Article Text

Abstract
Introduction Diseases and non-battle injuries (DNBIs) are common on UK military deployments, but the collection and analysis of clinically useful data on these remain a challenge. Standard medical returns do not provide adequate clinical information, and clinician-led approaches have been laudable, but not integrated nor standardised nor used long-term. Op TRENTON is a novel UK military humanitarian operation in support of the United Nations Mission in South Sudan, which included the deployment of UK military level 1 and level 2 medical treatment facilities at Bentiu to provide healthcare for UK and United Nations (UN) personnel.
Methods A service evaluation of patient consultations and admissions at the UK military level 2 hospital was performed using two data sets collected by the emergency department (ED) and medicine (MED) teams.
Results Over a three-month (13-week) period, 286 cases were seen, of which 51% were UK troops, 29% were UN civilians and 20% were UN troops. The ED team saw 175 cases (61%) and provided definitive care for 113 (40%), whereas the MED team saw and provided definitive care for 128 cases (45%). Overall, there were 75% with diseases and 25% with non-battle injuries. The most common diagnoses seen by the ED team were musculoskeletal injuries (17%), unidentified non-malarial undifferentiated febrile illness (UNMUFI) (17%), malaria (13%), chemical pneumonitis (13%) and wounds (8%). The most common diagnoses seen by the MED team were acute gastroenteritis (AGE) (56%), UNMUFI (12%) and malaria (9%). AGE was due to viruses (31%), diarrhoeagenic Escherichia coli (32%), other bacteria (6%) and protozoa (12%).
Conclusion Data collection on DNBIs during the initial phase of this deployment was clinically useful and integrated between different departments. However, a standardised, long-term solution that is embedded into deployed healthcare is required. The clinical activity recorded here should be used for planning, training, service development and targeted research.
- disease and non-battle injuries
- acute gastroenteritis
- fever of unknown origin
- malaria
- military personnel
- south sudan
Statistics from Altmetric.com
- disease and non-battle injuries
- acute gastroenteritis
- fever of unknown origin
- malaria
- military personnel
- south sudan
Key messages
96% of clinical activity at the deployed level 2 hospital was by the emergency medicine, general medicine and primary healthcare teams.
The most common diagnoses were acute gastroenteritis, musculoskeletal injuries, unidentified non-malarial undifferentiated febrile illness, malaria and wounds.
Clinicians need to prepare for both the language and clinical challenges of seeing overseas patients who have been partially managed in other nation’s health systems.
Military emergency physicians need to be competent in managing a wide range of diseases and non-battle injuries that may be unrepresentative of their normal NHS practice.
Military general physicians need to be competent in managing a wide range of infections and other diseases that may be unrepresentative of their normal NHS practice.
Clinical experience on humanitarian missions varies significantly, and reports from clinical staff can help to prepare those about to deploy.
Introduction
Diseases and non-battle injuries (DNBIs) are the most common medical problems occurring on humanitarian deployments. The term ‘DNBI’ may be useful for commanders making casualty estimates, but diseases have little in common with non-battle injuries and so the term should not be over-used, and both require further study on deployments. The standard medical returns generated on UK military deployments for public health and command purposes (for example EpiNATO, FMed 85s and so on) do not provide sufficient clinical information to guide clinical aspects of planning, training or service development. Major trauma cases on military deployments have clinical data recorded in detail using dedicated systems and staff.1 While this enhances our understanding of one disease process (trauma), this approach is of less value for the far wider range of other diseases that occur on deployments. The need to collect clinical data on patients with diseases during deployments has become more apparent since the end of war-fighting operations, such as Op TELIC in Iraq and Op HERRICK in Afghanistan, but developing a suitable data collection system for this cohort has been challenging. Most published data on diseases occurring on UK military deployments have come from clinicians using a variety of individual approaches.2–9 These efforts have been laudable, but they have not integrated the data collection between different departments, and the approaches used have not been standardised nor used long-term. Nevertheless, valuable information has been generated in this way, which has been used for manpower planning, operational planning, mandatory training, pre-deployment training, service development and targeted research.
Op TRENTON is a novel UK military humanitarian operation in support of the United Nations Mission in South Sudan. A task force of military engineers, force protection troops and Defence Medical Services (DMS) personnel was deployed from April 2017 on a three-year mission with roulement of troops every six months (or three months for medical officers). The task force’s main objective is to provide engineering support for the United Nations (UN) Protection of Civilian (PoC) camps at Malakal and Bentiu. UK level 1 primary healthcare centres (UK L1 PHCs) are located at both sites for UK military personnel and a UK level 2 hospital (UK L2H) was located at Bentiu for ~200 UK military personnel and ~2000 UN military and civilian personnel. UN level 1 PHCs (UN L1 PHCs) are also present for each contingent of UN personnel. In comparison with recent operations in Iraq, Afghanistan and Sierra Leone, this deployment has limitations and extended timelines with regard to resupply, medical evacuation and the return of laboratory samples back to the UK.
For a three-month (13-week) period from 19 June to 24 September 2017 (during the rainy season), the UK L1 PHC and UK L2H at Bentiu were co-located at a UK medical treatment facility (MTF). The UK L2H was a ‘4-2-4-20’ facility consisting of four emergency department (ED) bays, two operating theatre tables, four intensive therapy unit (ITU) beds and 20 ward beds (including a separate isolation ward). The medical staff deployed consisted of consultants in emergency medicine (EM), general medicine, intensive care medicine, general surgery, orthopaedics, burns and plastics, radiology, anaesthetics, and aeromedical evacuation, plus a medical registrar, general practitioner and general duties medical officer. The standard UK L2H radiology service was enhanced with a CT scanner (for head scanning only), and the standard UK L2H laboratory was enhanced with the BioFire FilmArray (bioMerieux, St Louis, Missouri, USA) for multiplex PCR diagnosis of infectious diseases, as used previously.10 11
UK military patients presenting to the UK L1 PHC with acute gastroenteritis (AGE) symptoms were ‘bedded-down’ at the MTF if their symptoms were mild, there was thought to be a low-risk of transmission to other patients and there was no requirement for intravenous fluids. All patients with AGE who required L2H care were referred directly to the general medicine physician and sent directly to the isolation ward (rather than via ED) for infection prevention and control reasons.
A service evaluation of patient consultations and admissions at the UK L2H was performed in order to support improved planning, training and service development for this and other similar missions in the future.
Methods
Two data sets on the cases seen at the UK L2H were compiled and cross-referenced with each other in order to maintain consistency. Data collection was performed by the consultants in EM, general medicine and the medical registrars.
First, details of ED clinical episodes were prospectively recorded in an electronic spreadsheet listing date of attendance, national origin, ED diagnosis and disposal. ED diagnoses were sub-divided by specialty categories for analysis.
Second, all UK L2H consultations and admissions (including those ‘bedded down’ under the care of the UK L1 PHC team) were retrospectively identified from the watch-keeper’s electronic record of every patient issued with a patient tracking form (FMed 830) and from the handwritten case notes stored in the deployed L2H headquarters. Data on demographics, routes of referral and admission, dates of admission and discharge, diagnoses, and outcome were extracted and entered into an electronic spreadsheet.
For the second data set, diagnostic data were categorised into groups, diseases and further details as in previous reports.7 8 AGE was defined as having at least two of the following four features: (1) diarrhoea, (2) nausea or vomiting, (3) abdominal pain, and (4) subjective fever, headache, arthralgia or myalgia.3 Travellers’ diarrhoea (TD) was defined as having diarrhoea with no dysentery and only diarrhoeagenic Escherichia coli (enterotoxigenic, enteroaggregative, enteroinvasive or enterohaemorrhagic) found on faeces PCR testing. Acute undifferentiated febrile illness (UFI) was defined as ‘an acute (<2 week duration) febrile (>38°C) illness that had no specific organ focus on clinical and radiological assessment’.12
Results
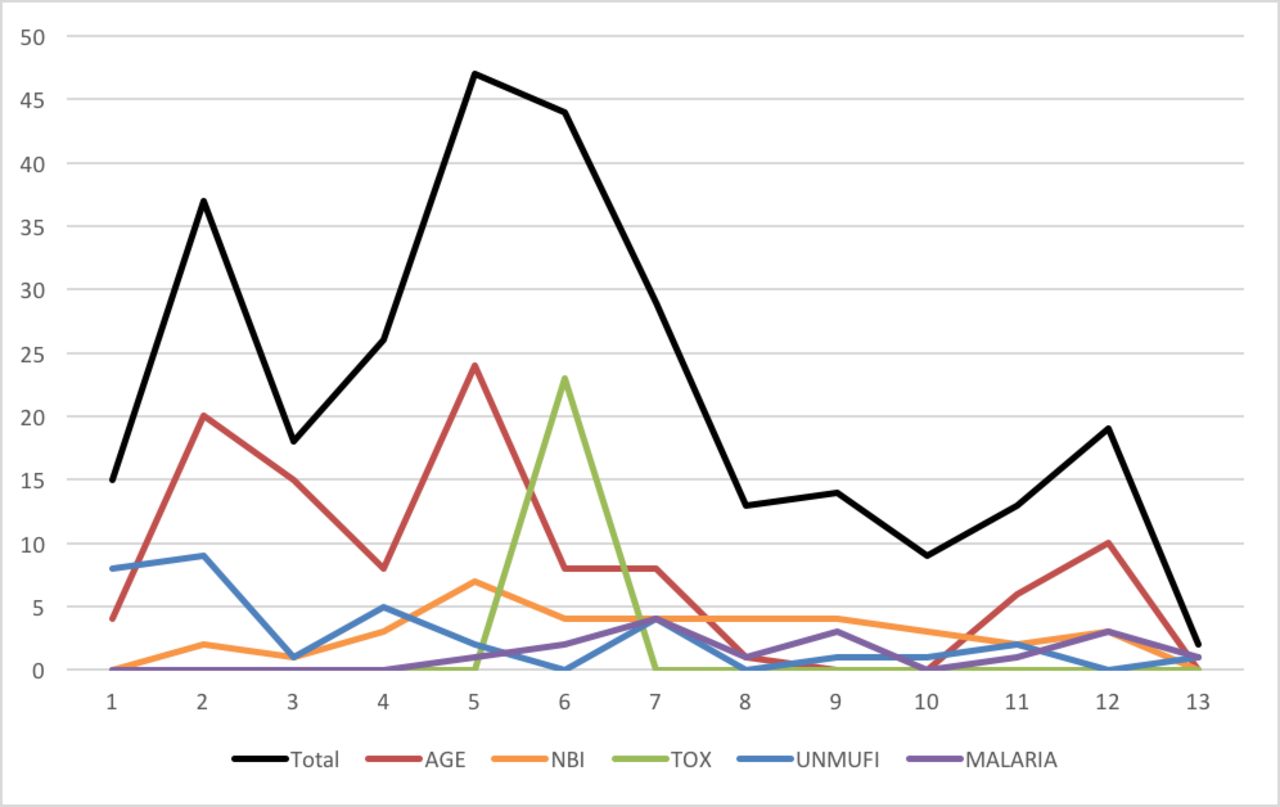
Over the first three months of Op TRENTON, there were 286 patient consultations and admissions at the UK L2H (including those ‘bedded down’ under the care of the UK L1 PHC team). The busiest month was July with 153 cases, and the number of cases varied from two to 47 per week (as shown in figure 1), with a median of 19 and a mean of 22. Of 286 patients, 146 (51%) were UK military personnel, 83 (29%) were UN civilians and 57 (20%) were UN military personnel (mostly from Ghana, Mongolia and India). There were 244 (86%) men and 42 (14%) women, and their ages varied from 19 to 56 years old, with a median of 32 years old and a mean of 33 years old.

{kind=link}
Cases seen per week at the UK level 2 hospital in Bentiu, South Sudan. AGE, acute gastroenteritis; NBI, non-battle injury; TOX, toxicology; UNMUFI, unidentified non-malarial undifferentiated febrile illness.
The ED data showed that 181 consultations were completed, including six planned reviews. Patient attendances were excluded if these were for outpatient laboratory investigations only (as sometimes requested by UN L1 PHCs). From 175 patients seen, only 34 (19%) were UK military personnel and the remaining 141 (81%) were UN civilian or military personnel. A summary of the ED clinical episodes is shown in table 1. No patients with AGE were seen in ED for infection prevention and control reasons. The most common diagnostic group was the 89 episodes (49%) that related to medical specialties, and of these the most common diagnoses were unidentified non-malarial UFI (UNMUFI) in 30 (17%) and malaria in 24 (13%). The second most common diagnostic group was non-battle injury (NBI) with 46 cases (25%), of which 31 (17%) were musculoskeletal and 15 (8%) were wounds. Toxicology problems accounted for 23 cases (13%) due to a mass presentation of chemical pneumonitis from chlorine exposure during a fire in a UN facility. ED clinical episodes were classified as ‘disease’ for 109 cases (60%) and NBI for 72 cases (40%). Only 39 (22%) of ED cases were admitted for in-patient management, and all of these were under the care of the medicine (MED) team.
Emergency department clinical episodes at the UK level 2 hospital in Bentiu, South Sudan
The data on all L2H consultations and admissions showed that of 286 cases seen, definitive care was provided by MED for 128 (45%), ED for 113 (40%), PHC for 33 (12%) and surgical specialties (SURG) for 12 (4%). Joint care between the MED and ITU teams was required for two patients (one with hypotension due to falciparum malaria and one with hypoxia due to Staphylococcal pneumonia). The diagnoses made by the MED and PHC teams are as shown in table 2. The most common diagnosis was AGE in 105 cases (37%), which was viral in 33 (31%), TD in 34 (32%), another bacterial cause in six (6%) and protozoal in 13 (12%). The second most common diagnosis made by the MED team was UNMUFI in 15 cases (12%), although a total of 36 cases were seen in conjunction with the ED team. This affected both UK and UN personnel and has not yet been diagnosed despite comprehensive serology testing of paired samples by the Rare and Imported Pathogens Laboratory (RIPL) at Public Health England (PHE) Porton, UK. Malaria accounted for 13 cases (5%), although a total of 24 malaria-related cases were seen in conjunction with the ED team. All of these were falciparum malaria and two were in UK military personnel. When all 286 cases were considered, 214 (75%) were due to disease and 72 (25%) were due to NBI.
Definitive specialty care at the UK level 2 hospital in Bentiu, South Sudan
The number of cases seen per week for the most common diagnoses and in total is shown in figure 1. From 286 cases seen, there were 142 (50%) admitted, of whom 108 (76%) were under MED, 33 (23%) were under PHC and one (1%) was under SURG. The length of stay for admissions varied from one to seven days, with a median of two days and a mean of 2.4 days. The outcomes showed that 279 (98%) of cases were returned to duty, three (1%) were evacuated to the UN level 2+ hospital in Juba, and four (1%) were evacuated to role 4 MTFs in the UK, Uganda or Kenya.
Discussion
Previous data collection on clinical activity during UK military deployments has been laudable, but not integrated nor standardised nor used long-term.2–9 This study is also not standardised nor long-term, but has integrated the data collected by the ED, MED and PHC teams (for patients ‘bedded down’ under their care). This was difficult to achieve, but produces a much more representative result. For example, ED data alone would under-represent the burden of AGE (as these cases were not admitted through ED). Similarly, MED data alone would underestimate the burden of UNMUFI and malaria that was dealt with by ED and would also under-represent AGE and skew the causes of this, if the cases managed by PHC had been excluded. In future a single joint data set should be collected by all specialties to improve the transparency of results and make analysis simpler.
An integrated, standardised and long-term system for collecting useful clinical activity data is still required if the UK Ministry of Defence (MOD) is to improve its data collection and analysis regarding injuries and illnesses on military operations.13 Attempts are now being made to develop a ‘Medical Audit Form’ system that is robust and effective while not being overcomplicated or too onerous to use (for example, if it included almost every symptom, sign, result and treatment that patients may have for a wide range of diseases). The data required by clinicians are very different from those required for public health and command purposes, and so there is little point in trying to merge these systems while the former is still being developed.
The categorisation of cases for analysis remains a contentious issue. Categories based on patient symptoms or initial diagnosis would lack diagnostic accuracy, and so categories based on clinicians’ final diagnosis are preferable. However, further categorisation of cases based on systems such as the WHO International Classification of Diseases-10 is problematic (most gastrointestinal infections are classified under ‘Certain Infectious and Parasitic Diseases’ rather than ‘Diseases of the Digestive System’, but most respiratory infections are classified under ‘Diseases of the Respiratory System’). Further categorisation according to medical specialty and sub-specialty can also be contentious, and so we have used a combination of disease and specialty categories in this paper. Obviously, standardisation of the categories used would be highly desirable in future so that data from different deployments can be compared more easily.
As expected, the majority (96%) of clinical activity recorded in this study was performed by the ED, MED and PHC teams. During Op HERRICK in Afghanistan, the ED workload was reported as 23% battle injuries, 39% NBIs and 34% disease,14 whereas on Op TRENTON it was 0% battle injuries, 40% NBIs and 60% disease during this period. With an average of two ED clinical episodes per day, the first three months of Op TRENTON has not generated a high burden of emergency patient case load. That this case load has been entirely of a DNBI nature supports the assertion that this cohort warrants more consideration. The nature and relative proportions of the DNBI cases seen can be greatly instructive when defining clinical training priorities and continued clinical exposure, as well as informing future planning assumptions.
Military EM has for more than a decade focused on a major trauma narrative for EM training and made efforts to provide additional major trauma exposure and formal teaching beyond that required of civilian EM training and the Royal College of Emergency Medicine curriculum. That Op TRENTON represents one of a series of deployments of military EM in which DNBI has predominated suggests that a rebalancing of priorities should be discussed. Emergency physicians of all grades need to be mindful of a requirement to maintain competency in a broad range of domains that include infectious diseases and tropical medicine, clinical toxicology, and musculoskeletal presentations that are now mostly managed by nurse practitioners, and the ear, nose and throat (ENT) and ophthalmology presentations for which there is little alternative deployed source of expertise and experience. Achieving this will require specific training (eg. for example, the DMS courses in infectious diseases and tropical medicine, and in chemical-biological-radiological-nuclear medicine), plus appropriate clinical training and placements for military EM trainees and consultants.
For the MED cases managed by physicians, the main diagnostic groups were gastrointestinal tract diseases, UFIs and respiratory system diseases, which was similar to previous reports.2–8 The most common diagnoses were AGE, UNMUFI, malaria and respiratory tract infections, which was also similar to previous deployments.4–8 Other significant challenges for the physicians on Op TRENTON have included cases of atrial fibrillation, deep vein thrombosis, diabetes mellitus, psychosis following high-dose mefloquine treatment for malaria in UN personnel, probable viral hepatitis in UN personnel that could not be confirmed with the available laboratory tests and possible heat illness in a British soldier. Maintaining the acute and general medicine competencies needed to deal with such a range of cases is challenging for military physicians working in NHS hospitals, where sub-specialisation and direct admissions to sub-specialties are increasingly common.
The clinical management (including isolation) of AGE cases was optimised due to the availability of faeces PCR results, and the clinicians felt that this facility should be available on all deployments of this type. In practice, many patients were found to have PCR positive results for diarrhoeagenic E. coli in addition to other enteric pathogens, and so this test may be identifying carriage or sub-clinical infection rather than clinically significant infection. Improving the effectiveness and efficiency of treatment and avoiding excessive medication and associated adverse effects should reduce the number of days lost to this very common condition and so improve operational effectiveness (especially in a small deployment where some trades were represented by a single individual).
No fever study was conducted on this deployment, and so UFI cases were investigated according to standard operating procedures only. There were 15 UK cases of UNMUFI in ~200 personnel during this three-month period, which typically presented with arthralgia, myalgia, headache, rash, leucopaenia, lymphopaenia, thrombocytopaenia and low C-reactive protein (CRP) levels. The most likely cause is an arbovirus, but none has been identified despite a full range of serology tests performed at RIPL on cases who subsequently returned to the UK. Hence a prospective fever study should be performed in future (possibly using portable real-time devices for DNA and RNA sequencing) especially in view of the problems encountered with UFI on military deployments in recent years.12
This was a high-risk deployment for malaria as South Sudan has ~3500 malaria cases per 100 000 population per year,15 and the UN PoC camp at Bentiu (which was only 400 m away) has reported 4000–8000 confirmed cases in ~150 000 people per week during the rainy season from 2015 to 2017.16 There were 13 malaria cases who were newly diagnosed and treated at the MTF during this three-month period, of whom seven required intravenous artesunate initially and the remaining six were treated with oral Riamet alone, as per UK guidelines.17 Only two cases occurred in UK military personnel and another two military cases from South Sudan presented back in the UK during this period (Mark S Bailey, unpublished data, 2018) suggesting that the bite prevention, vector control and chemoprophylaxis (mostly with Malarone) measures employed were satisfactory. In contrast, malaria prevention measures appeared to be less well implemented in UN military and civilian personnel.18
The case mix seen over this three-month period suggests that clinical pre-deployment training and force generation of clinical staff for this deployment were appropriate. However, none of the nurses had clinical experience of working on an infectious diseases ward or with patients suffering from UFIs or malaria, which was a similar issue during Op GRITROCK in Sierra Leone from 2014 to 2015 (Mark S Bailey, unpublished data, 2015). The generally low level of clinical activity seen on this deployment will inevitably lead to debate about the ideal staffing for an L2H on a humanitarian mission such as this. However, it is the UN who decides staffing requirements for UN operations 19 20 and so any significant changes would need to be negotiated with them.
The fact that 146 (~73%) of ~200 UK military personnel were seen or admitted at the MTF compared with 140 (~7%) of ~2000 UN military and civilian personnel merits consideration. The rate for UK military personnel will have been increased due to a complete roulement of these troops in August 2017 and because their proximity to the MTF increased their access to it. However, this still seems like a high DNBI casualty rate overall and reminds us that force health protection can be especially challenging in the early stages of a deployment.
The UK DMS is only occasionally involved in providing secondary healthcare for humanitarian operations, and the demands of such deployments have varied significantly for Op HAVEN21 22 in Northern Iraq in 1991, Op GABRIEL23 in Rwanda in 1997, Op GRITROCK24 25 in Sierra Leone in 2014–2015 and now Op TRENTON in South Sudan from 2017. Hence there is a need to learn as much as possible in the early stages of this deployment by prompt publication of brief reports such as this, and we encourage other healthcare disciplines to share their experiences too.
Ethics statements
Patient consent for publication
Ethics approval
This service evaluation project was approved by the deployed clinical audit committee, and all data collected were anonymised and stored securely according to the Caldicott principles.
References
Footnotes
Contributors All authors treated the patients. MSB, IG, JL, JSB and NEH collected the data. MSB and IG drafted the manuscript, which was reviewed by all authors. MSB is the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer The views expressed in this article are those of the authors and do not reflect the official policy of the Defence Medical Services, Ministry of Defence or British Government.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.