Article Text

Statistics from Altmetric.com
- INFECTIOUS DISEASES
- INTERNAL MEDICINE
- MENTAL HEALTH
- ORTHOPAEDIC & TRAUMA SURGERY
- ACCIDENT & EMERGENCY MEDICINE
- BASIC SCIENCES
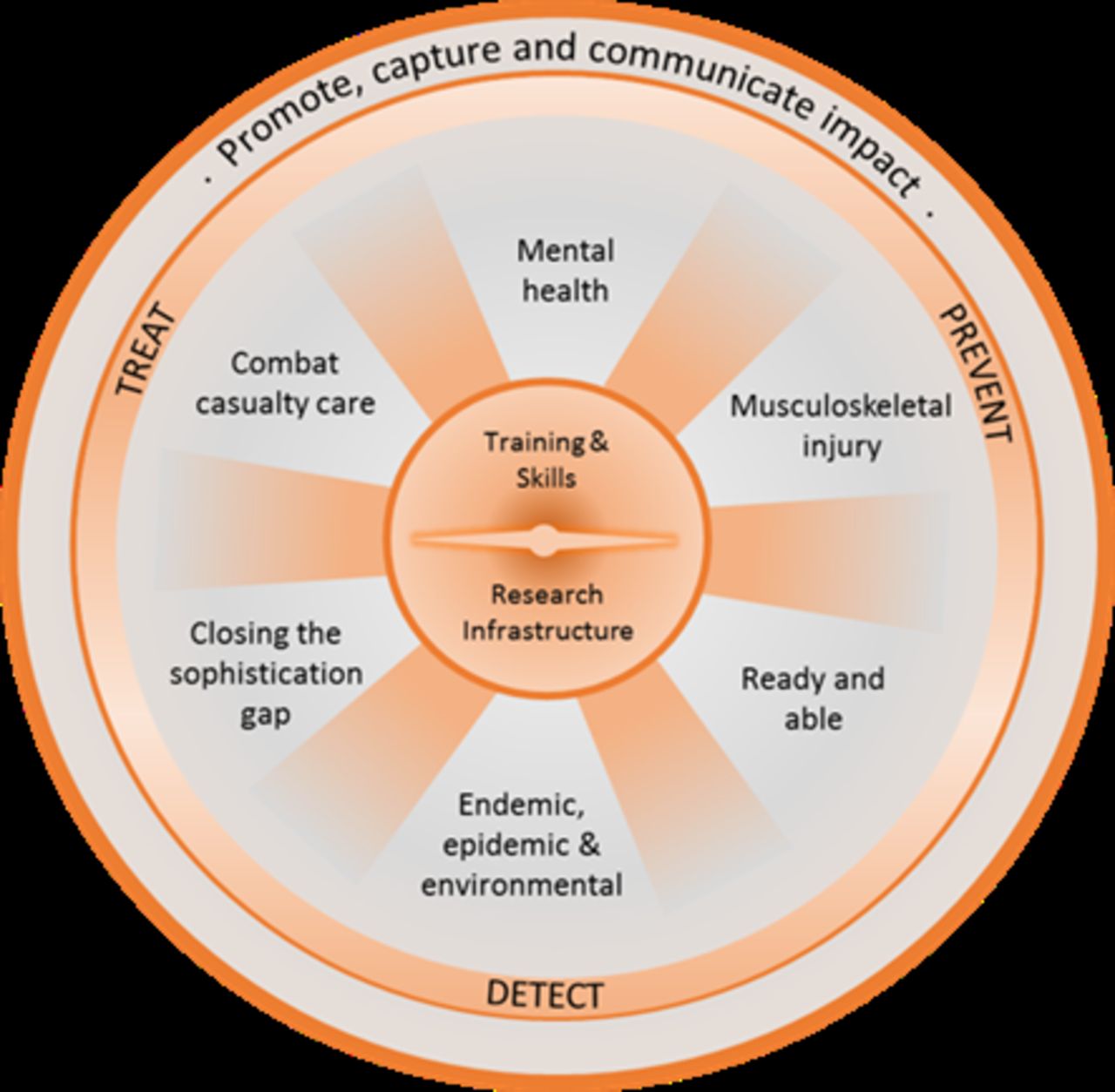
November 2021 saw the launch of Avoiding the Walker Dip: A Strategic Delivery Plan for Defence Medical Services (DMS) Research 2021–2026 (SDP 21). It had a three-pronged purpose (see Figure 1): to set priority research themes for the near to mid-term future, to highlight ways in which underlying research capability will be strengthened and to outline how the impact of DMS research should be captured and communicated.

{kind=link}
Schematic summarising the priority research themes, underlying capability requirements and requirement to capture and communicate impact inherent to SDP 21. SDP 21, Avoiding the Walker Dip: A Strategic Delivery Plan for Defence Medical Services (DMS) Research 2021–2026.
The ‘Walker Dip’ refers to the regression in military medicine that occurs between conflicts that is repaid in the lives of service personnel at the start of the next campaign.1 The implementation of SDP 21 is well underway and is geared towards avoiding any regression of momentum in research and innovation across DMS. A new governance structure now coheres and oversees DMS research and includes the formation of working groups to drive activity under the six priority themes. Plans to establish a research tissue bank, a research repository and improved early-career research opportunities are all in train. New mechanisms for reporting research outcomes and impacts have been initiated.
These initiatives sit firmly within the DMS sphere of control and can be pursued by its Research and Clinical Innovation (RCI) pillar. Outside of RCI are layers of stakeholders at increasing distance starting with supporting DMS functions and radiating outwards through UK Defence partners, external UK organisations and international collaborators. Realising the ambition of SDP 21 will depend on DMS embracing the complexity of this research ecosystem, attempting to drive innovation where influence can be brought to bear and making the most of opportunities that are presented at every level.
RCI must maintain its own capability to innovate.2 It must be agile and responsive to rapid demand signals from within DMS and from front line commands. Indeed, within SDP 21 research priorities were specified at broad theme and topic levels to allow this agility and we have already seen this bearing fruit: novel research projects addressing, for example, immunosuppression in basic training have been initiated as a result of demand signals being fed from 1* Boards into Research Theme Working Groups (RTWGs). Further routes must be established that allow capability branches to feed in their requirements in a similar manner, so we are responsive to emerging threats beyond our immediate horizon.
RCI has a responsibility to provide leadership when areas of concern arise within the Joint medical space. Recently, the dearth of evidence for the burden, mechanisms of injury and effects of whole body vibration has prompted RCI to lead on establishing a multi-million pound research programme in this area. This will be launched via the Defence and Security Accelerator making good use of resources and expertise that sit within other areas of Defence. RCI will continue to pursue novel routes to access the research base within academia and industry especially when faced with complex and wide-ranging evidence gaps that cannot be tackled by internal expertise.
Similarly, RCI will continue to be nimble in aligning its in-house capacity to areas of emerging need. The recent appointment of an inaugural Senior Lecturer in chemical, biological, radiological and nuclear medicine speaks to this commitment.
DMS supporting functions—commercial, financial, legal—sit at the next stakeholder layer and play a critical role in ensuring public money is well spent. Balanced against the rigorous governance requirements for public funds is a requirement for supporting functions to show the flexibility necessary to deliver high quality research in conjunction with academic partners. Risk tolerance is a critical component of an innovative ecosystem.3 A shift from a one-size-fits all approach to contracting towards a risk-based approach that accounts for the nuances of supporting a research project vs traditional Defence procurement would help accelerate the pace of innovation.
Existing in the Joint space, DMS is positioned in the centre of a web of connections across Defence. Some of these connections are with departments directly engaged in research, science and technology. The formation of the RTWGs has strengthened long-standing links to the Defence Science and Technology Laboratory (Dstl), Institute of Naval Medicine and Army Health Branches. In the short term, this will assure coherence and reduce redundancy. In the long term, this will encourage new shoots of research that leverage the combined expertise and capability across departments. This connectivity is bidirectional with DMS researchers jointly chairing Dstl working groups and providing clinical insight to Dstl-led projects. Other connections reach into areas of Defence that are on the receiving end of research outputs with implications for their policies and practices. For DMS research to have the biggest possible impact, stakeholders such as Defence Equipment & Support and Health, Safety & Environmental Protection must be brought into discussions early to help set research priorities and where possible to provide support to help investigate them.
Outside of Defence, it is important that new collaborations are fostered with industry and academia and engagement events are planned throughout the period of SDP 21 to enable this. At the same time, it is as important to realise that research is often the result of long-standing collaborations between partners that share common understanding of a project’s history and future direction. Internal policy and process must encourage researchers to maximise the value of these relationships for Defence benefit rather than put up barriers to their use.
Beyond industrial and academic collaborators are other government departments (OGDs), such as the Department for Health and Social Care and Office for Veterans Affairs, and bodies including UK Research and Innovation that will be better engaged over the course of SDP 21. Despite hosting a wealth of exceptional military academic talent, DMS is afforded less than 1% of Defence’s R&D budget.4 As such, leveraging additional funds via OGDs, other public bodies and charitable partners is essential for the long-term sustainability of research effort. The key to this engagement is pinpointing research areas that straddle the boundaries between military and civilian and serving and veteran interest. Traumatic brain injury, regenerative medicine, remote monitoring, pain relief and mental health are clear examples of where mutual benefit can be derived through closer collaboration and sharing of resources.
Finally, and in a similar vein, many of the military medical challenges facing the UK Armed Forces are shared by our allies (and adversaries). By working with partners to solve these challenges, we can devise better, interoperable solutions more quickly and at a lower cost to UK Defence. An ongoing research collaboration with the USA to prevent and treat enteric diseases on operations demonstrates what can be achieved with pooled funding, a larger treatment population, wide geographical reach and shared intellectual contribution. This programme relies on an openness to share problem sets, data, intellectual property and expertise with a NATO partner and there is no reason why this model of cooperation cannot be mirrored in other research areas with other allies.
SDP 21 crystallised the military medical challenges facing DMS under six research themes. Addressing these challenges—and avoiding the Walker Dip—requires not just the alignment of RCI effort, but pragmatism of its supporting functions, and the positive exploitation of links within Defence, across industry, academia, OGDs and beyond. Only by doing so will the ambition of SDP 21 be fully realised.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Footnotes
Contributors PW conceptualised, drafted, refined and finalised the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.