Article Text

Abstract
Introduction Periodontal disease ranges from simple gums inflammation to major damage to the periodontal tissues, even losing teeth. Severe periodontitis has a world overall prevalence of 11.2%. These are evaluated with periodontal probes and oral epidemiological indices. Our aim is to estimate the prevalence and severity of periodontal disease of a Spanish military population according to the 2013 WHO criteria.
Methods Observational study of prevalence carried out in a representative random sample of 221 military staff from the Spanish Army base ‘Conde de Gazola’. Prevalence was estimated by calculating the Community Periodontal Index modified, loss of attachment, Plaque Index and Gingival Bleeding Index measured with a third-generation electronic ‘Pa-on’ periodontal probe.
Results Averages of probing depth, recession and clinical attachment level were 2.17, 0.19 and 2.36 mm. Plaque and gingival bleeding indices were 71% and 40.3%. All subjects bled in some tooth after probing. 3.6% of subjects had no periodontal pockets, 58.8% mild periodontal pockets and 37.1% severe periodontal pockets. All had some loss of attachment, 52% mild loss of attachment and 47.5% severe loss of attachment. Teeth present with and without bleeding were 24.4 (86.5%) and 3.6 (13.1%). 28% of teeth had periodontal pockets and 40.4% loss of attachment. Sextant averages with periodontal pockets and loss of attachment were 2.79 and 3.56.
Conclusions Our plaque and gingival bleeding indices were high and we found a higher prevalence and severity of periodontal disease than other Spanish and foreign military populations. This could be related to differences in context, life habits and insufficient dental hygiene.
- epidemiology
- oral medicine
- preventive medicine
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
Periodontal disease is one of the most common chronic non-communicable disease worldwide, being the main cause of tooth loss.
Any periodontal pathology in military personnel can cause a dental casualty, affecting the operation of the units.
Studies in military populations are scarce and show great variability in the prevalence and severity of periodontitis due to difficulties in comparison between authors.
The prevention of periodontal disease in Armed Forces is important to reduce oral pathologies both in national territory and in areas of operations.
Introduction
Periodontal disease is a chronic non-communicable disease defined as any disorder of the tissues that surround and support the teeth, usually involving inflammatory alterations induced by biofilm-forming bacteria in the periodontium.1 Its evaluation is performed with a periodontal probe and the prevalence in a population is determined by measuring oral hygiene, gingival and periodontal indices. Periodontitis has been reported in military populations throughout history with a variable prevalence due, among other reasons, to the absence of a uniform measurement methodology and sociodemographic differences.
During the First World War the term Trench Mouth, currently called necrotising periodontitis, was introduced because it was a common pathological periodontal condition among soldiers.2 Military professionals are a high-risk group for oral diseases because they work under specific physical, psychological and environmental conditions.3 Therefore, promoting its periodontal health is not only an important component of general health but also for military preparedness, representing a part of the strategic orientation of each country.4
The aim of this study was to estimate the prevalence and severity of periodontal disease in a representative sample of the Spanish military population according to the 2013 criteria of the WHO.
Methods
This was a cross-sectional observational prevalence study in a representative random sample of military personnel, conducted between October 2015 and May 2016, to assess periodontal health status. From the study population (N) of 1297 military personnel assigned to the ‘Conde de Gazola’ Army base (León), between 25 and 57 years of age, including all military positions from soldier to Brigadier general, a representative sample (n) of 221 individuals—189 men and 32 women—was selected using a randomisation software. This military facility houses several military units, including the Campaign Artillery Command and Emergency Intervention battalion, and its organisation is almost completely similar to other Spanish bases in terms of Army staff and structure.
The criteria established by the WHO in 2013 for the study of oral health in a population were followed, in particular the section referring to the study of periodontal status using the Community Periodontal Index modified (CPI modified)5 for measuring gingival bleeding and periodontal pockets. Loss of attachment was also evaluated. Additionally, the Plaque Index,6 the Gingival Bleeding Index,7 mean probing depth, gingival recession and clinical attachment level were examined in each individual. The third generation electronic ‘Pa-on’ periodontal probe (Orangedental GmbH & Co KG, Germany) was used as a measuring instrument as it provides greater precision and accuracy in periodontal examinations.
Examinations were performed by a single examiner, to avoid interexaminer bias, by exploring six sites per tooth of all teeth present in the mouth, including third molars. As the values calculated by the probe vary in 0.1 mm increments, the pathological cut-off determined by the WHO for probing depth and clinical attachment level was set at 3.5 mm.
Gingival bleeding was recorded as the absence or presence of bleeding on probing for each tooth. Probing depth was individually classified according to the absence or presence of mild pockets (4 to 5 mm) and severe pockets (≥6 mm), according to the highest value obtained after six periodontal probings for each tooth. Gingival health was assessed by calculating the number and percentage of individuals and teeth with and without bleeding on probing. Furthermore, the prevalence of subjects with periodontal pockets was determined by calculating the number and percentage of individuals without pockets, with superficial pockets and with deep pockets, according to the maximum severity found for each individual after examining all teeth. The severity of periodontitis was determined according to the number and percentage of teeth present in the mouth without pockets, with superficial pockets and with deep pockets. Finally, the number and percentage of excluded and missing teeth were also counted.
To compare our results with other studies we also calculated the CPI,8 recording the periodontal status by sextants. By transforming the results of the CPI modified to the CPI, in our study, we did not record the presence of calculus, and gingival bleeding was analysed separately from the presence of periodontal pockets. Therefore, individuals were classified into three categories: without periodontal pockets, with superficial pockets and with deep pockets.
Finally, to estimate cumulative periodontal destruction, the clinical attachment level was calculated by selecting index teeth and dividing the mouth into sextants for examination. The extent of loss of attachment was stratified into the following five levels according to the millimetres lost: 0 to 3 mm, 4 to 5 mm, 6 to 8 mm, 9 to 11 mm and 12 mm or more. The prevalence of loss of attachment was measured by calculating the number and percentage of individuals with the maximum value obtained in this variable after analysing the six sextants. Likewise, severity of loss of attachment was estimated according to the mean of sextants with loss of attachment. Finally, the mean of excluded and unrecorded sextants was included.
In the descriptive statistical analysis, for continuous variables, the arithmetic mean was calculated as a measure of central tendency, and the SE of the mean and SD were calculated as dispersion measures. For categorical variables, the frequency distribution was calculated according to the results of the survey variables and results obtained with the periodontal probe. For the inferential analysis, the correlation between probing depth, clinical attachment level, plaque index and the bleeding on probing index was calculated using Pearson, Kendall and Spearman correlations. Dispersion diagrams were plotted for those variables whose relationship was significant.
The results found in the present study were compared with those of similar studies at national and global levels in the military population, despite its complexity.
Results
The mean probing depth, gingival recession and clinical attachment level were 2.17 (SEM=0.02; SD=0.36), 0.19 (SEM=0.01; SD=0.21) and 2.36 (SEM=0.03; SD=0.45), respectively. The Plaque Index was 71% (SEM=0.72; SD=10.74), and the Gingival Bleeding Index was 40.3% (SEM=1.16; SD=17.14). Mean number and percentages of teeth present, missing and excluded per person were 28 (87.4%), 3.7 (11.6%), and 0.3 (1%), respectively.
Table 1 shows the CPI modified and loss of attachment results, calculated according to the highest score found after examining six sites per tooth in all teeth present in the mouth.
Periodontal status according to the highest score found after examining all sites of all teeth
All subjects studied showed bleeding on probing in some tooth and 24% in all teeth. The number and percentage of teeth present with gingival bleeding were 24.4 (86.5%). Overall, 95.9% and 99.5% of the population studied had some periodontal pocket and loss of attachment, respectively.
Severity of periodontitis according to the percentage of teeth present with periodontal pockets and loss of attachment showed that 28% and 40.3% had periodontal pockets and some degree of loss of attachment, respectively. Furthermore, the number of sextants with periodontal pockets and loss of attachment resulted in a mean of 2.79 and 3.56 sextants, respectively. The mean of excluded sextants was 0.08, and there were no unrecorded sextants.
Otherwise, according to the CPI and the highest score obtained after exploring the six sextants in each individual, the prevalence of subjects with periodontal pockets was 91% (mild: 63.8% and severe: 27.2%) while 97.2% showed some degree of loss of attachment, (4 to 5 mm: 62.4% and ≥6 mm: 34.8%).
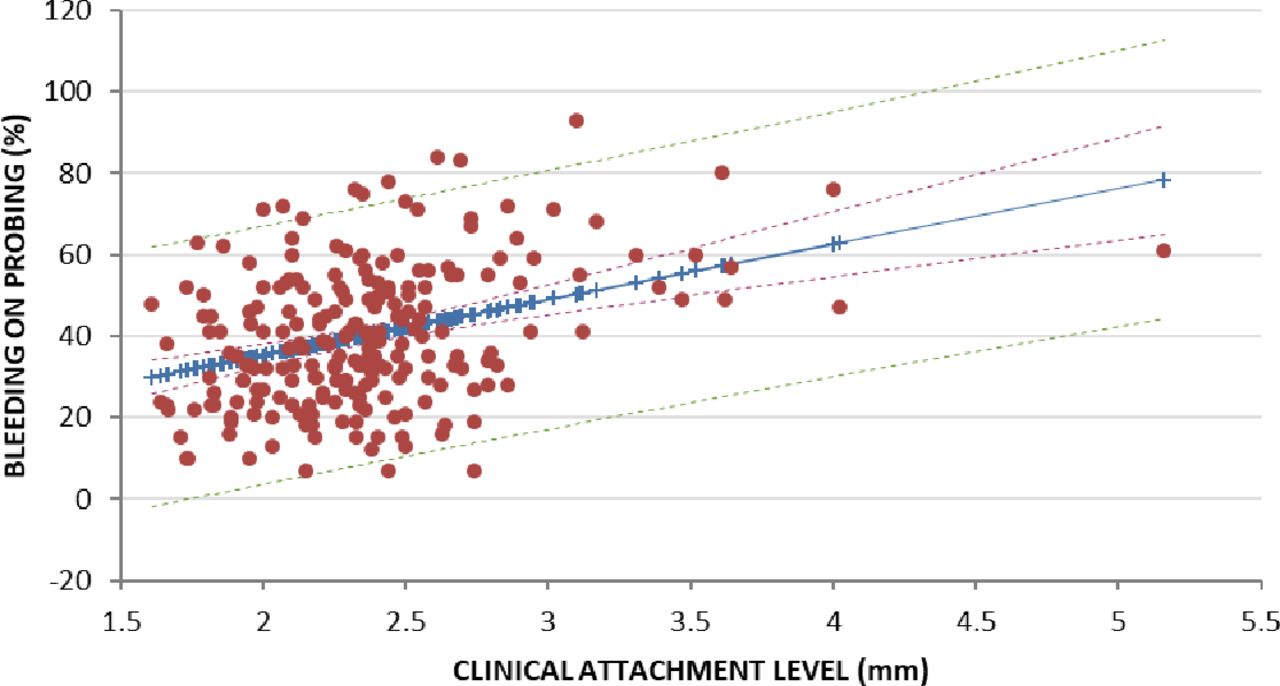
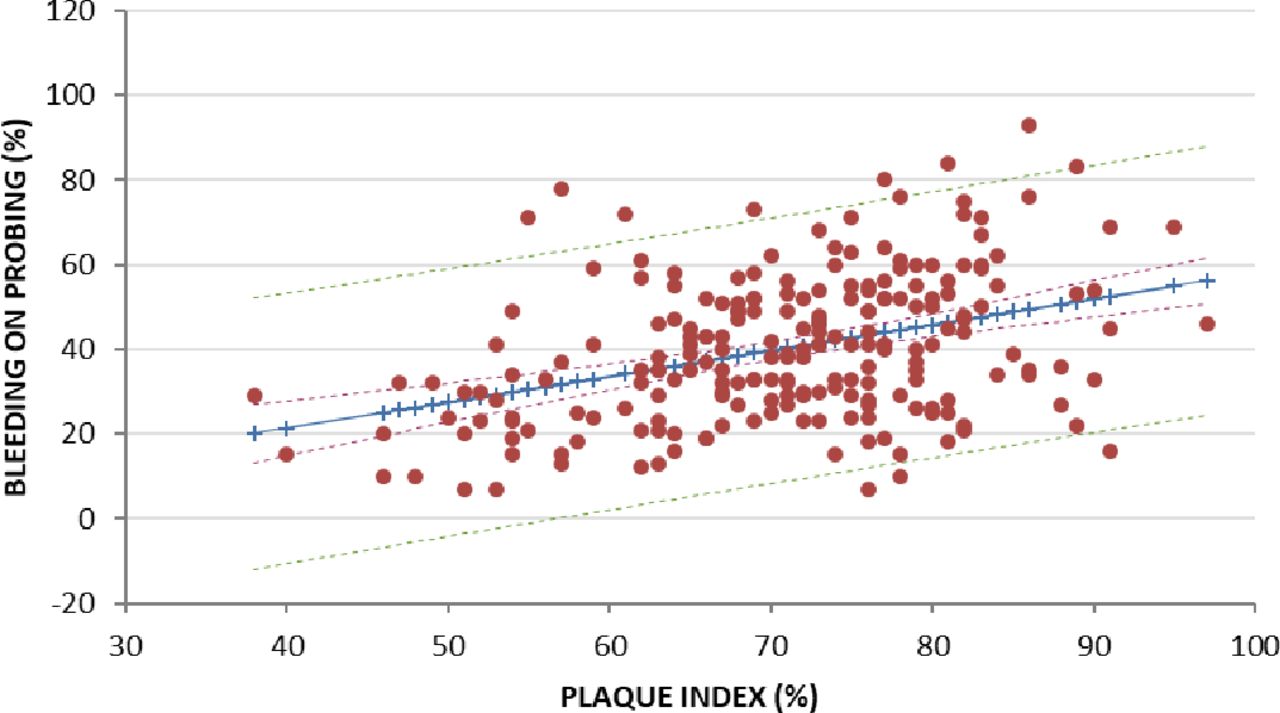
Figures 1–3 show the results of the correlation analysis between Plaque Index and bleeding on probing, probing depth and bleeding on probing and clinical attachment level and bleeding on probing. There was a significant correlation for the three cases (R=0.383; p=0.000), (R=0.453; p=0.000), (R=0.361; p=0.000), respectively; in the non-parametric analysis, the correlation was also significant (Kendall’s tau=0.258; p=0.000) (Spearman’s rho=0.355; p=0.000); (Kendall’s tau=0.282; p=0.000) (Spearman’s rho=0.407; p=0.000) and (Kendall tau=0.216; p=0.000) (Spearman’s rho=0.312; p=0.000), respectively.

Dispersion diagram for plaque index and bleeding on probing. R=0.383 (p=0.000). R=Pearson correlation coefficient.

Dispersion diagram for probing depth and bleeding on probing. R=0.453 (p=0.000). R=Pearson correlation coefficient.
{kind=link}
{kind=link}
{kind=link}
Dispersion diagram for clinical attachment level and bleeding on probing. R=0361 (p=0000). R=Pearson correlation coefficient.
Discussion
The studies on periodontal health in Spanish military populations are scarce, conducted in military conscripts,9–12 without women and with a lower mean age than military professionals.13–15 In our study the prevalence of subjects with mild pockets was between 2.6 and 24.5 times higher, and the prevalence of subjects with severe pockets was between 2.5 and 27.2 times larger. The prevalence of loss of attachment was between 1.8 and 50.9 times higher in our study. Our severity, as the mean of sextants with superficial pockets, ranged from 4.9 to 10.8 times higher. However, deep pockets ranged from 8.3 times lower to 140 times higher.
Machuca et al 11 obtained a mean probing depth 1.3 times less for each measure compared with the results from our study and Carroquino et al 9 found gingivitis 2.5 times higher than that in our study. The highest values were found in the first upper molar and the lowest in the lower incisors. However, in our study, the teeth with the highest prevalence of gingivitis were the second upper molar and the second lower premolar, and those with the lowest prevalence were the upper incisors. In their study, periodontal pockets >3 mm were rare. This differs from our results, obtaining a mean of 7.9 pockets ≥3.5 mm per person. Mombiedro-Sandoval13 found that the first and third sextants had the highest prevalence with periodontal pockets while in our study was the first.
We have chosen studies to analyse the periodontal health of foreign soldiers with an age cohort similar to ours. The prevalence of subjects with mild pockets was between 1.3 and 8.7 times higher in our study but with severe pockets ranged from 1.2 to 13 times larger. Regarding the mean of sextants per person, our mild periodontal pockets varied from 1.1 to 3.4 times higher, and severe pockets ranged from 6.9 times lower to 2.2 times higher.4 16–18In military personnel of the Indian Air Force,19 they had a similar loss of attachment of 0 to 2 mm compared with our population, 1.4 times lower in those with 3 to 4 mm and 15.8 times higher in those with ≥5 mm.
Other studies evaluated periodontal health in foreign military personnel with a young mean age (≤37 years). The presence of mild pockets in our study ranged from 1.8 to 159.5 times larger, and severe pockets ranged from 1.2 times lower to 27.2 times higher. Only the Otero study measured clinical attachment level, finding that the subjects had 4.3 times lower of loss of attachment.20 Mean of sextants per person varied in mild periodontal pockets from 1.1 to 2.37 times lower compared with our population, and severe pockets ranged from 0.42 lower to 4.5 times higher.20–24 The study conducted by Röthlisberger et al 25 in Swiss recruits found that the Gingival Bleeding Index was 1.5 times lower than that found in our study. In addition, the mean probing depth was almost identical to ours.
Finally, we recognise that there were limitations to our study. Establishing the pathological cut-off at 3.5 mm in the measurements and the inclusion of the third molars has influenced a greater periodontal condition, so our findings should be interpreted with appropriate caution. Future research would be advisable to study the impact of periodontal health promotion programme in Spanish Army.
Conclusions
The prevalence of individuals with periodontal pockets and loss of attachment based on the 2013 WHO CPI modified, as well as the severity of periodontitis, the O'Leary Plaque Index, and the Ainamo and Bay Gingival Bleeding Index were high in our military population. Periodontal disease compared with other studies in Spanish and foreign military populations was higher. However, differences in sociodemographic conditions and method comparison between authors require precaution when interpreting these findings.
This study was the first in Spain to explore periodontal health specifically in a representative sample of military professionals. The results obtained suggest inadequate oral hygiene and advise the need to improve periodontal health to reduce oral pathologies in military population both in national territory and areas of operations.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The study was authorised by the Spanish Army and each participant signed and accepted a participant form prior to be involved.
Footnotes
Contributors MBG, JMCP and PIAG contributed equally to the design, implementation of the research, analysis of results and writing of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.