Article Text

Abstract
The use of strength and conditioning (S&C) in musculoskeletal rehabilitation has gained wide acceptance among the rehabilitation community. However, there is an absence of evidence demonstrating how to best integrate the principles of S&C into rehabilitation practice. This article discusses four broad themes: (1) an overview of the UK Defence Rehabilitation care pathway, (2) the historical and current approaches to physical training to support operational readiness of the British Armed Forces, (3) the current and future challenges of integrating S&C into Defence Rehabilitation practice and (4) research priorities relating to the use of S&C in Defence Rehabilitation. We detail the importance of strength/power-based physical attributes within our military population. We recommend that consideration be given to the benefits of an alternative education/coaching-based model to be used during the current 3-week residential care pathway, which aims to ensure effective implementation of therapeutic S&C over a longer period of care.
- rehabilitation medicine
- occupational & industrial medicine
- musculoskeletal disorders
- orthopaedic sports trauma
- sports medicine
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- rehabilitation medicine
- occupational & industrial medicine
- musculoskeletal disorders
- orthopaedic sports trauma
- sports medicine
Background
The most common reason for medical non-deployable status among military personnel is musculoskeletal (MSK) injury.1 Soldiers injured during basic training, field exercise and sport may be unable to deploy on operations, while soldiers injured during deployment may not be fit to return to active duty.2 Subsequently, there is a large economic and operational cost to UK Defence associated with MSK injury. Functional status during rehabilitation is most closely associated with muscle strength.3 Therefore, maximising the potential for adaptations during strength training is a crucial factor in the progression of any MSK rehabilitation programme. However, there is an absence of evidence demonstrating how to best integrate the principles of strength and conditioning (S&C) into rehabilitation practice.4 A significant challenge lies in designing optimal rehabilitation programmes that facilitate both neurological and muscular adaptations while concurrently accommodating biological healing, recovery and patient safety.5 Historically, it has been widely accepted that to elicit significant gains in muscle hypertrophy and strength requires loads equivalent to a minimum of 70% of an individual’s one repetition maximum for a given movement.6 For individuals undergoing MSK rehabilitation, heavy-load resistance training can be contraindicated or they are limited by their symptomatic impairment, including pain and immobility, to attain the recommended heavier loads.7 Therefore, patients with MSK injuries are often advised to reduce their training load, potentially limiting the desired muscular response to treatment, presenting a challenge to effective service delivery. Despite these known challenges, the use of S&C in MSK rehabilitation has gained wide acceptance among the rehabilitation community. Therefore, the purpose of this clinical commentary is to discuss issues surrounding the challenges of integrating S&C principles into UK Defence Rehabilitation practice.
Overview of UK Defence Rehabilitation service delivery
UK Defence Rehabilitation services are provided through a tiered network within Defence Medical Services. This consists of unit-level primary care rehabilitation facilities (PCRFs), 14 regional rehabilitation units (RRUs) and the Defence Medical Rehabilitation Centre (DMRC) at Stanford Hall (formerly DMRC Headley Court). PCRFs are unit/station-based outpatient departments providing exercise rehabilitation therapy for acute MSK injury. Military personnel with injuries that are unsuitable or do not respond at this level of care are referred to RRUs to allow rapid access to imaging services and residential rehabilitation. This intermediate level of care nests between the PCRF and DMRC. DMRC delivers consultant-led residential rehabilitation for more complex and chronic disorders and injuries, including complex trauma, neurological injury or illness, and chronic or specialist MSK injury/pain. DMRC provides an interdisciplinary approach to rehabilitation with services, including occupational therapy, social work, mental health, prosthesis/orthosis provision, podiatry, speech and language, dietetics and pain management support. Each admission at the RRUs and DMRC is traditionally 3 weeks in duration (readmissions may be provided for more complex or chronic conditions). The overall aim of treatment at each level of rehabilitation care is to restore optimal function and to regain full occupational employability to maintain force readiness. While there is some evidence supporting the efficacy of this 3-week model of residential treatment,8–10 to our knowledge, there is only one descriptive study specifically investigating the integration of strength training into UK Defence Rehabilitation practice.11 The primary opportunity for clinical staff at RRUs/DMRC to provide treatment and facilitate favourable medium-term to long-term rehabilitative outcomes is during this 3-week residential admission. Delivery of the exercise component of the multidisciplinary team rehabilitation care pathway and overall responsibility for integrating the principles of S&C into rehabilitation rests with the exercise rehabilitation instructor (ERI) and the physiotherapist. It is acknowledged that there is a particular challenge integrating S&C practice into the residential RRU/DMRC settings. This complex challenge is therefore reflected as a focus for this clinical commentary.
Historical and current approaches to physical training to support operational readiness of the British Armed Forces
Military training can be physically and mentally demanding. Through necessity, it is vital that soldiers are prepared to function under the uncomfortable conditions they may be exposed to during combat. The UK military’s historical approach to physical training involved high-volume running, group circuits involving callisthenic-based exercise and marching with load.12 It was traditionally advocated that high levels of aerobic capacity and muscular endurance were the components of fitness most closely associated with operational readiness.12 13 However, the training culture of volume over intensity and aerobic conditioning over strength/power-based physical attributes has since been challenged. Many military tasks require an underlying level of muscular strength to perform.13 14 For example, handling heavy machinery, casualty extraction and performing functional tasks while carrying heavy load (ie, a Bergen).14 The ability to produce high quantities of force (maximum strength) provides the foundations of a soldier’s ability to create explosive movements necessary during close-quarter combat, jumping/landing, multidirectional speed and agility, sprinting and throwing.12 Therefore, improving or maintaining strength and power is essential to optimise the number of military personnel fit for operational duty. To meet this task, rehabilitation practitioners must individually tailor their programmes to meet the needs of the individual and the occupational standards expected by the British Armed Forces. Furthermore, strength training is consistently shown to be a key component of MSK injury prevention strategies.15 ERIs and physiotherapists across UK Defence Rehabilitation should become familiar with the updated physical employment standard (PES) and, in particular, the 6-monthly soldier conditioning review (SCR) that measures a soldier’s (army-specific) ability to perform various components of fitness (see online supplemental file). Rehabilitation outcomes following traditional MSK injury should therefore be assessed against these new physical standards and gym-based assessment criteria. The updated PES provides a strong rationale for prioritising the development of these strength and power-based physical attributes towards the end stage of rehabilitation and reinforces the importance of why ERIs and physiotherapists must understand the principles of S&C and how to integrate them into MSK rehabilitation. Strategies to improve strength and power during rehabilitation using athletic populations returning to high performance have been described elsewhere.16
Supplemental material
A summary of commonly used programme variables and monitoring methods is presented in Table 1. These guidelines are well established and widely accepted, but describe recommendations resulting from research using healthy adult populations.17–19 It is the challenge of incorporating these principles into UK Defence Rehabilitation practice that provides the focus for this commentary.
Examples of training variables and monitoring equations based on healthy adults
Current and future challenges of integrating therapeutic S&C into UK Defence Rehabilitation practice
Despite an abundance of information on the implementation of S&C principles with healthy adults, investigations regarding the application of these principles in MSK rehabilitation programmes (or therapeutic S&C) are lacking.4 Clear clinical reasoning relating to effective progression of therapeutic strength training is essential to achieve positive clinical outcomes.20 In the absence of evidence to inform decisions regarding the integration of S&C training in rehabilitation, it is recommended that rehabilitating a patient at the site of injury be considered similar to an untrained individual when designing their training programme.5 While useful as a means of progressing single exercises, this approach is limited in its ability to apply progressions within a multidimensional rehabilitation programme at different stages of a patient’s recovery.20 Consequently, it is difficult to justify the use of formulas and principles for the physiological adaptation to S&C established with healthy adults as a basis for clinical reasoning in the rehabilitation setting.
Figure 1 presents a model that describes the challenges of applying ‘mainstream’ S&C principles into a complex multimodal rehabilitation programme. In this context, the term mainstream applies to the accepted knowledge and principles derived from research using healthy adults. In this model, the horizontal axis represents a continuum of physical function ranging from low to full functional capacity. The application of mainstream strength training principles (eg, intensity, duration, frequency and exercise order) is maximally exploited when approaching the later stages of functional recovery but is less applicable when physical function is significantly impaired, particularly in the presence of pain. This is represented in the model by the blue triangle and proportional vertical arrows. The green triangle and arrows represent the integration of therapeutic/restorative strength training principles and knowledge employed in the clinical rehabilitation setting. This knowledge is principally applied with patients at the early stage of functional recovery with less reliance at the ‘higher functioning’ end of the continuum. Therefore, while acknowledging a degree of overlap during functional recovery (Figure 1, shaded rectangle), this model visually shows an inverse relationship between the integration of mainstream versus therapeutic resistance training knowledge, principles and techniques at different stages of the recovery process. However, in the absence of clear guidelines on the integration of therapeutic strength training, decisions on when to increase load and add an external resistance are disproportionately driven by mainstream strength training principles, with little or no rationale for such decision making in a clinical rehabilitation programme. We would argue this approach promotes eminence rather than evidence-based practice. The examination of what constitutes an optimal therapeutic strength training programme is a research priority for UK Defence Rehabilitation.
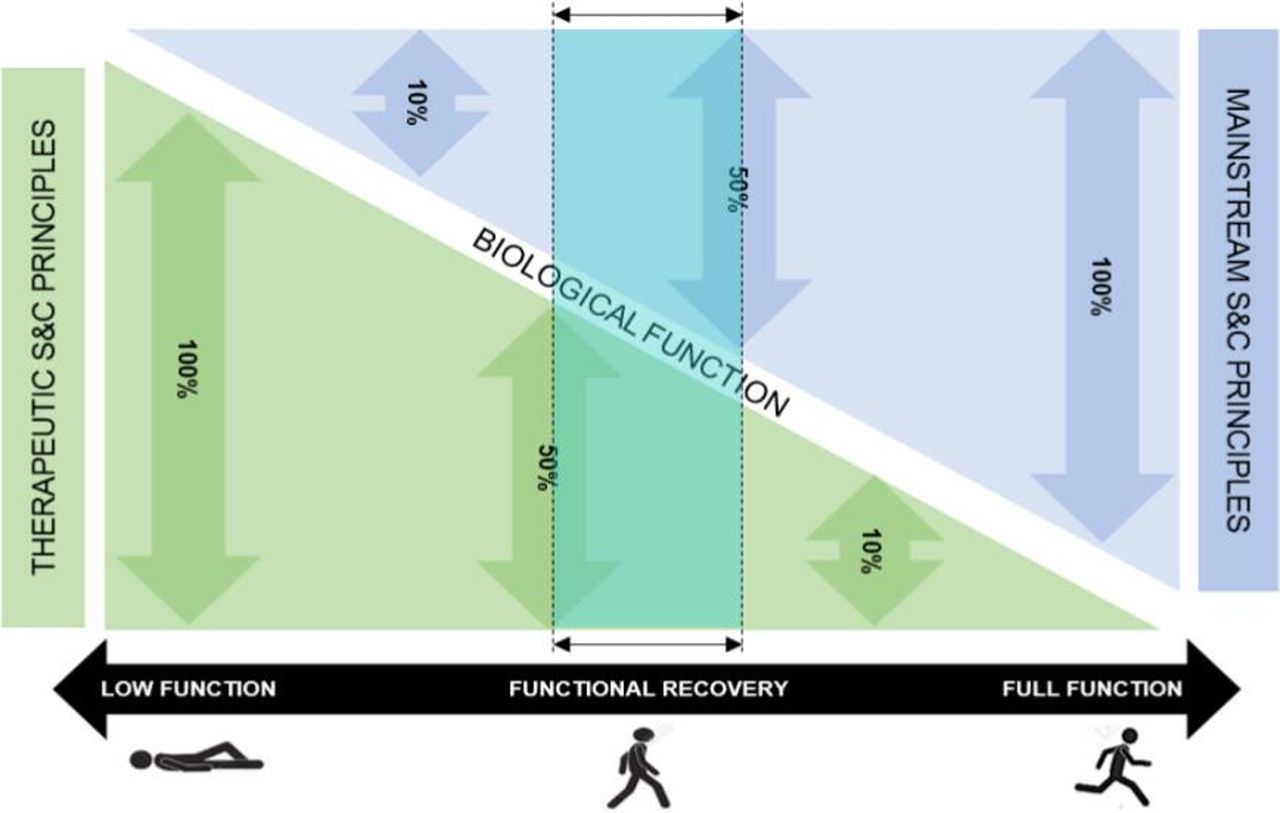
Coppack and Ladlow's theoretical model of the challenges integrating ‘mainstream’ versus ‘therapeutic’ strength training principles across the rehabilitation functional continuum. S&C = strength and conditioning.
While the use of S&C within MSK rehabilitation has acceptance across UK Defence Rehabilitation, there remains much debate surrounding how best to integrate accepted principles into the current treatment care pathways. Tables 2 and 3 identify some of the common challenges and proposed solutions from a clinical delivery, education, training and research perspective.
Integrating S&C in UK Defence Rehabilitation: challenges and solutions related to clinical delivery
Integrating S&C in UK Defence Rehabilitation: challenges and solutions related to education, training and research
Figure 2 provides a template for exercise programme design considerations and how different components of therapeutic S&C should be prioritised and progressed from point of injury to discharge from rehabilitation care, while taking into consideration operational ‘group’ and using the updated PES (using the Army PES as an example). During the restorative recovery (figure 2, phase I), the priority is promotion of pain-free movement. Once the therapist is satisfied the patient has completed the early restorative phase, they will perform a thorough needs analysis and identify which occupational group the patient most closely aligns with: group 1: medically discharged (return to civilian life and community reintegration); group 2: sedentary role (eg, desk-based role, low physical demand); group 3: low operational tempo (eg, this will be a unit who has just returned from ops and is just required to meet normal single-service physical testing criteria relevant); group 4: medium operational tempo (eg, units that are about to enter the readiness training cycle for future deployment); group 5: high operational tempo (eg, units that are undertaking training for deployment or units that have ongoing operational commitments, eg, special operations forces). The length of the blue arrows reflects the level of function, training load and physical capacity requirements to meet operational readiness. Operational readiness is determined using the updated PES. Groups 2 and 3 reflect non-ground close combat (GCC) (army non-GCC, not yet complete, to be published in 2021/2022); groups 4 and 5 represent army GCC (see online supplemental file 1). Preparing the injured serviceperson for operational readiness (figure 2, phase II) will require a semistructured, progressive periodised training programme.
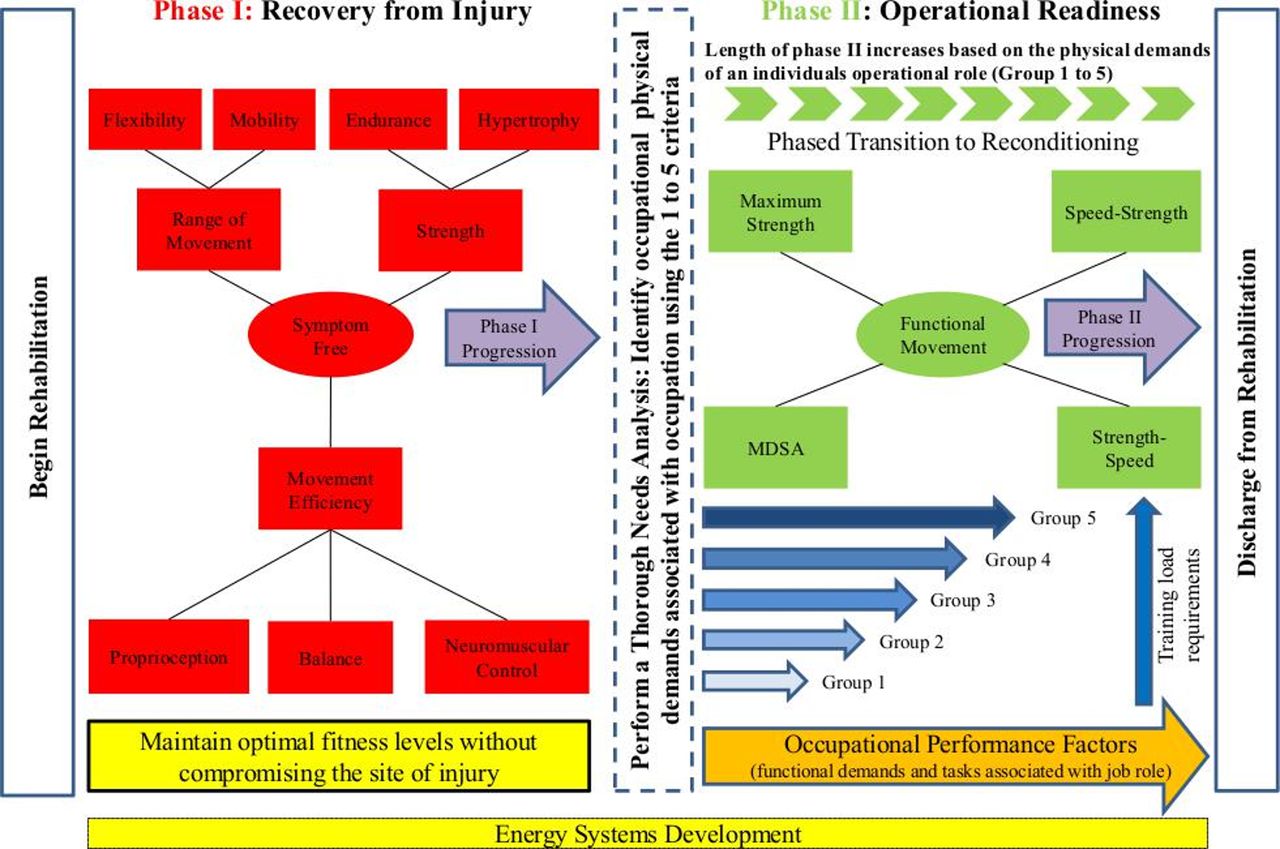
Ladlow and Hayhurst's therapeutic S&C progression model following musculoskeletal injury in UK Defence Rehabilitation. MDSA, multidirectional speed and agility; S&C, strength and conditioning.
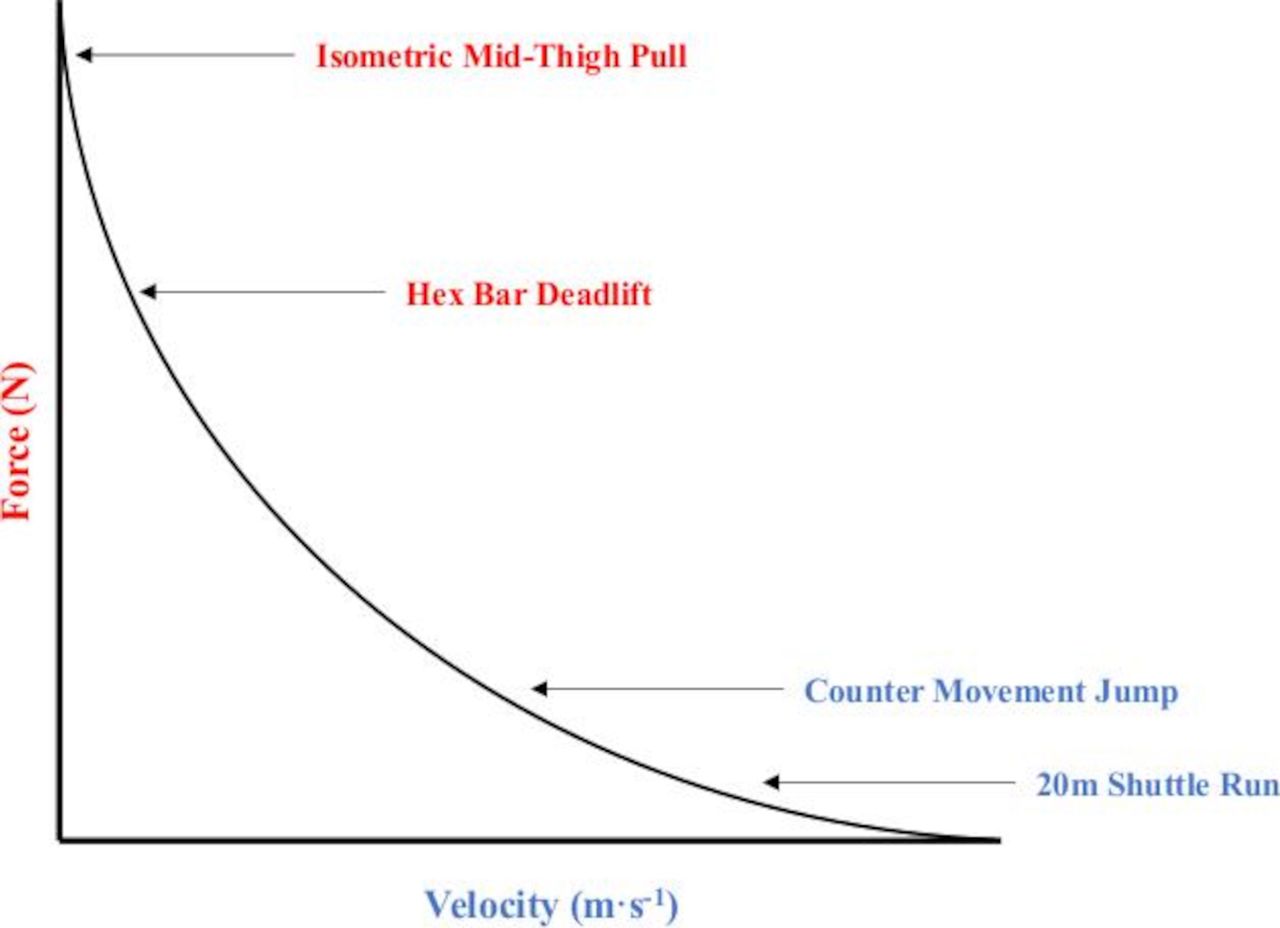
One of the most important challenges raised in Table 2 is the lack of objective performance-based outcome measures that can be directly used to inform current and future exercise prescription and programme design across all tiers of UK Defence Rehabilitation. Using examples of measurements currently used within different components of the PES whole career testing continuum (during entry selection, end of basic training and in-service); figure 3 plots these measures against a force–velocity curve. This approach to testing can provide therapists with a simple yet more diagnostic representation of their patient’s force-generating capacity, which can be quantified and monitored over time against the updated employment standards expected by the British Armed Forces.
{kind=link}
{kind=link}
{kind=link}
Physical performance measures used within the updated (Army) physical employment standards plotted against the concentric portion of the force–velocity curve.
Research priorities
UK Defence Rehabilitation must respond to and incorporate an ever-evolving evidence base to meet the needs of its injured personnel while remaining sufficiently flexible to meet the dynamic/changing priorities of the Defence Medical Services and UK Military. Research priorities relating to the integration of S&C into MSK rehabilitation include optimal loading to aid safe progression that simultaneously accommodates tissue healing and recovery while achieving strength/hypertrophy adaptations. A review of how exercise therapy is currently prescribed and managed across Defence Rehabilitation (particularly during the structured 3-week residential care model delivered at RRUs/DMRC) is warranted. In addition, determination of whether rehabilitation outcomes are optimised using alternative methods of delivery (an education-based model) should also be considered.
Summary
In this clinical commentary, we detail the importance of strength and power-based physical attributes within our UK military population and reinforce the reasons why medium-term to long-term MSK rehabilitation training programmes could potentially be designed to reflect the updated PES. We provide some areas for consideration that may address these commonly cited challenges. We discuss the potential benefit of developing objective performance-based outcome measures that can be used across all tiers of Defence Rehabilitation that more closely reflect the updated PES/SCR. We would also recommend that consideration be given to the benefits of an alternative education/coaching-based model that aims to ensure effective implementation of therapeutic S&C over a longer period of care (eg, 3 months). Determining optimal loading to aid safe progression of strength/hypertrophy adaptations while simultaneously accommodating tissue healing and recovery is poorly understood across the global MSK rehabilitation community and has now become a research priority for UK Defence Rehabilitation. This article was written immediately prior to the COVID-19 outbreak in the UK. Therefore, it is too early to speculate on what impact the ongoing contingency measures may have on long-term service delivery in Defence Rehabilitation.
Ethics statements
Patient consent for publication
Acknowledgments
The author’s thank all staff and patients across UK Defence Rehabilitation for their support and contribution to this article. The authors also thank Vanessa Walters (Academic Department of Military Rehabilitation) for her technical input and comments on the final draft.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors PL and RJC conceived the study idea. PL, DC and RJC wrote the first draft. DH, CS and RPC reviewed and provided detailed comments and revisions on the first draft. All authors participated in further revisions and provided their full approval prior to submission.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.