Article Text

Abstract
Introduction Fractures have been a common denominator of the injury patterns observed over the past century of warfare. The fractures typified by the blast and ballistic injuries of war lead to high rates of bone loss, soft tissue injury and infection, greatly increasing the likelihood of non-union. Despite this, no reliable treatment strategy for non-union exists. This literature review aims to explore the rates of non-union across a century of conflict, in order to determine whether our ability to heal the fractures of war has improved.
Methods A systematic review of the literature was conducted, evaluating the rates of union in fractures sustained in a combat environment over a 100-year period. Only those fractures sustained through a ballistic or blast mechanism were included. The review was in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses. Quality and bias assessment was also undertaken.
Results Thirty studies met the inclusion criteria, with a total of 3232 fractures described across 15 different conflicts from the period 1919–2019. Male subjects made up 96% of cases, and tibial fractures predominated (39%). The lowest fracture union rate observed in a series was 50%. Linear regression analysis demonstrated that increasing years had no statistically significant impact on union rate.
Conclusions Failure to improve fracture union rates is likely a result of numerous factors, including greater use of blast weaponry and better survivability of casualties. Finding novel strategies to promote fracture healing is a key defence research priority in order to improve the rates of fractures sustained in a combat environment.
- adult orthopaedics
- limb reconstruction
- trauma management
- orthopaedic & trauma surgery
Data availability statement
Data are available in a public, open access repository. All papers included in the systematic review are accessible on the world wide web.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
Fractures sustained in a combat environment are at high risk of progressing to non-union.
There does not appear to be a discernible improvement in the rates of fracture union over across a century of warfare.
Prevention and management of non-union in the fractures of military personnel remains in a key priority in defence research.
Better survivability of individuals and increasing use of blast weaponry may be key factors contributing to this apparent failure in medical advancement of this condition.
Introduction
Since World War I, war has been ubiquitous across the globe with each conflict being defined and characterised by novel weaponry and injury patterns. Extremity trauma has remained a common denominator of injuries sustained on the battlefield throughout this period. Rates of extremity injury are reported at 54%–77% among injured service personnel, with fractures being sustained in approximately one-third of these cases.1–3
Bone non-union is the failure of fracture to heal. The mechanism through which a fracture is sustained has a significant impact on the risk of developing a non-union. The high energy fractures seen with the blast and ballistic injuries commonly sustained in a combat environment lead to high rates of bone loss, soft tissue injury and infection that greatly increase the chance of a fracture progressing to non-union.4 5 Although commonly seen among military personnel, the global terrorist attacks in recent years as well as civilian injuries sustained in warfare mean that these complex injuries are not confined to servicepersons.6 7 Moreover, the risk of non-union is further compounded by the often austere environment in which such individuals (both military and civilian alike) sustain their injuries, often resulting in delayed initial management and treatment of these high-energy fractures.8 Those fractures sustained by blast and ballistic injury can therefore represent the greatest challenge to an orthopaedic surgeon when it comes to promoting bone union.
The subject of bone non-union is not a modern concept. Literature dating from 1802 details the attempted management of non-union through the use of a seton.9 Later in the 19th century, the use of irritants applied to the bone ends to stimulate callus formation was utilised. Bone grafting at the non-union site, a now commonplace method to ameliorate non-union, was first pioneered by the American orthopaedic surgeon Frederick H Albee in 1914. It formed the cornerstone of treating non-union for much of the 20th century and was later augmented by the addition of external fixation and local antibiotics for cases of infected non-union.10 More recently, the use of bone morphogenetic proteins (BMPs), stem cells, and ultrasound and shockwave therapies have increasingly been described in the literature as novel strategies to treat non-union.11–14
Despite over 200 years of non-union being described in the medical literature, the difficulties and challenges of treating this condition remain. A reproducible and reliable treatment strategy for managing non-union still eludes orthopaedic practitioners globally and besets the most experienced orthopaedic surgeon. Preclinical studies abound that seek to identify a novel method to treat it.15
This systematic review seeks to identify whether the ability of the military surgeon to achieve union in fractures sustained in the combat environment has improved over a century of conflict.
Methods
Search strategy
A systematic review of the literature was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.16 Relevant search terms were composed of those relating to fracture healing and non-union, with the preface of each search term then adding the military component of the review. An example of a search strategy is included in the online supplementary appendix. Sources of peer-reviewed information were identified using Embase, Medline and Google Scholar. Hand searching citation lists of included studies and relevant reviews was also undertaken. The search was limited to a 100-year period, that is, 1919–2019.
Supplemental material
Inclusion criteria
Fractures sustained in a combat environment or war zone.
Civilian injuries sustained in a combat environment or war zone.
Peer-reviewed articles.
Bone union rates stipulated.
Adult and paediatric fractures.
Exclusion criteria
Established non-union.
Delayed bone union.
Fractures sustained from non-ballistic/blast injuries for example, road traffic accidents and falls.
Articles not written in English.
Injuries sustained in a civilian environment.
Primary amputations.
Data extraction
Two authors undertook independent literature searches (SKS and OT), with a third author being used for arbitration (AR). The demographical data, mechanism of injury, anatomical location of the non-union, treatment modality, rates of union, average time to union, infection rates, delayed amputation rates and mortality rates were recorded from the papers. Where papers discussed both included and excluded cases, the average age and gender demographics were extracted from all cases, with subsequent data on non-union treatment and outcomes relating to only those cases meeting the inclusion criteria. This was necessary as it was not possible in most instances to delineate the age and gender demographics once cases were excluded, as many papers described the pooled age and gender demographics relating to all cases in the paper.
Quality assessment
The presence or absence of five data items pertaining to bias assessment was also extracted from included papers: demographical data; completeness of data set; blinding; definition of union or non-union specified; and treatment strategy stipulated. Due to the niche nature of the subject matter and absence of any randomised controlled trials, it was not possible to apply a validated quality assessment scoring system to the included papers.
Results
Demographic data
A total of 1377 studies were identified by the search process, with 30 papers meeting the inclusion criteria (Figure 1). The 30 studies encompassed data from 15 different conflicts and wars over the period 1919–2019. Fractures sustained from the Israel–Palestine conflict (1948-present) (n=6) and Iraq war (2003–2009) (n=5) had the highest prevalence among included papers.
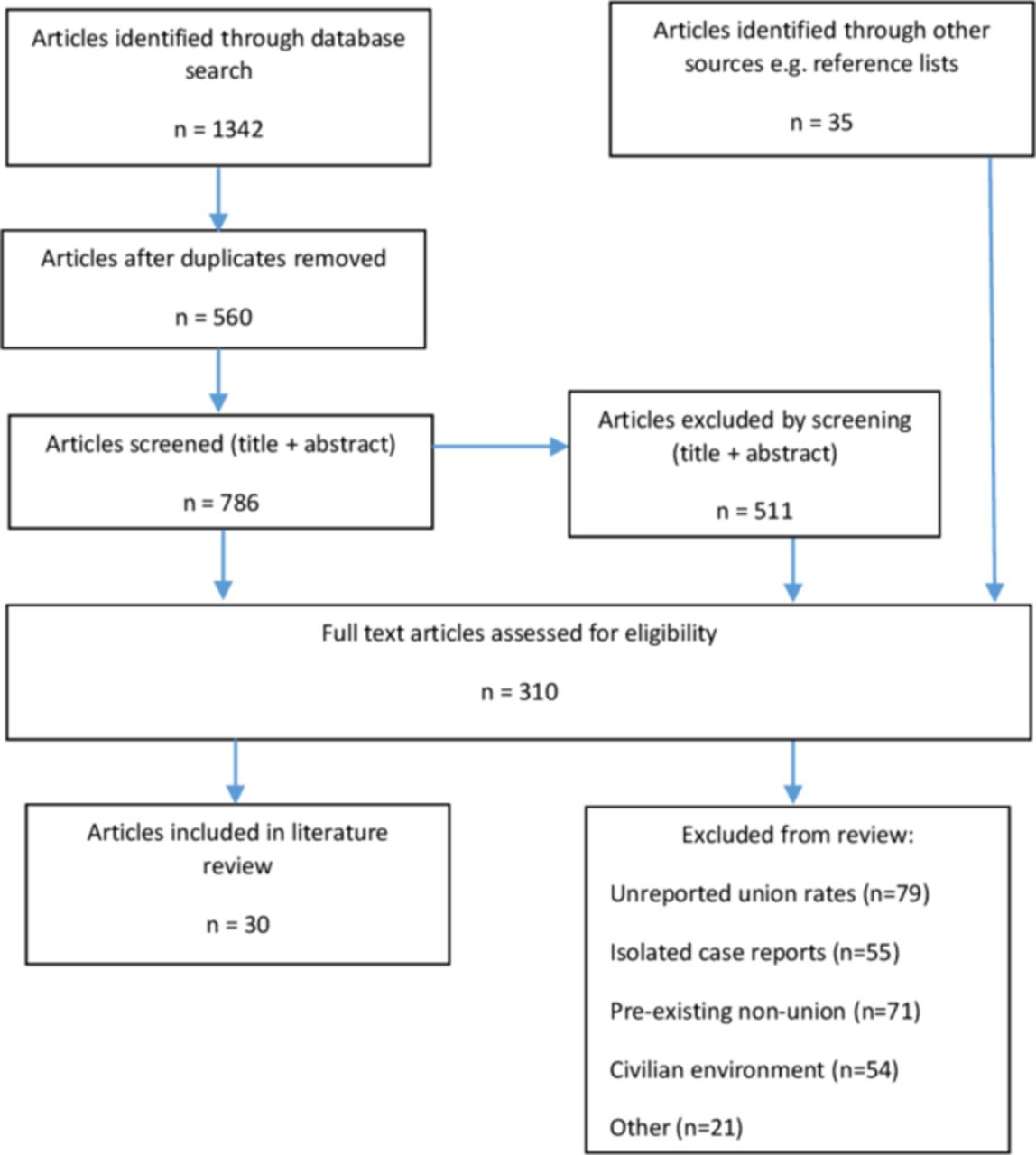
PRISMA diagram illustrating the literature search and identification process. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
The median study size was 110 (range 4–3190), and the average age of subjects was 28 years. Male patients made up 96% of the total cases (male n=1709, female n=74). The average age of the subjects was not detailed in 18/30 papers (60%), and the gender distribution of the subjects was not detailed in 13/30 papers (43.3%). A summary of the demographical data from the included studies is illustrated in Table 1.
Table illustrating fracture treatment strategies and associated union rates
Anatomical location of fractures
A total of 3232 cases of fracture were described. Tibial fractures predominated (n=1247; 39%), followed by femoral (n=956; 30%), humeral (n=563; 17%) and forearm fractures (n=366; 11%). Other anatomical locations included the clavicle, patella, scapula and fractures of the foot ankle (n=100; 3%). Three out of 30 (10%) papers did not describe the anatomical location of the fractures. The percentage of tibial fractures among all fractures analysed increased from 21% in the first three decades (1919–1949) to 43% in the last three decades (1989–2019).
Mechanism of injury
The injury mechanism was classified as ‘blast’ (relating to injuries sustained from bombs, mines and IEDs) or ‘ballistic’ (relating to injuries sustained from projectiles encompassing bullets and artillery shell, including fragmentation injuries). Injuries sustained from other causes, for example, road traffic accidents were excluded. Fractures sustained as a result of ballistic mechanisms dropped from 100% in the World War I era (1911–1920) to 30.5% in the most recent decade analysed (2011–2020), compared with blast mechanisms which rose from 0% to 69.5% across the same period (Figure 2).

Proportion of blast versus ballistic injuries for each decade of study. Omitted decades are a result of an absence of papers and/or absence of data.
Fracture treatment
The treatment strategies employed by the 30 included papers can be broadly classified in to four categories: (1) bone grafting, (2) external fixation, (3) internal fixation (including intramedullary nailing and plating) and (4) non-operative (Table 1). These treatment strategies were either used alone, or in conjunction with another treatment category, for example, internal fixation and bone grafting,17 or with an adjuvant treatment, for example, external fixation with BMPs.18 A number of papers also employed two or more different strategies in the form of a trial of fracture treatment modalities19 or because different fracture patterns warranted contrasting fixation methods.20 External fixation was the most common treatment modality (n=17), followed by non-operative management (n=9), internal fixation (n=7), bone grafting (n=6) and others (n=3), which encompassed use of BMP and minimal osteosynthesis.
Fracture union rates
Fracture union rates were defined as fractures that healed over total number of fractures sustained, after exclusion of primary amputations. Delayed amputations (due to failure of salvage procedures) and progression to non-union were considered as failure of healing. The definitions of the terms ‘union’ or ‘non-union’ were determined by the authors of the included papers (rather than the authors of this review). A definition of fracture union or non-union was stipulated in 5/30 (16.7%) of papers reviewed (Table 2). No two identical definitions existed between papers that cited a definition.
Definitions of union or non-union, where stated amongst included papers
The mean fracture union rate across all 30 papers was 87.6%. The lowest fracture union rates was 50%,21 and the highest union rates were reported at 100%, observed in 4/30 papers22–25 (Table 1). We used linear regression to test whether non-union rates have changed over time. This analysis indicated that the year of study had no statistically significant effect on non-union rate (n=30, p=0.98, r2=0.00002) (Figure 3).

Rates of fracture union by date of publication of paper. Each data point represents the average union rate reported in an included paper.
The median length of time to union following application of treatment to the fracture was 28 weeks (IQR 21.4–25.2 weeks). In half of the papers reviewed (15/30), data pertaining to the length of time to achieve fracture union was not present.
Infection, amputation and mortality rates
Data on fracture infection rates were collated from included papers. Infection rates were reported in 24/30 papers (80%). The mean fracture infection rate was 16% (range 0%–44.5%), and the rate of infection between century quartiles remained largely static at 16.6% (1919–1944) versus 18.2% (1945–1969) versus 15.6% (1970–1994) versus 15.1% (1995–2019). Causative organisms were predominantly Clostridium perfringens (referred to as ‘gas gangrene’ in early papers; n=36), Acetinobacter (n=13), Pseudomonas aeruginosa (n=8), Enterobacter (n=6) and haemolytic Streptococcus (n=6).
Delayed amputations because of failed salvage were observed in 11/30 papers (n=91). Where reasons for failed salvage were specified, the most common factors were infection (n=45), non-union (n=8), ischaemia (n=7), uncontrollable haemorrhage (n=4) and intractable pain (n=2).
Mortality among included papers was also collated. Deaths were reported among casualties in 4/30 papers (13.3%), with rates ranging from 0.9% in the Northern Ireland conflict26 to 19.8% in casualty data from World War I.27
Assessment of bias
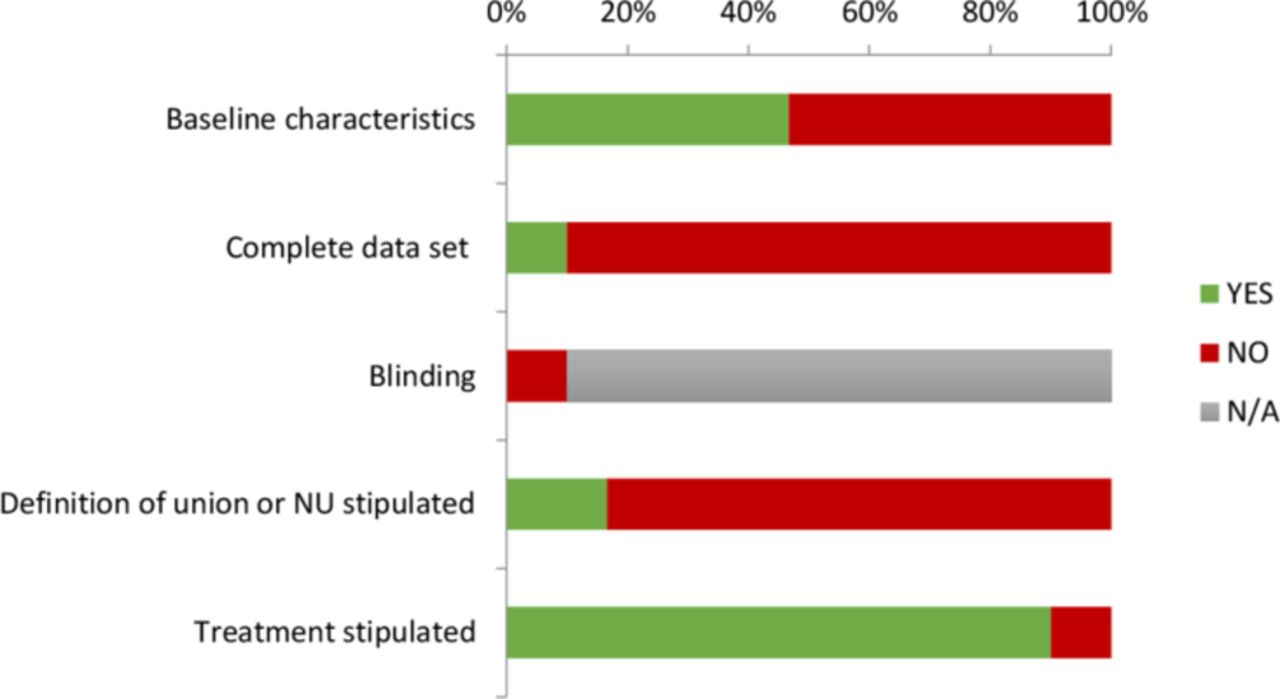
Figure 4 illustrates the results of the quality criteria items for each paper. Completeness of baseline characteristics (encompassing age and gender data) was observed in 14/30 (46.7%) of included papers, and a complete data set (encompassing demographics (age and gender data), anatomical location of fracture, treatment strategy, average time to union and infection rate and delayed amputation rates) was observed in 3/30 (10%) of papers. The definition of union or non-union was stipulated in 5/30 (16.7%) of papers, and the treatment strategy stipulated in 28/30 (93.3%) of papers. Where treatment strategies were being compared (eg, bone grafting vs bone grafting with BMP) which accounted for a total of three papers, blinding of allocation of patients to a treatment arm was not specified in any of these three papers.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Data were extracted from the included papers to assess for quality and bias, including completeness of data set (demographics, time to union, infection rates and amputation rates), stipulation of treatment, definition of union or non-union specified, blinding in the case of comparison of treatment strategies and presence of baseline characteristics (encompassing gender and age data). NU, non-union.
Discussion
Achieving successful fracture union represents one of the major challenges when managing the high-energy extremity injuries sustained in operational theatres. By reviewing a century’s worth of literature on the subject, fracture union rates appear not to have improved. This is likely to be a result of several factors.
Regarding anatomical location, fractures of the tibia have an increased propensity of progressing to non-union, both in a combat and civilian environment.28 29 The paucity of a soft tissue envelope enveloping the tibia renders it susceptible to open fractures and the subsequent difficulties in promoting union that ensues. Tibial fractures are not uncommon either, making up 39% of all fractures observed in this review. Together, it is evident that healing of the tibial fracture sustained in a combat environment will always prove challenging.
A second notable factor to consider is infection. The high energy, open fractures sustained from blast and ballistic insults predispose to contamination and the establishment of subsequent infection. Furthermore, the prolonged timelines between time of injury and index debridement surgeries that often define combat injuries contribute to the risk of subsequent infection. Infection has been shown to be a causation factor for non-union.30 31 The average fracture infection rate in this review was 16%, which is lower than other infection rates reported in the literature for comparable, combat-related injuries.4 32 However, the devastating nature of deep infection in a fracture is evident from the delayed amputation data, with infection cited as the most common cause (68%).
Finally, the mechanism of injury sustained among the fractures included in this review will predispose them to non-union. With blast and ballistic injuries comes the soft tissue damage and vascular injury that gives rise to Gustilo-Anderson type III open fractures, which have been shown to be associated positively with non-union establishment.30
There undoubtedly exist confounding factors with regards to our observation of an apparent static trend in fracture union rates across a century of literature. The incidence of tibial fractures doubled between the first three decades and the last three decades analysed from 21% to 43%. Despite the propensity of tibial fractures to progress to non-union, this was not mirrored in a concomitant increase in the rate of non-union between these same time frames suggestive of improved operative and treatment strategies.
The evolution of weaponry over the century of warfare is also likely to introduce a confounding factor in our analysis of union rates. Blast and ballistic weaponry cause injury through different mechanisms, with blast injuries arguably generating higher energy injuries through their primary, secondary, tertiary and quaternary injury effects. Given the rise in blast weaponry (largely borne out of the advent of IEDs) observed in the latter half of the century, paralleled by a drop in ballistic weaponry employed (Figure 2), one might therefore expect this to be manifested as an increase in the fracture non-union rate over this period. The fact that the non-union rate remains static is again a likely testament of improved operative techniques and better perihospital care. This may also explain the observation of apparent static infection rates of fractures over the four quartiles of the century. Increased use of blast warfare is likely leading to increased contamination and subsequent infection of fractures, with increasingly sophisticated antibiotic therapies being able to save many limbs from amputation. However, the overall effect of this on infection rate is likely to leave rates relatively unchanged.
Limitations
The heterogeneity that exists between papers, particularly regarding the definition of non-union, is a significant limiting factor for comparison between studies. Not only is there a marked paucity of a definition of union or non-union existing among the papers, a significant degree of disparity between definitions is evident. The establishment of non-union can be identified using temporal, clinical or radiological parameters, although a lack of consensus remains.33 The diagnosis of non-union can therefore be a subjective decision by the clinician.34 Consequently, union rates observed in this review are likely to be heavily biased based on the clinician’s perception and hampers reliable comparison. Marked variation in the data content of the included studies (Figure 4) also renders meaningful evaluation between papers challenging. We would advocate for the implementation of minimum datasets collected on those fractures sustained in combat environments by bodies such as the Joint Trauma Theatre Registry (JTTR) and Military Orthopaedic Trauma Registry (MOTR), in order to better unify the data and make future analysis on such fractures across campaigns and theatres easier.
Second, increasingly sophisticated medical interventions and reconstructive options has resulted in the decision to amputate versus attempt salvage of a limb to be far less binary than in previous conflicts. Although this review demonstrates that fracture union rates appear static over 100 years of conflict, one must be cognisant that the mangled extremity was far more likely to be managed with primary amputation in the former half of the century. Furthermore, the reduction in mortality rates across the included studies with time (with mortality rates decreasing from 19.8% to 2.4% between the earliest and most recent study in the review), an observation that is commensurate with other studies examining survivability35 36 ultimately means that the complexity of fractures is becoming greater as individuals are surviving greater levels of polytrauma. This paradox is likely to therefore distort further the observation of failure of improvement of fracture union rates that we have gleaned from this review.
Finally, publication bias is likely to tend towards positive results. In almost half of the papers reviewed, the rate of fracture union was greater than 90%. This is comparable with rates of healing following treatment for non-union in civilian, non-combat, low-energy fractures.37 38 Failure to stipulate a definition of union or non-union in the majority of papers also represents bias, through the authors being unable to justify their decision in determining that a non-union has been established.
Conclusion
This systematic review highlights the ongoing difficulty of managing those fractures sustained by blast and ballistic injury in a conflict environment, with evidence to suggest that union rates have failed to improve across a century of warfare. However, multiple confounders generated by inadequate data sets, the evolution of weaponry and treatment strategies and study bias render meaningful and quantitative comparison challenging. The authors would advocate that a minimum standard of data needs to be collated by the JTTR and MOTR relating to blast and ballistic-induced fractures. This would serve to minimise the heterogeneity of data obtained from such injuries and to enable easier identification of trends among such fractures when analysing outcomes. Finally, the lack of consensus within the literature regarding the definition of fracture non-union highlights the importance to authors of stipulating what is defined as non-union when publishing work on the subject.
Data availability statement
Data are available in a public, open access repository. All papers included in the systematic review are accessible on the world wide web.
Ethics statements
Patient consent for publication
Ethics approval
As this was a review of the literature and did not involve animal or human subjects, no study approval was required. Authorisation to submit for publication has been granted by the Defence Professor of Trauma and Orthopaedics (Surgeon Captain SA Stapley RN).
References
Footnotes
Contributors AR conceived the idea for the manuscript. SKS and OT undertook the literature review. SKS wrote the manuscript and performed the data analysis. SM, CH and AR reviewed the final draft of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.