an accuracy of 78%. CT recognised in 7 cases a TP result, in 3 cases an FP, in 5 cases a TN and in 11 cases an FN result. This produced a sensitivity of 39%, a specificity of 63%, a PPV of 70%, an NPV of 31% and an accuracy of 46%.
Conclusions Three-phase bone scanning did not deliver any diagnostic benefit, since no result was able to differentiate unequivocally between infection-related and reactive changes. Antigranulocyte scintigraphy using Tc-99m-sulesomab represented a highly suitable technique for diagnostically clarifying combat-related infections of the extremities. It is superior to CT in sensitivity, specificity, PPV, NPV and accuracy.
- osteomyelitis
- combat-associated infection
- scintigraphy
- Tc-99m-sulesomab
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
Combat-related injuries are characterized by numerous metal splinters and bullet fragments lying superficially and deeply in the soft tissue. These injuries are commonly associated with predisposition for long-term complications such as chronic infection like osteomyelitis.
For optimal orthoplastic reconstruction of the affected limb, preoperative information of the presence and extend of an infection is essential.
Antigranulocyte scintigraphy with Tc-99m-sulesomab provides a solid basis for preoperative planning, preferably including CT as SPECT/CT.
Three-phase bone scintigraphy is not suitable for diagnosing bone and soft tissue infection in patients with combat-related injuries.
MRI, as current modality of choice, is usally contraindicated, due to scattered metal foreign bodies.
Introduction
Combat-related injuries are commonly associated with open and contaminated fractures of the extremities.1–3 They can usually only be treated definitively after a delay, sometimes not until weeks later. This results in predisposition for long-term complications such as chronic infection and abnormal wound healing.4 With post-traumatic chronic infections, the typical clinical symptoms of a florid infection often present only discreetly and sometimes not at all. Laboratory parameters also often display non-specific changes or even lie within normal limits.5 6 Reliable diagnostic investigations to confirm the presence of musculoskeletal infections are required to enable planning of treatment of these injuries. A conclusive microbiological and histological examination of tissue samples remains the diagnostic gold standard.7
However, in order to later achieve an optimal physical function with as few surgical stages as possible in the course of orthoplastic reconstruction, preoperative information about the anatomic extent of the infection is also desirable. In literature, the significance here of individual imaging techniques is still a matter of controversy.6 8–11 In many cases, reliable depiction of the state of soft tissue and bone is still possible using sectional imaging techniques as CT and MRI.6 However, patients with combat-related chronic and septic wound defects often have internal bone fixation material, which interferes with image quality due to artefact formation. Depending on their position, ferromagnetic foreign bodies spread throughout the tissue can also present a contraindication for MRI.6 9 11 In comparison, nuclear medical imaging allows the demonstration of metabolic processes and an almost artefact-free image acquisition. Diagnostic investigations generally employed are three-phase bone scanning and antigranulocyte scintigraphy.8 9 12
Previous studies have assessed the diagnostic accuracy of bone scintigraphy and scintigraphy using sulesomab, for example, for suspected joint or periprosthetic infection as well as for suspected osteomyelitis associated with diabetic foot syndrome. Antigranulocyte scintigraphy has shown good to very good diagnostic reliability.13–16 Devillers et al established a sensitivity of 86% and specificity of 72% in diagnostic investigation of bone infections in cases of diabetic foot syndrome and hip and knee joint replacements.13 Pakos et al also showed good diagnostic reliability (sensitivity=75%, specificity=86%) in the clarification of periprosthetic infections.14 Iyengar and Vinjamuri highlighted, in particular, a very good negative predictive value (NPV) of 96% for exclusion of an infection of joint implants.15 So far, there has been no evaluation of nuclear medicine analysis options conducted on a patient population with suspected combat-related extremity infection. With this in mind, the aim of the present study was to evaluate the use of scintigraphic diagnostic techniques and to compare them with the results of microbiological samples taken during surgery. We set out to answer the following questions:
Are three-phase bone scanning and antigranulocyte scintigraphy suitable as diagnostic investigations for the identification or exclusion of combat-related extremity infections?
Do three-phase bone scanning and antigranulocyte scintigraphy demonstrate greater diagnostic reliability than radiological modalities, such as CT, in the diagnostic assessment of combat-related infections?
Do three-phase bone scanning and antigranulocyte scintigraphy have major advantages or disadvantages over other diagnostic procedures, such as CT or MRI, in the diagnostic assessment of combat-related infections?
Materials and methods
Patient population and study design
During the period from April 2013 to September 2017, twenty-seven male patients (mean age 33.9 years) with combat-related extremity injuries and suspected chronic osteomyelitis were treated in an inpatient setting. The presumptive diagnosis of chronic osteomyelitis was based on clinical criteria for infection, such as absence of bony consolidation, abnormal wound healing, fistula formation, erythema, swelling and increased skin temperature of the affected extremity. The retrospective analysis involved a comparison of the results of clinical examinations, laboratory parameters (white cell count, C-reactive protein (CRP)), three-phase bone scans, antigranulocyte scintigraphy and CT, with the microbiological result representing the diagnostic gold standard.
Scintigraphy: study protocol
Before or at the beginning of their inpatient stay, each patient received a three-phase bone scan with Tc-99m-hydroxymethylene diphosphonate (HDP, Mallinckrodt Medical, Petten, the Netherlands) after application of an average activity of 545 MBq (507–608 MBq). It was carried out in accordance with current guidelines.17 18 After a period ranging from at least 48 hours up to maximum of 15 days, this was followed by antigranulocyte scintigraphy with Tc-99m-sulosomab (Leukoscan, Immunomedics, Rödermark, Germany) after an application of an average activity of 843 MBq (736–1001 MBq). Whole body scans and regional static images were obtained at different times (1–2, 4–6 and 20–24 hours) after injection (pi) of the radiopharmaceutical. Whole body scans were taken with a scan speed of 10 cm/min, 1024×1024 matrix and 1.0-fold magnification factor (zoom). A 512×512 matrix and 1.0-fold zoom were used for regional static images. Furthermore, a single photon emission CT scan (SPECT, 360°, 120 images, 20 s per image, step-and-shoot mode, 6° angle steps, 128×128 matrix, total field of view (FOV)) of the affected extremity was obtained for views 4–6 hours pi; this allows a better demarcation of hot or cold spots, which would not have been recognisable, or only poorly recognisable, using planar technique. Furthermore, SPECT scans can contribute towards more exact evaluation of location and extent.17 18 All image data were acquired using a dual-head, large FOV gamma camera (BrightView, Philips, Hamburg, Germany) with low-energy high-resolution collimators and with an energy window centred at 140 keV±5%. The patients also underwent CT of the affected extremity for morphological imaging of bony defects and secondary fusion with SPECT data sets, in order to provide anatomically more precise allocation of metabolically diagnosed foci.
Evaluation of findings
Bone scan and antigranulocyte scintigraphy were evaluated immediately after each examination on a Philips workstation (IntelliSpace Portal, V.5–7) by consensus of two examiners experienced in nuclear medicine. At the same time, a semiquantitative evaluation using region of interest (ROI) reconstruction was used in addition to visual assessment. Evaluation of CT was conducted by consensus of two radiologically experienced examiners. Local findings and reported laboratory results were known to the observers at the time of scan evaluating, while microbiological test results were not made available to them. The diagnosis of chronic osteomyelitis, soft tissue or wound infection (WI) was made by antigranulocyte scintigraphy, if a pathological increased enhancement compared with surrounding tissue and contralateral side or region of normal bone marrow (eg, iliac bone, sternum) was visible over the clinical course and if an increasing ROI ratio was evident at different examination times (4–6 hours and 20–24 hours pi). Therefore, we calculated the lesion-to-reference (L/R) ratio in early (1-2 hours pi), delayed (4–6 hours pi) and late (20–24 hours pi) images. Retrospectively, the evaluation was carried out in accordance with the relevant guideline of the European Association of Nuclear Medicine.19 Assessment of CT scans was limited due to the sometimes marked overexposure artefacts, which were present despite dual-energy technique and software-assisted postprocessing of the images. The exact specification of location and extent of infection foci was achieved using SPECT images or secondary fusion of SPECT and CT data sets.
Statistics
For the purposes of statistical analysis, sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV) and accuracy were calculated for all named examination techniques and compared with the microbiological results. There was no CT result available for one patient. McNemar’s χ2 test was used for significance analysis between the individual diagnostic investigation modalities as dichotomous samples. A comparison of their diagnostic reliability was made using cross tables based on a comparison of the positive or negative examination findings and taking microbiological results into account. A p≤0.05 was defined as significant and p≤0.01 as highly significant.
Result
Twenty-seven patients from Libya, Syria, Jordan and the Ukraine with combat-related injuries of the musculoskeletal system were treated. In 18 of the 27 (67%) patients, colonisation of the bone with pathogens was demonstrated in the microbiological examination. The diagnosis of chronic osteomyelitis was therefore established in these patients. In addition, a superficial WI was demonstrated in the group with microbiological evidence of chronic osteomyelitis in three cases and a soft tissue infection (STI) in six cases. According to microbiological resistance tests, seven patients had a multidrug-resistant Gram-negative bacteria (3MRGN) infection and four patients a 4MRGN infection according to European Committee on Antimicrobial Susceptibility Testing criteria.
Diagnostic reliability of clinical examination
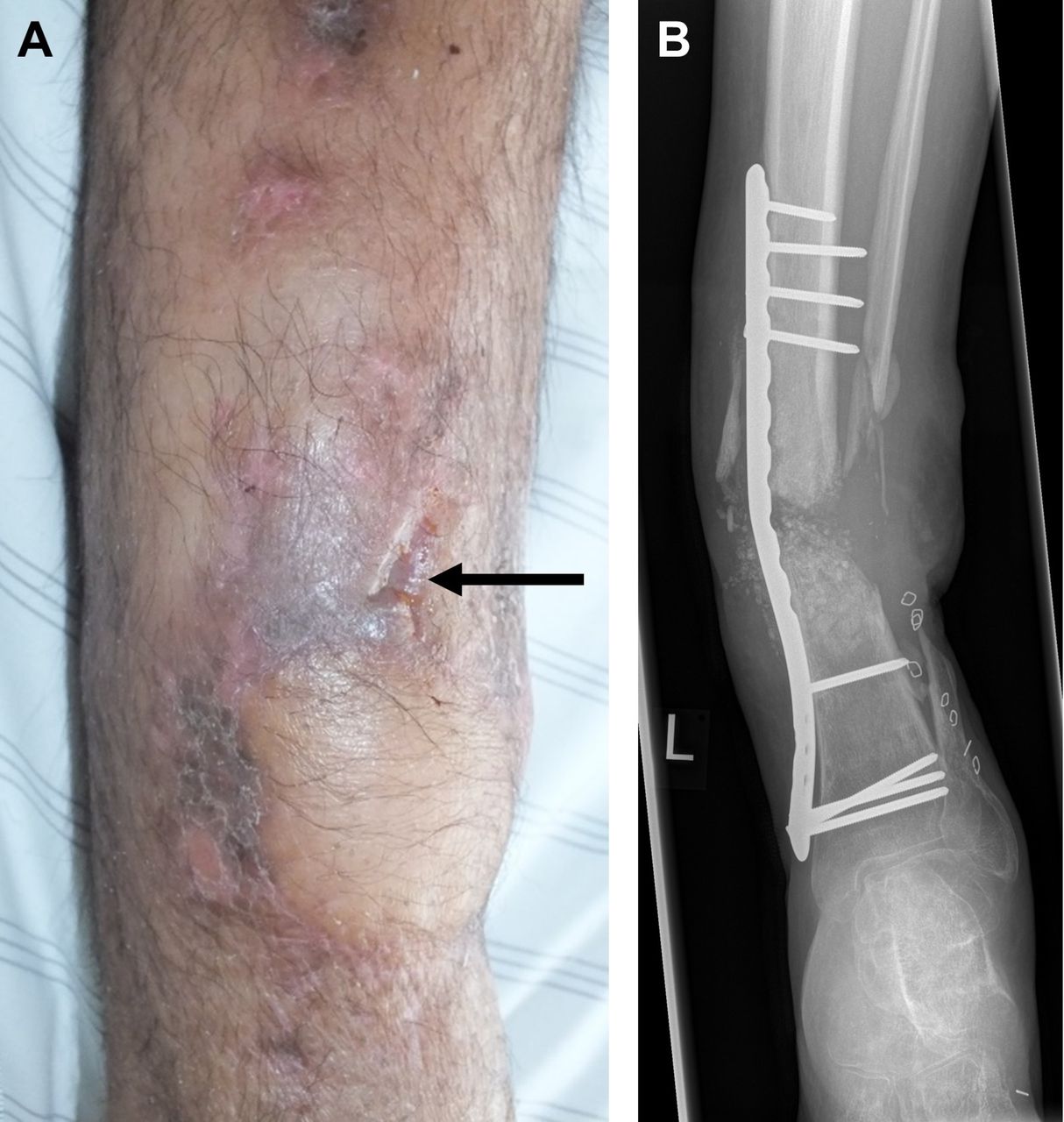
On admission to hospital, eight of the 27 patients presented clinically abnormal findings involving erythema, swelling, pain, disturbance of function (functio laesa) or fistula formation, correlating in all cases with a positive microbiological result (figure 1). In nine of 19 cases, negative examination findings corresponded with a negative microbiological result. In 10 patients, contrary to their unremarkable clinical presentation, there was microbiological evidence of pathogen colonisation of bone, resulting in a sensitivity of 44%, a specificity of 100%, a PPV of 100%, an NPV of 47% and an accuracy of 63% (tables 1 and 2).
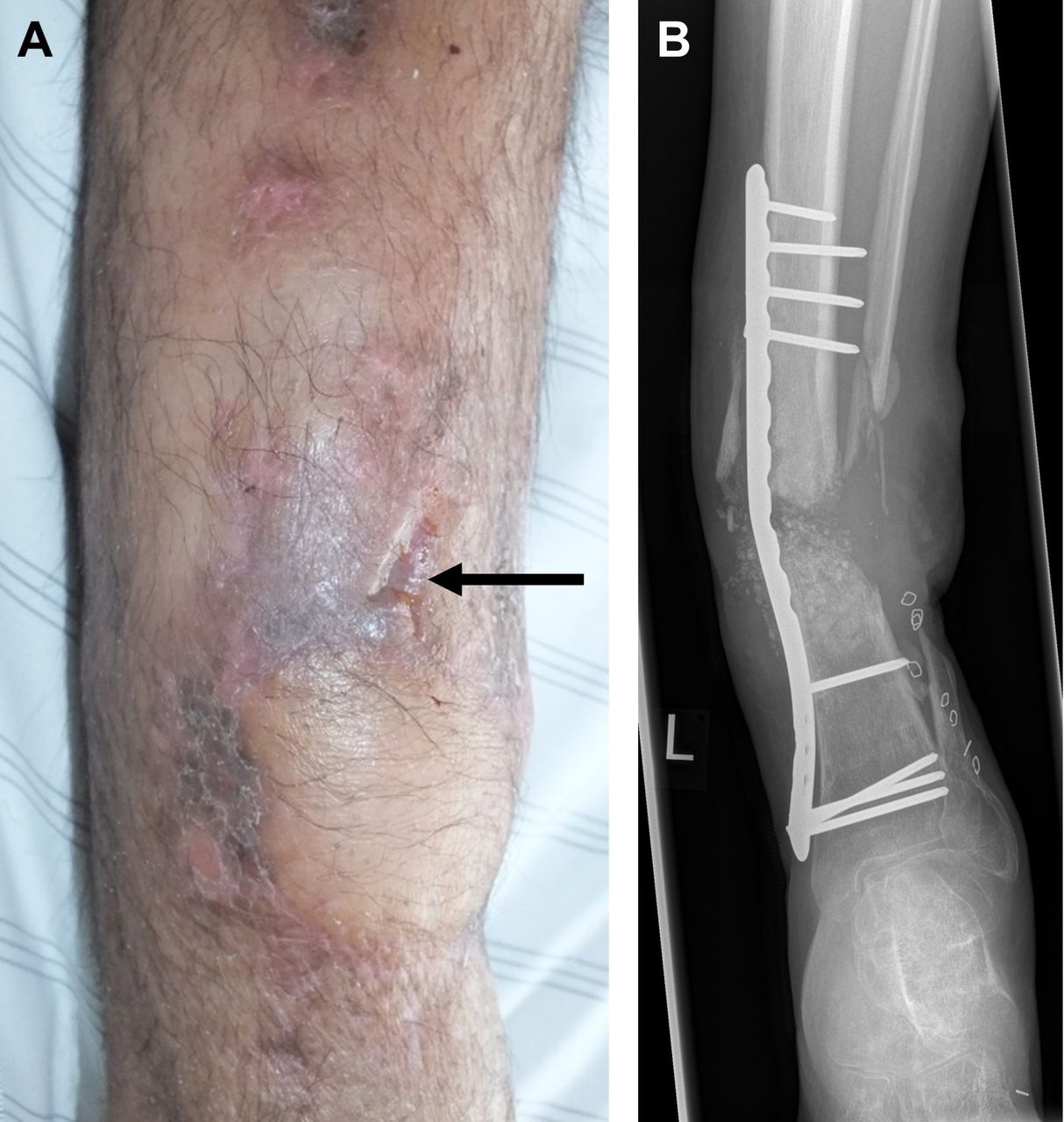
Suspected chronic osteomyelitis of the left tibia and fibula. (A) Photographic documentation of the left lower leg with clinically abnormal findings (fistula formation, see arrow). (B) Radiograph (anteroposterior, AP), plate osteosynthesis, absence of bony consolidation of the fracture associated with axial malalignment.
Overview of statistical parameters (sensitivity, specificity, positive predictive value, negative predictive value, accuracy) of the individual examination techniques; respective 95% CI in brackets
Overview of patient data
Diagnostic reliability of inflammatory laboratory parameters
Blood tests at the time of admission revealed mild leucocytosis of 9.39–10.26×109/L in seven of the 27 patients. The average white cell count of all patients was 7.72×109/L (4.52–10.26×109/L, reference range: 4.23–9.07×109/L); in the 18 patients with microbiologically confirmed osteomyelitis, the average white cell count was 7.51×109/L (4.52–9.92×109/L). Leucocytosis correlated in five cases with the microbiological result, while there was no correlation in two patients. Twenty patients had a normal white cell count. In 13 of these cases, that is, the vast majority, this did not correlate with the microbiological result; a correlation was found in only seven patients (table 2). Therefore, a sensitivity of 28%, a specificity of 78%, a PPV of 71%, an NPV of 35% and an accuracy of 44% could be calculated (table 1).
On average, a mildly elevated CRP of 17.1 mg/L (0.5–75.4 mg/L, reference range: 0–5.0 mg/L) was registered. An elevation was detected in total of 17 patients, including discrete increases to 5.7 and 6.1 mg/L, for example. This correlated in 15 cases with a microbiologically proven infection (true positive, TP); in two patients, a false positive (FP) result was demonstrated. A normal CRP was found in 10 patients. Compared with the microbiological result, a true negative (TN) result was demonstrated here in seven cases and a false negative (FN) result in three cases. The 18 patients with microbiological confirmation of osteomyelitis had a mean CRP of 22.4 mg/L (0.9–75.4 mg/L), thus resulting in a sensitivity of 83%, a specificity of 78%, a PPV of 88%, an NPV of 70% and an accuracy of 81%.
Diagnostic reliability of scintigraphy
Bone scintigraphy yielded a positive result in all 27 patients. It was not possible to make clear differentiation of findings between bone infection, post-traumatic or reactive changes, in either planar images or SPECT. Therefore, after retrospective comparison with the microbiological results, 18 scans were classified as TP and nine scans were FP (table 2). In no patient was the presence of non-viable bone suspected, since no examination phase showed areas with definable, reduced accumulation of Tc-99m-HDP.
Antigranulocyte scintigraphy produced a positive result in 14 patients (figures 2 and 3). Thirteen of these were identified as TP; scintigraphic result was FP in one patient. In comparison, a negative result was found in 13 patients, where in eight of these patients it was TN (figure 4) and in the remaining five patients FN (table 2). This resulted in a sensitivity of 72%, a specificity of 88%, a PPV of 93%, an NPV of 62% and an accuracy of 78% for antigranulocyte scintigraphy (table 1). The routinely applied SPECT scan made a significant contribution in TP cases towards achieving a correct assessment of location and extent.
In eight of the 27 patients, surgery had already been performed before scintigraphy, but this had no effect on the result of the antigranulocyte scintigraphy. In all 27 patients, the average time lag between surgery and antigranulocyte scintigraphy was 35.7 days (3–138 days). This evaluation showed that in two of the five patients with FN results on antigranulocyte scintigraphy there was a marked time lag (138 and 155 days) between diagnostic investigations and surgery. In the other three patients with FN result, there was an average difference of 4.3 days between surgery and scintigraphy.
Parenteral antibiotic therapy was given to 21 patients; it was administered to four of the patients before and during antigranulocyte scintigraphy, but this did not lead to an FP or FN result. The remaining 17 patients did not receive antibiotic medication until after antigranulocyte scintigraphy had been performed. No antibiotics were administered in six patients.

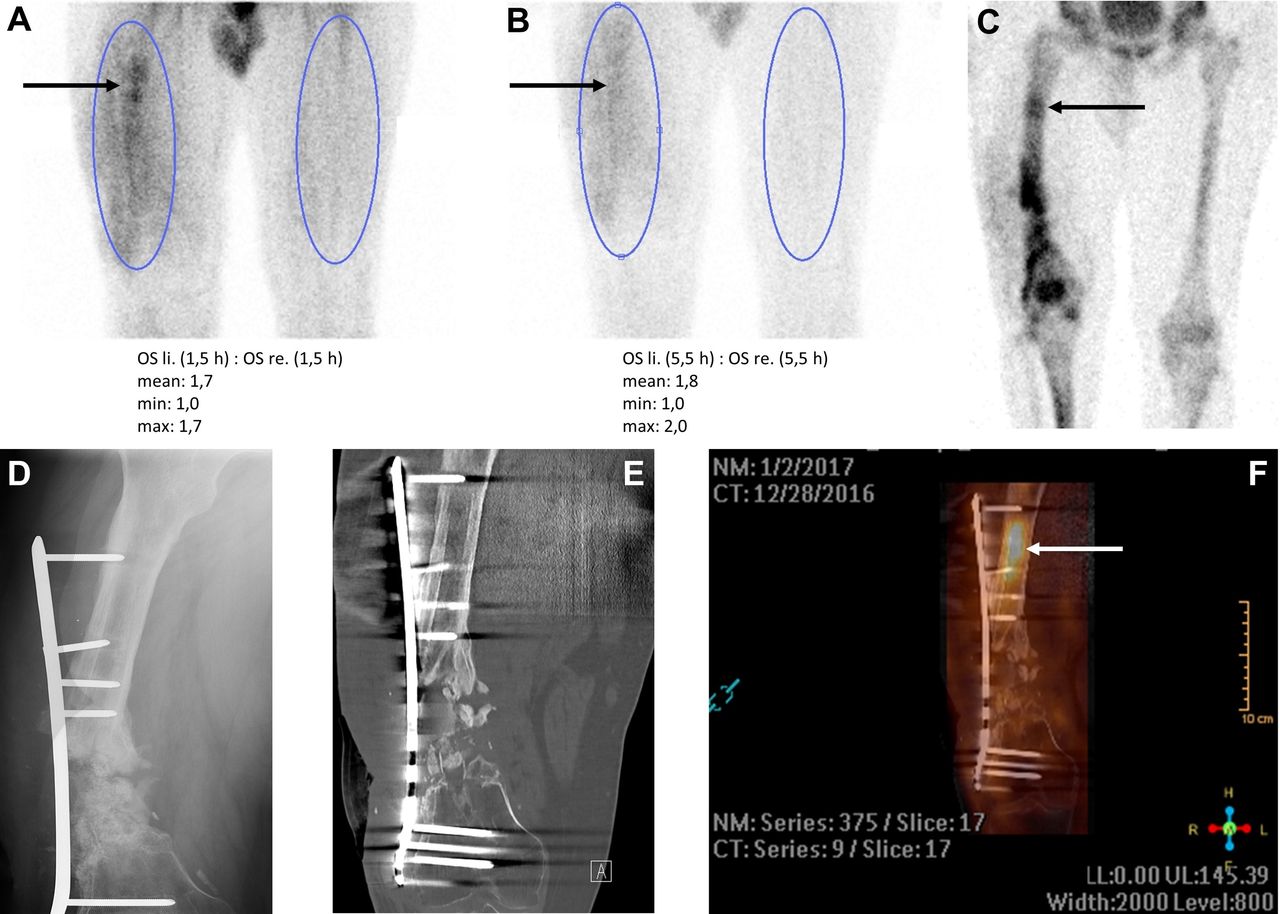
Suspected chronic osteomyelitis of the right femur. Clinical evidence of slough-covered pore measuring 1×1 cm in the distal third of right thigh, laterally; probing extended approximately 3.5 cm distally with contact down to fixation hardware. White cells=5.72×109/L, C-reactive protein (CRP)=23.4 mg/L. Intraoperative detection of Enterobacter cloacae (multidrug-resistant Gram-negative bacteria, 3MRGN). (A, B) Positive antigranulocyte scintigraphy with focus of infection in the proximal third of femur (arrow), targeted static views 1.5 hours after injection (pi) (A) and 5.5 hours pi (B) in right ventral left view (RVL), averaged region of interest (ROI) ratio increasing over the further clinical course from 1.7 to 2.0. (C) Mineralisation phase of three-phase bone scan, targeted static image 2.5 hours pi in RVL view. (D) Radiograph (anteroposterior, AP), absence of bony consolidation of the fracture, loosening of internal plate osteosynthesis. (E) Dual-energy CT, coronary section, overexposure artefacts due to bone fixation hardware and testicular capsule. (F) Secondary fusion of single photon emission CT (SPECT) antigranulocyte scintigraphy and CT, coronary section, evidence of the intramedullary focus of infection (arrow) in screw canal, proximal to non-consolidated fracture.

Suspected chronic osteomyelitis of the right tibia. Clinical evidence of myelocutaneous fistula formation in the middle third of right lower leg. White cells=7.26×109/L, C-reactive protein (CRP)=6.1 mg/L. Intraoperative isolation of Enterobacter cloacae (4MRGN) and Pseudomonas aeruginosa (multidrug-resistant Gram-negative bacteria, 4MRGN). (A, B) Positive antigranulocyte scintigraphy with focus of infection in the caudal part of fracture zone (arrow), targeted static views 2.0 hours after injection (pi) (A) and 4.5 hours pi (B) in right ventral left view (RVL), averaged region of interest (ROI) ratio increasing over the further clinical course from 1.5 to 2.2. (C, D) Multiphase bone scintigraphy, targeted static views 10 min pi (C) and 3.5 hours pi (D) in lateral-medial oblique (LMO) view. (E–H) Secondary fusion of single photon emission CT (SPECT) antigranulocyte scintigraphy and dual-energy CT in sagittal (E, F), coronary (G) sections and 3D reconstruction (H) with evidence of foci of infection in the caudoventral part of fracture zone and in the soft tissue anterior to tibial plateau (arrows); multiphase bone scan (C, D) with false-positive focus in the left anterior tibial plateau associated with adjacent soft tissue infection and periosteal reaction.

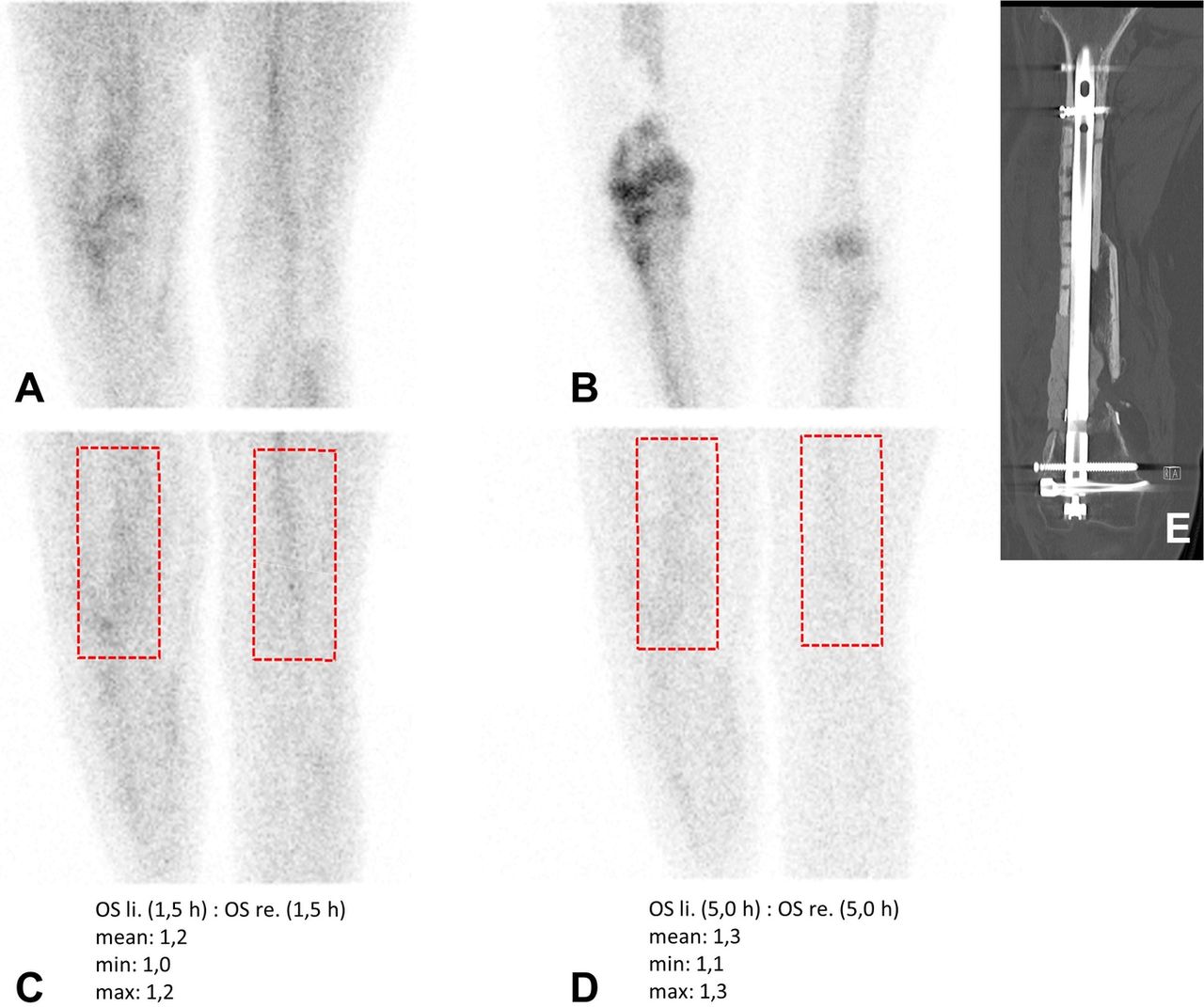
Suspected chronic osteomyelitis of the right femur secondary to a fracture from gunshot injury, intramedullary nail. No clinical evidence of an infection of the limb. White cells=10.26×109/L, C-reactive protein (CRP)=36.2 mg/L. No bacterial growth from intraoperative sample. (A, B) Multiphase nuclear bone scan, targeted static views 5 min after injection (pi) (A) and 4.5 hours pi (B). (C, D) Negative antigranulocyte scintigraphy, targeted static views 1.5 hours pi (C) and 5.0 hours pi (D) in right ventral left view (RVL), averaged region of interest (ROI) ratio constant over the further clinical course at 1.2 and 1.3. (E) Dual-energy CT in coronary cross-sectioning with locking nail.
Diagnostic reliability of CT
Ten patients demonstrated a positive result on their CT scans. This turned out to be TP in seven patients and FP in three patients. In a total of 16 patients, CT led to a negative result, which was shown to be FN in 11 patients and TN in five patients (table 2). Thus, a sensitivity of 39%, a specificity of 63%, a PPV of 70%, an NPV of 31% and an accuracy of 46% were calculated for CT (table 1).
Comparison of scintigraphy and CT
The comparison between antigranulocyte scintigraphy and bone scanning revealed highly significant difference with regard to specificity, with p value of 0.008. Comparison of sensitivity produces no significant difference, with p value of 0.06. On comparing antigranulocyte scintigraphy and CT, no clearly significant difference was found between them. As regards sensitivity, however, a trend in favour of antigranulocyte scintigraphy was evident with p value of 0.07. Before surgery, the correct diagnosis was made in patients with microbiologically confirmed bone infection in six of 18 cases (33%) using antigranulocyte scintigraphy and CT. In seven of 18 patients (39%), the bone infection could be detected using only antigranulocyte scintigraphy; CT returned negative results in these cases. In only one of 18 cases (6%) was the situation reversed, with the diagnosis being made by CT and not by antigranulocyte scintigraphy. In four of 18 patients (22%), a successful confirmation of bone infection was achieved solely with the aid of microbiological assessment, with both antigranulocyte scintigraphy and CT producing negative examination results here. On the whole, therefore, the majority of TP results could be recognised by scintigraphy using Tc-99m-sulesomab. A highly significant difference between bone scanning and CT was demonstrated regarding sensitivity, with a p value of 0.001.
Discussion
Infectious diseases of the musculoskeletal system, such as chronic osteomyelitis, often present as a heterogeneous disorder.5 6 The absence of classic signs of infection and normal inflammatory parameters in laboratory results can present even experienced clinicians with diagnostic and therapeutic challenges with regard to reaching an exact diagnosis.5 20 The aim of the present study was to review the suitability of three-phase bone scanning and antigranulocyte scintigraphy as diagnostic procedures in clarification of combat-related bone infections. It was shown that only 44% of patients with chronic osteomyelitis presented clinically suspicious examination findings. Analysis of the laboratory parameters of patient population revealed that leucocytosis was present in only 28%, while CRP was elevated in 83% of microbiological positive cases.
The imaging techniques used in nuclear medicine and radiology contrasted with these clinical methods. In our patient population, antigranulocyte scintigraphy achieved values of 72% for sensitivity and 88% for specificity. The very high PPV of 93% is particularly impressive. Evaluation of CT in comparison with antigranulocyte scintigraphy only produced a sensitivity of 39% and a specificity of 63%.
Comparison with the literature revealed similar values for the above laboratory parameters. For example, a study by Chadayammuri et al involving patients with post-traumatic osteomyelitis demonstrated a sensitivity for white cell count of about 34% and for CRP of about 82%.21 Our results for clinical parameters confirm the view held in professional literature that both unremarkable clinical examination and the absence of classic inflammatory parameters such as leucocytosis cannot exclude unequivocally the presence of chronic osteomyelitis.5 20–23 Unlike Chadayammuri et al, who calculated a specificity for CRP of only about 18%, CRP levels in our evaluation demonstrated higher specificity of 78%. In their study, Chadayammuri et al did not provide a reason for extremely low specificity for CRP. Taking into consideration our calculated accuracy of 81% for CRP, of 63% for clinical examination and of 44% for white cell count, CRP represents in this context the parameter with the greatest diagnostic benefit.
The microbiological examination of deep tissue samples still represents the gold standard for obtaining a diagnosis.5 However, before using invasive diagnostic investigations, non-invasive methods should first be employed to exclude or confirm suspected diagnosis, to carry out a pretherapeutic assessment of the extent and activity of infection and to differentiate between bone and/or STI to help in the planning of surgical management.6 12 23 24 A broad spectrum of various imaging techniques is available here, with different applications, diagnostic accuracies and disadvantages.6 24 25
In earlier assessments, MRI has developed into modality of choice, with a sensitivity up to 92%, specificity of up to 87% and the absence of any radiation exposure, provided there are no contraindications.5 25 As regards the present patient population, MRI was, however, confronted with a decisive limitation, given that ferromagnetic foreign bodies such as shrapnel and at times even bullets were present in vivo or could not be unequivocally excluded. Apart from these contraindications, adequate assessment would clearly also be rendered difficult, or even impossible, in numerous patients due to the presence of fracture fixation hardware previously introduced elsewhere in another facility. The same often applies for operations performed elsewhere shortly beforehand.8 26
Projectional radiography is regularly used as an overview examination with high spatial resolution as part of the basic diagnostic investigations.12 In several studies it was not convincing as a diagnostic procedure for detecting bone infections, with comparatively low sensitivity of 62% and 63%, respectively.27 28
The literature affords the use of nuclear medicine modalities for the diagnosis of chronic osteomyelitis varying degrees of significance. Thus, several authors recommend the use of scintigraphic imaging of bone or inflammation for cases with bone fixation hardware or unclear MRI findings.9 12 Ledermann and Kaim and Kaim et al observe that MRI is subjected to considerable limitations up to 12 months after injury or surgical intervention. In this time window, non-specific signal changes, such as those that occur in florid infection, may appear and bone marrow oedema may lead to overestimation of the extent of the infection.12 20 Kirchhoff, on the other hand, reports that the use of MRI is already possible 6 months after injury or surgery, although here too diagnostic reliability may be reduced by changes in signal intensity.9 All three publications regard complementary scintigraphic imaging of bone and inflammation as the diagnostic procedure of first choice in comparison to MRI up to 12 months after injury or surgery or following osteosynthesis.9 12 20
In those cases, three-phase bone scan is presented as the initial nuclear medical modality in the light of its sensitivity of up to 89%. The authors regard scintigraphic imaging of inflammation in this context as an additive procedure to supplement bone scintigraphy with its lower specificity of sometimes only 25%.12 25
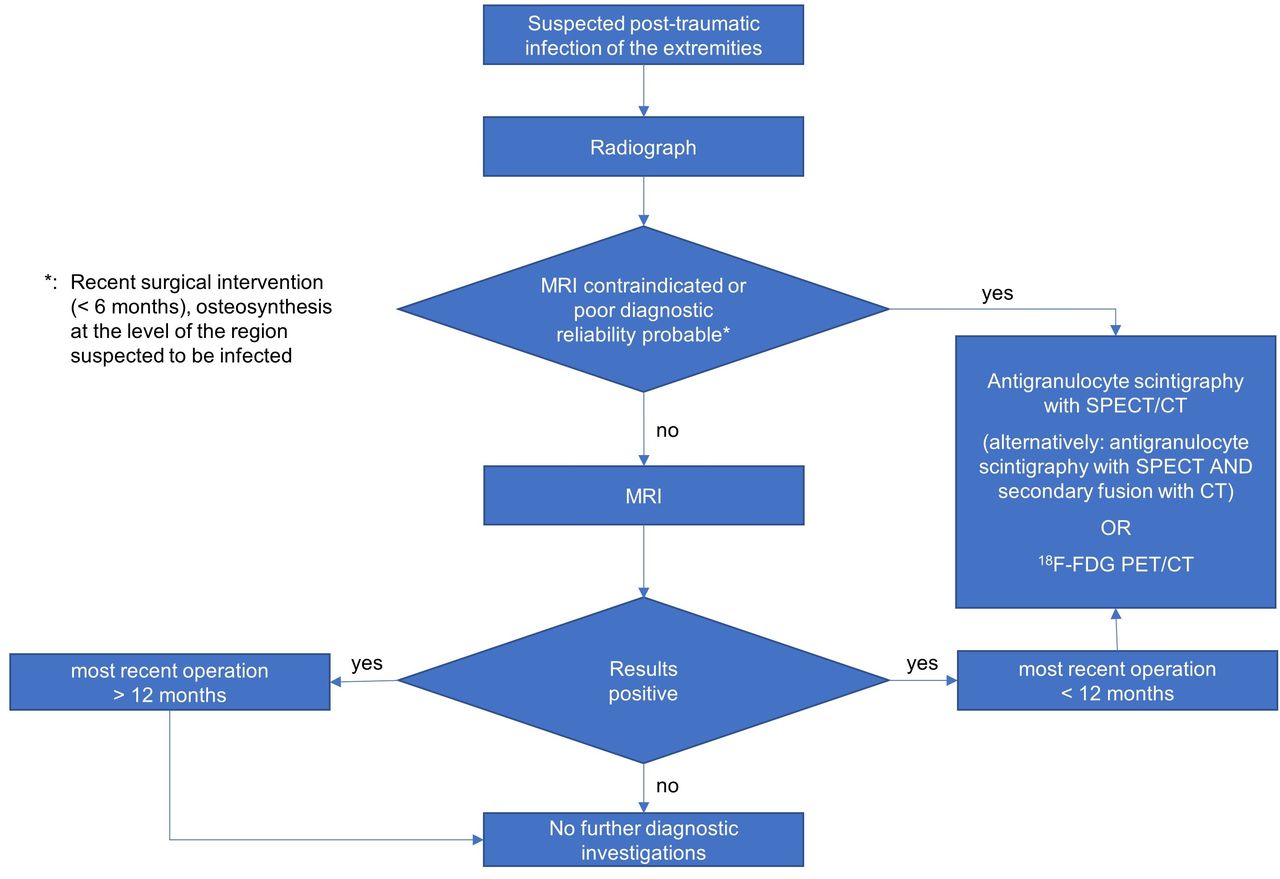
In line with publications of Ledermann and Kaim, and Kirchhoff, a modified diagnostic algorithm (figure 5) was developed for a patient population with suspected infection secondary to combat-related extremity injury.9 12

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Diagnostic algorithm for suspected infection associated with combat-related extremity injury (modified according to Kirchhoff, and Ledermann and Kaim [9 12]). 18F-FDG PET, 18-fluorodeoxyglucose positron emission tomography; MRT, MR tomography; SPECT, single photon emission CT.
Our study revealed a positive examination results in bone scanning for all patients, although it was not possible to make an unequivocal differentiation between septic or aseptic distribution pattern. Thus, bone scintigraphy proved itself, on the one hand, as the most sensitive method, but, on the other hand, produced the highest number of FP results (n=9, specificity of 0%). This high rate of FP results must be traced back to frequently observed bone healing processes, pseudarthrosis situations and sometimes loosened fixation hardware, which makes this examination modality appear impracticable, at least for this patient population.11 A further aspect of FP results can occur where STIs are immediately adjacent to bone. In these cases, bone scanning can often demonstrate bone uptake, which is not due to a focus of infection, but rather to periosteal reaction secondary to adjacent STI (figure 3). Any diagnostic approach to infections of the extremities must also adequately consider soft tissue situation. In this context, Horger et al, for example, reported that bone scintigraphy, even when using a three-phase technique, cannot be employed to distinguish between a concomitant reaction of the bone secondary to a STI and infection-related osteomyelitis.23
The only advantage of bone scintigraphy over other diagnostic methods, which were investigated, is its ability to confirm viability of the fracture ends. Nevertheless, it must be considered here that assessment of viability is usually accomplished during the surgical procedure, when the surgeon will evaluate the situation from intraoperative findings.
In principle, there is a broad spectrum of radiopharmaceuticals available for scintigraphic imaging of inflammation. The use of autologous white cells marked with In-111 or Tc-99m is still regarded as gold standard for this purpose. However, this method has been replaced by other modalities.23 29 30 Nowadays, monoclonal antibodies or fragments labelled with Tc-99m are predominantly used. In the present study, we opted for the routinely used tracer Tc-99m-sulesomab (Leukoscan), which binds to the NCA-90 surface antigen of granulocytes. This radiopharmaceutical has been extensively researched, for example, in patients with suspected periprosthetic infection and ulcers secondary to diabetic foot syndrome. Calculations showed a wide corridor of sensitivity (75%–91%) and specificity (56%–95%). Suspected periprosthetic infections were investigated by Pakos et al in a patient population with hip replacements and by Vicente et al in hip and knee replacements.14 16 31 In their studies, Pakos et al demonstrated a sensitivity of 75%, a specificity of 86% and an accuracy of 79% in a patient population of 19 patients,14 while Vicente et al identified a sensitivity of 80%, a specificity of 89% and an accuracy of 87%31 in a population of 81 patients. In comparison, our present evaluation of antigranulocyte scintigraphy produced a sensitivity of 72%, a specificity of 88% and an accuracy of 78%. The results of both authors on diagnostic clarification of periprosthetic infections correspond largely to results presented here. The calculations produced by Ivancevic et al describe a sensitivity of 100%, a specificity of 58% and an accuracy of 73% in a population of 30 patients.16 Their results are, however, comparable to only a limited degree with those presented here, as a microbiological correlation was not undertaken in all of their patients and infection prevalence was significantly lower.
Kaim et al examined a total of 18 patients with chronic, post-traumatic osteomyelitis of the lower extremities. They demonstrated a sensitivity of 77%, a specificity of 50% and an accuracy of 61%.20 They used monoclonal NCA-95 antigranulocyte antibodies (besilesomab, BW250/183). Their study showed approximately the same value for sensitivity only; specificity and accuracy have strikingly lower values. Possible reasons for this are that Kaim et al prepared scintigraphic images exclusively 17 hours pi in planar technique. SPECT images were not obtained. Given today’s diagnostic standards, obtaining SPECT scan is indispensable, since adequate assessment of the affected extremity, unobscured by overlying structures, and better spatial resolution of the foci of infection are only possible with the aid of cross-sectional imaging. This statement is further supported by addition of obtained CT data set, which allows even more precise and anatomically correct allocation of the focus with the aid of secondary fusion of SPECT and CT.
Secondary fusion of nuclear medical and radiological section image data sets is extremely time consuming and needs experience in dealing with the required software. Exact overlay can be rather difficult at times, because identical patient positioning is not always possible for the respective examinations. However, despite these disadvantages, Horger et al underlined that secondary fusion of SPECT and CT data sets is not inferior to a combined SPECT/CT examination.23 As hybrid devices become increasingly established, the ‘one-stop-shop’ approach and its associated benefits should nevertheless be given preference.
The comparison between antigranulocyte scintigraphy and CT shows a trend towards a significant difference with regard to sensitivity, with a p value of 0.07, and thus an almost better clinical value in favour of scintigraphy. Antigranulocyte scintigraphy also shows higher values for specificity, PPV and NPV than for CT, even though the latter has no significant difference from statistical point of view.
Essential weaknesses of CT include the sometimes marked overexposure artefacts from fixation hardware or metallic foreign bodies in vivo, thus not allowing adequate interpretation (figure 2). In contrast, scintigraphic diagnostic testing has almost artefact-free image acquisition. This may explain presented discrepancy of seven out of 18 microbiologically positive patients, in whom infection was recognised solely by antigranulocyte scintigraphy, while CT returned negative result.
Furthermore, antigranulocyte scintigraphy was assessed under antibiotic medication. In the present study, a total of four patients were receiving antibiotics at the time of scintigraphic diagnostic. However, in none of these patients did this result in misinterpretation of examination results. It should be noted that a TP result was detected on the antigranulocyte scintigraphy of two patients, despite, when considered retrospectively, receiving the correct antibiotics according to resistance tests. In this connection, our result contradicts the observation by Vicente et al, who ascribe some of FN results purely to the antibiotic medication and the subsequent reduction of granulocytes in focus of infection.31 It should also be noted that surgery performed in eight patients immediately before antigranulocyte scintigraphy did not negatively affect examination result. Given the last two aspects, antigranulocyte scintigraphy appears to be a robust examination modality in relation to external factors, even when statistical limitations are taken into consideration regarding number of patients.
Several authors examined the use of F-18-fluorodeoxyglucose positron emission tomography/CT (F-18-FDG-PET/CT) and were able to demonstrate promising diagnostic results (sensitivity up to 96%, specificity up to 91%). Thus, on comparison, PET/CT even ranked before MRI.7 26 27 32 Guhlmann et al were able to demonstrate, in a patient population with chronic osteomyelitis, that antigranulocyte scintigraphy and F-18-FDG-PET represent comparable methods for diagnosing infection of the peripheral skeletal system.33 In another examination, F-18-FDG-PET/CT was used by Wenter et al to examine chronic osteomyelitis and implant-associated infections in a total of 215 patients, where PET/CT was shown to have a sensitivity of 88%, a specificity of 76% and an accuracy of 82%.6 The comparison with our patient population shows almost reversed values regarding sensitivity and specificity, even though both procedures demonstrate an almost identical accuracy. Termaat et al confirmed a similar diagnostic accuracy of both methods in meta-analysis.25 To the authors’ knowledge, F-18-FDG-PET/CT has not yet been investigated on a patient population with combat-related extremity injuries. The exact significance still requires clarification in further studies.
However, this study also has its limitations. For example, the retrospective design and a comparatively small patient population restrict the scientific significance of the presented results. Furthermore, data were acquired exclusively in form of a single-centre study. Once more, the great importance of antigranulocyte scintigraphy was ascertained, in particular, because of the special patient population, in which radiological modalities have already demonstrated significant technical limitations.
Conclusions
In patients with combat-related extremity injuries, MRI, as the current modality of choice, is usually contraindicated, due to scattered metal foreign bodies or decisive limitations. The current assessment of alternative imaging modalities has shown that three-phase bone scanning is not suitable for diagnosing infection of complex, combat-related extremity injuries. This is due to the absence of differentiation between infection-related and common reactive changes of mineralisation. Furthermore, it cannot reliably assess soft tissue foci of infection. On the other hand, antigranulocyte scintigraphy using Tc-99m-sulesomab (Leukoscan) offers good diagnostic reliability in cases of chronic osteomyelitis and STIs of the extremities. The high PPV of 93% should be particularly emphasised in this context, that is, a positive result can identify post-traumatic musculoskeletal infection to a high degree of certainty. CT on its own is inferior to antigranulocyte scintigraphy with regard to sensitivity, specificity, PPV and NPV. The anatomic allocation of the foci of infection is sometimes not possible with degree of accuracy, although this disadvantage may be largely eliminated by integrating CT in form of SPECT/CT as hybrid procedure. Of all used and assessed modalities, antigranulocyte scintigraphy is the procedure with the greatest diagnostic benefit.
In clinical practice, the diagnostic algorithm for suspected combat-related extremity infection should always begin with plain radiograph as an overview study. Antigranulocyte scintigraphy and CT are recommended as supplementary procedures, at best as hybrid procedures to exploit synergistic effects of metabolic and morphological imaging. This will place preoperative planning on a firm footing. This process is summarised in a modified algorithm for diagnostic assessment (figure 5). The diagnostic value of imaging modalities assessed here should be validated using a larger patient population and in a prospective study.
Acknowledgments
We thank Dr Martin Müller, Ute Fett, Anke Bank, Kerstin Kröning, Katja Sambale and Jessica Apel for their support in examining the patients and providing examination results. We also thank Alice Schneider for monitoring the work regarding statistical questions.
References
Footnotes
Contributors All authors have contributed to transient manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval All procedures were in accordance with the ethical standards of the respective institutional research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Provenance and peer review Not commissioned; internally peer reviewed.