Article Text

Abstract
The inclusion of British Service Personnel (SP) lacking capacity into research studies from the point of injury through to medium-term rehabilitation had not previously been undertaken until work to support operations in Afghanistan (2001–2014). The Surgeon General’s Casualty Nutrition Study and the Steroids and Immunity from Injury through to Rehabilitation Study sought to address the nutrition, endocrine and immune responses in a military patient cohort. A fundamental part of research is to feedback to patients, their relatives and ward staff on data collection and outcomes, and how future research may be improved to better support both injured SP and trauma patients in the UK. This paper will provide an experiential view on the delivery, operations and infrastructure requirements that should be considered when developing military research at a role-3 facility, before, during and after a study.
- statistics & research methods
- information management
- health services administration & management
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
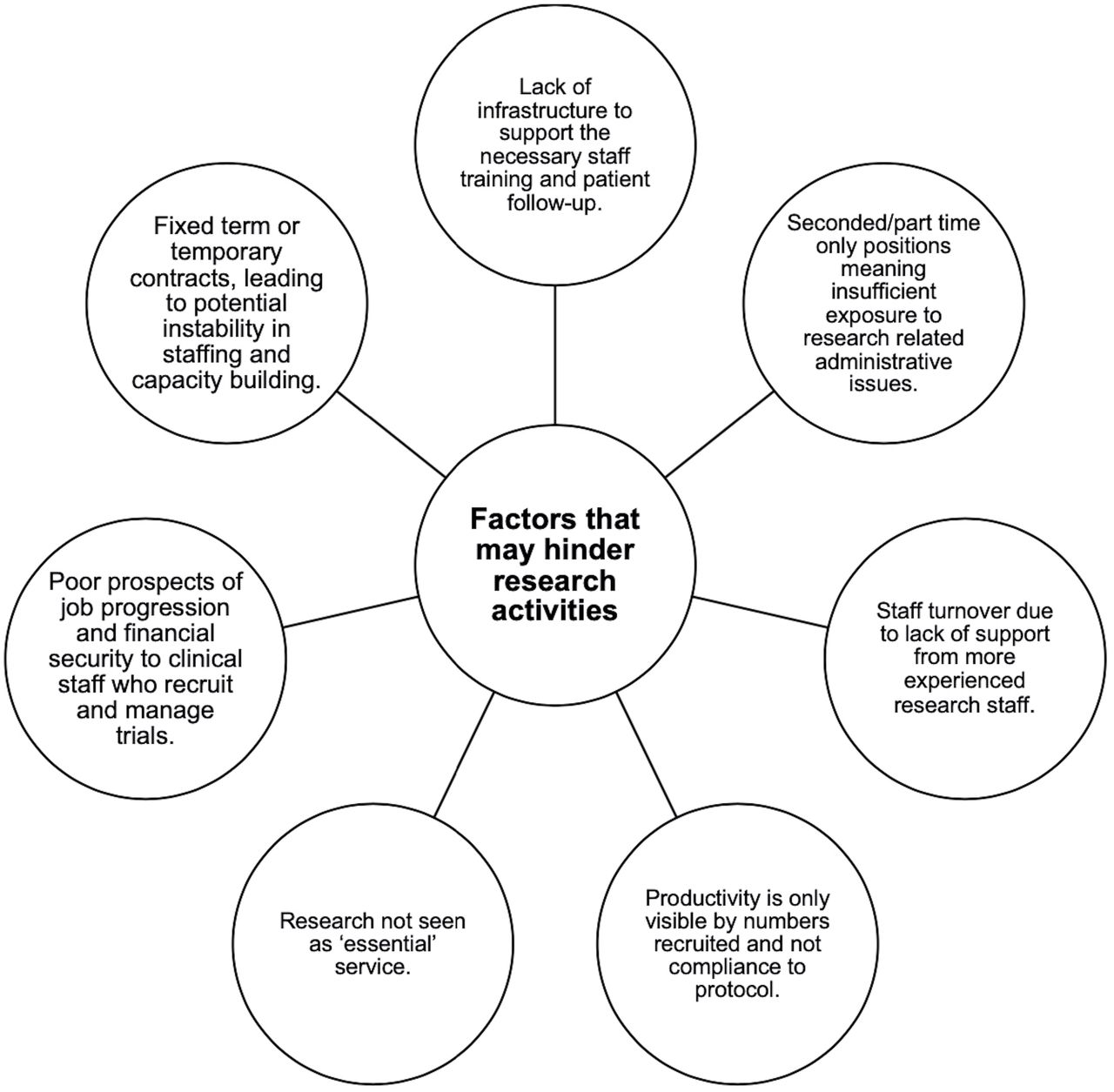
It is well established that conflict and military operations have driven medical and surgical advances throughout history,1 and there is a continued requirement to improve the evidence base of trauma care, both in military and civilian contexts. The Surgeon General’s Casualty Nutrition Study (SGCNS) and the Steroids and Immunity from Injury through to Rehabilitation Study (SIRS)2 sought to investigate the nutritional, endocrine and immune responses of a cohort of repatriated military patients. The rationale for NHS trusts to perform research is clear,3 but the ability for clinical teams to engage in research is less evident (Figure 1). The increasing media exposure, public engagement events and medical advances from well-designed clinical trials mean that patients are now more likely than ever to want to participate in research activities,4 and this should be an option open to all patients. Injured operational Service personnel (SP) are a unique cohort of patients, but nevertheless represent a cohort that should still be involved in research activity. Outputs from such research would benefit both fellow SP who may similarly experience combat trauma, and the future care of civilian patients.

Factors that may hinder research activities.
Study population
Formal research in SP without capacity had not previously been undertaken by the UK Ministry of Defence (MOD). There is an ethical and legal obligation to gain valid informed consent from any potential research participant before they undertake research activity. Consent is normally straightforward to confirm when an individual has the capacity to provide consent. However, many SP recruited into SGCNS and SIRS were unconscious when the initial blood samples needed to be drawn. The flight time to repatriate SP wounded in action during military operations in Afghanistan allowed sufficient time for next of kin relatives based in the UK to be present at Queen Elizabeth Hospital Birmingham (QEHB) on the arrival of their loved one. The study team, therefore, approached a nominated consultee, or a personal consultee, to enrol SP into the study.5
Medical and nursing staff were reticent to allow research staff to speak with relatives perceiving that ‘…they were too upset’ or ‘…unable to take in the details of the study’. The experiences of the SGCNS and SIRS study team were contrary to this perception; relatives viewed the study as a positive outcome, contrasting with the often negative prognosis of their loved one.
Upon regaining consciousness, the injured SP were generally supportive of the work that was being carried out and positive about their inclusion which had been initiated before they had the capacity to consent. Patients felt it was ‘…part of the job of being a soldier’ to be involved in such research. There was a strong sense of ‘…giving something back’ to their fellow soldiers and an acknowledgement of the care they had received during their inpatient stay.
Some SP had taken part in MOD research before, and as such were confident in their decision to join the study; they did not want a lengthy consultation process with the study team. Personal consultees commented that their relatives were proud to have altruistic motives for their involvement in the study. Indeed, evidence suggests that those who provided altruistic motivation for participation in research were more likely to have higher levels of social support.6 .
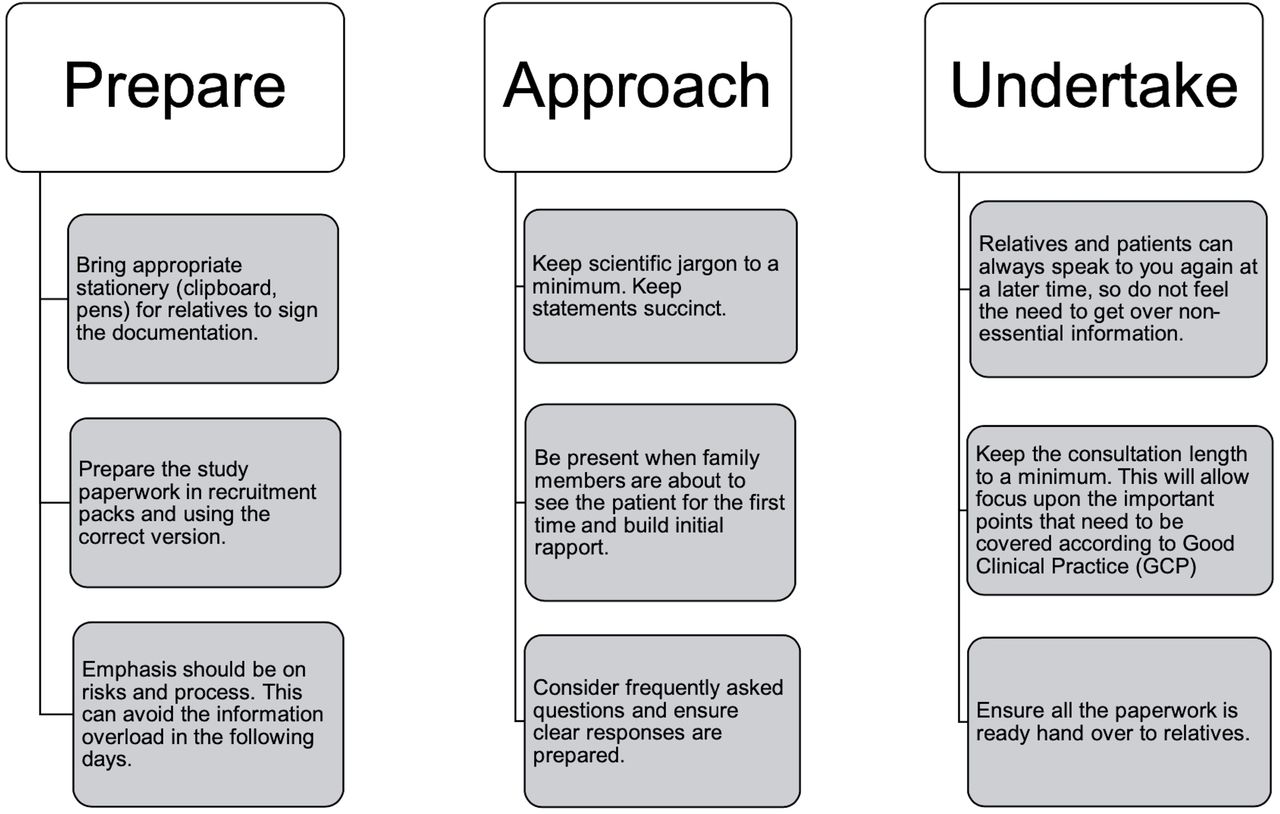
Members of the study team were always present when the returning casualty arrived at QEHB. Figure 2 provides guidance when preparing for the delivery of the consent process at this emotional time for personal representatives. An outline of the main concerns and reasons for participation when enrolling military patients to the study is detailed in Figure 3.

Important factors to consider when preparing, approaching and undertaking consent with soldier’s relatives.

Personal observations during the professional legal, personal legal and direct patient recruitment.
Study management
Practice makes (near) perfect
The SIRS study collaborated with the SGCNS to pool funds and resources during a period of high military operational activity. This offered an opportunity to maximise recruitment to both studies for shared benefit and to establish new research pathways that reflected those of the patients’ clinical care. To ensure seamless recruitment and minimise disruption to clinical activities, the research team ran recruitment simulations. These practices informed an understanding of the research burden on study participants and identified any potential challenges for patient volunteers and/or clinicians providing care. These simulations included rigorous assessment of the required study resources, identifying where study activities could be undertaken, the delegation of study procedures and planning the required measurement timings around essential patient care activities, as well as promoting the trial among clinical staff to build rapport and anticipate—and forward plan—for any complications.
When a study opens, research teams can be overenthusiastic to enrol their first patient to meet study recruitment targets. While it can be exciting to recruit patient volunteers in this manner, it may create additional work and complications due to misinterpretation of study protocols. This could leave early data sets inaccurate and incomplete, patients erroneously recruited and potentially the mismanagement of study samples.
Research Staffing
In what may appear to be a simple observational study, time and resource management in recruiting the required number of SP necessitated significant coordination and comprehensive study management. Initially, two researchers provided 24 hours, seven days per week cover for the study. However, such limited staffing could have led to low protocol compliance, poor study governance and staff fatigue.
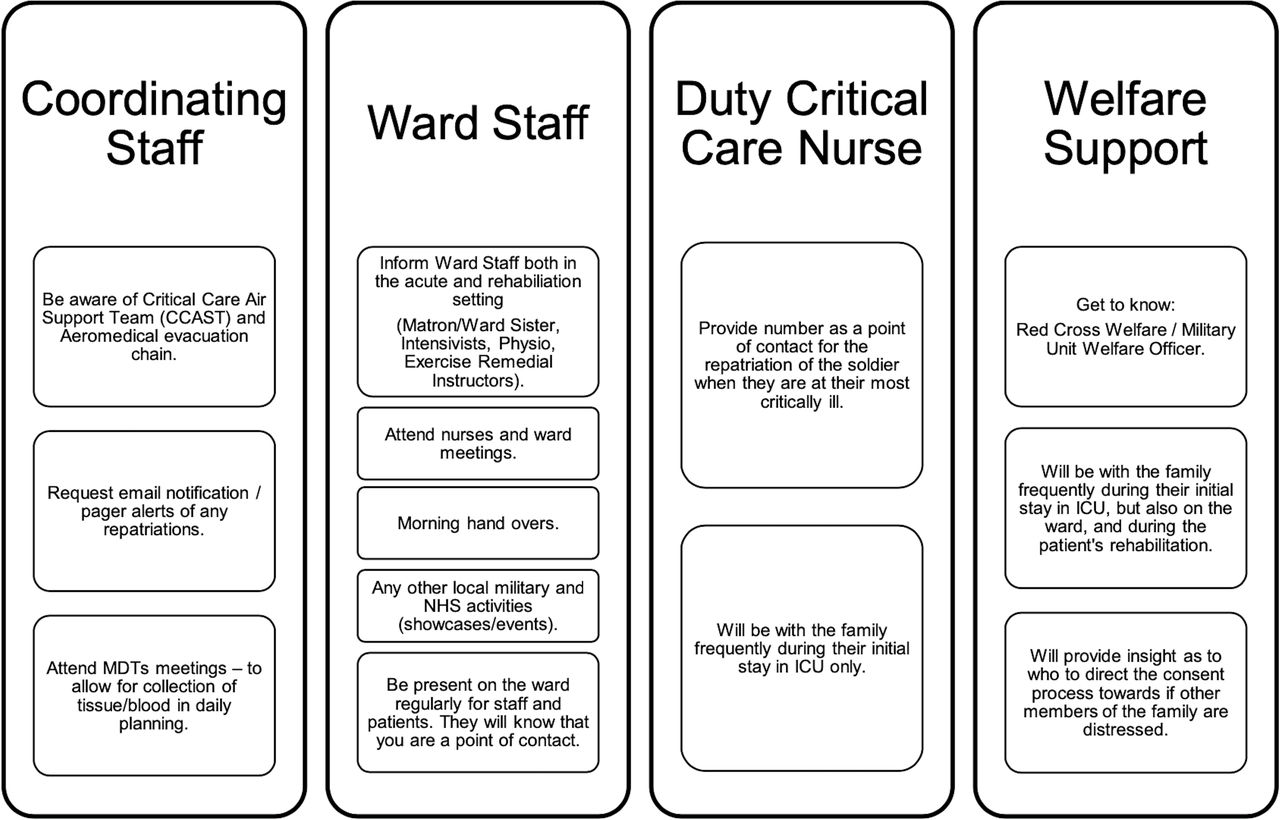
Multicentred military studies—such as the SGCNS and SIRS—hosted at both civilian and military clinical facilities, need an integrated military and civilian approach for the research pathway to be effectively managed. To that end, it is proposed that members of the research team should engage with the staff roles as detailed in Figure 4.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Important individuals with whom researchers should engage in undertaking research with soldiers(MDT: Mutlidisciplinary team; ICU: Intensive care unit).
Electronic data capture and coordination are essential
Handovers are commonplace within medical, allied health, nursing and social care environments; they provide essential information for the clinical team to highlight changes to a patient’s care plan. Research should be similarly conducted. The study team developed an electronic, automated patient scheduling system that detailed the date and time enrolled patients required study-related procedures to be completed.
Trial teams often work with a Clinical Trials Unit (CTU) to design an electronic case report form and accompanying database. These systems can represent a significant financial outlay and can be an inefficient use of time if data collection is duplicated. Furthermore, these databases may only be used for the specific study it was designed to support. An electronic tool to manage the movement of patients,perform data capture and sample collection was required, which was easy to use, accurate, adhered to local and national data protection regulations, and incorporated remote data collection for multiple studies from an extensive informatics system at QEHB. The study team also wanted to demonstrate the impact of clinical research on healthcare activity. At the time, there was little evidence suggesting how ‘activity’ might be recorded, other than documenting the number of accruals and time to recruit a patient.
The Clinical Research Tool (Crest) is a web-based clinical trial management system created by QEHB. Crest manages patient screening, recruitment and day-to-day tasks for multiple trauma-related trials. This has simplified the trial administration for front-line research teams, enabling more patients to be recruited and tracked and, by incorporating existing Trust IT systems into Crest, it has allowed more accurate and timely data collection.
Study improvement
Patient and Public Involvement
Without reflecting on the study with patients, the research approach and procedures could not be improved. The study team decided that a ‘research conference’ format would be the best means to provide feedback to servicemen and women and their relatives. Staff from QEHB and the former Defence Medical Rehabilitation Centre () at Headley Court were also invited to the event, thanking them for their support of the trial and also to disseminate the study findings. Staff are often informed about a study at the start, but frequently are not informed of the scientific outcomes at the end of recruitment to understand the impact and benefit derived from their assistance.
Relatives and patients
Due to the traumatic circumstances of the injury and the severity of patients’ presenting condition on return to the UK, the relatives naturally found it challenging to fully engage with the details of the study protocol. One relative commented that ‘…75% of the information went over my head’. Despite this, relatives agreed that the consent process was performed in a sensitive manner and at an appropriate time. Relatives reiterated that ‘…doing something is better than nothing at all’ and the action of the patient being involved in the research project allowed relatives to feel that something positive was being achieved from what was otherwise a negative experience. This also provided a sense of control during an uncertain time. Families stated that a single summary sheet of essential points would be far better than excessive explanations. Relatives were not interested in the relevant legislation and ethical governance of the study, which they felt unnecessarily added to the burden of information. Identifying the risks and the processes involved in study participation has previously been shown to be the most important factors to convey. 7It should, therefore, be the prioritised in the initial study visits.
Some relatives suggested that that the doctors and research teams ‘knew best’ and that they would do the best that they could under the circumstances. They stated that ‘…new things (surgery and drugs) have to be tried and tested’ and therefore they felt able to ‘…trust the judgement and decision’ of the medical and research staff. Previous work has identified that patients take part in research due to the recommendation from their doctor and through the doctor’s influence.8 The study team debated this position with the study patients and their families, and there were no feelings that the professional status of the research staff influenced their decision to take part in the study or not. The patients and their relatives have since helped inform and direct future interventional studies currently ongoing in the Surgical Reconstruction and Microbiology Research Centre.
Staff
As with any large acute trust—especially the QEHB with its mix of NHS and Royal Centre of Defence Medicine employees—staffing is shift-based and transient. As such, having just one introductory session to explain a study that is being performed on a ward may be insufficient. It was suggested by QEHB staff that regular updates are required throughout the entirety of an actively recruiting study.
As study team members were ever-present on the ward and in the intensive care unit (ICU), it was possible to overcome potential barriers to effective communication. Ward presence had an enhanced benefit by providing continuity for the patients and their relatives—as well as clinical care staff.
As the study was observational, there was no possibility that participants could have been immediately benefited by the study outcomes. However, work undertaken previously has identified that being part of research—even observational studies—has tangible benefits to patients, including increased medical monitoring and support, physical improvement and the prevention of further illness.7 Indeed, the clinical staff reported feeling that patient care was enhanced through study participation. The added value of the research team working closely with the clinical team could improve the overall, holistic patient experience and contribute towards a more positive view of healthcare. Teamwork was reflected in the comments QEHB staff received from families, often discussing the study with clinical staff and ensuring adherence to the protocol.
The main concern of ICU staff was that sampling should occur later than the 07:15–08:15 time period. This was similarly raised by patients, stating that once they were on the ward and at DMRC, they preferred fewer early morning disruptions. Therefore, future studies that are centred around times of high operational tempo will need to take into consideration the sample schedule, the resource allocation and the length of time to undertake study-specific procedures among the onerous clinical requirements.
Research needs to be similarly considered as important as clinical care; the two can be mutually beneficial if appropriately scheduled and managed. To facilitate this, the research team made efforts to concurrently collect clinical and research samples. Subsequently, barriers were broken down between the study team and the clinical staff, and this is an ethos that has endured at QEHB for subsequent studies.
Summary
For trauma research to be a success, it is vital to recruit patients at the earliest stages post-injury, to gather highly valuable information that can support the development of novel interventions. Relatives and independent treating clinicians must be engaged from the outset. Therefore, a study team must educate, inform and disseminate regularly to clinicians, nursing staff, allied health professionals and those who play an essential role in the holistic side of recovery. Involving families from the outset of a study shifts control back to the patient and their families. Although research may not influence a patient’s clinical outcome, it may provide other tangible benefits. More importantly, it could provide a definite sense of purpose and reward; the biological samples and data that patient volunteers have donated may be felt to help future injured military personnel, and NHS patients too. Logistically, it is crucial not to be complacent when considering workloads. Ward and laboratory procedures supporting essential research activity will require adequate resource, planning and practice. Collaborative working relationships are required between NHS and other agency colleagues to improve workstreams and productivity. Ultimately, everyone should be encouraged to be involved in recognising the significant contribution of military patients to clinical research, enhancing the care of future patients and continuing to push the boundaries of medicine.
Footnotes
Contributors CB, LC and JF have written the personal view. All authors approved the final manuscript.
Funding This study/project is funded by the National Institute for Health Research (NIHR) Surgical Reconstruction and Microbiology Research Centre (SRMRC). The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care. The SIR Study was part of the Surgeon General’s Casualty Nutrition Study (SGCNS), a Ministry of Defence funded project).
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; internally peer reviewed.