
Abstract
Purpose
Early central venous catheter (CVC) insertion in Ebola virus disease (EVD) is a novel approach and has not previously been described. This report delineates the safety, feasibility and clinical implications of early CVC insertion as the optimum means of vascular access in patients with EVD, in the setting of a deployed military Ebola virus disease treatment unit in Sierra Leone.
Methods
In the gastrointestinal phase of EVD, a 7-French 20-cm triple-lumen CVC was inserted using aseptic technique. Data were collected prospectively on all cases to include baseline and subsequent blood test variables, insertion site and technique, and complications associated with CVC placement.
Results
Twenty-three patients underwent CVC insertion as follows: subclavian, 21 (88 %); internal jugular, 2 (8 %); axillary, 1 (4 %). The mean duration of CVC placement was 5 days. There were no significant procedure-related adverse events. Despite coagulopathy being present in 75 % of cases, CVC insertion was safe, and there was only 1 case of significant catheter site bleeding. A total of 152 needle venepunctures were avoided owing to the presence of a CVC, a mean of 7 (±3.8) per case over the average stay.
Conclusion
The early use of CVCs in Ebola virus disease is safe, effective and facilitates patient care. It should be considered a feasible additional route of venous access, where physician expertise and resources allow.
Similar content being viewed by others

Background: the Ebola virus disease outbreak
In March 2014, the World Health Organisation was formally alerted to the current West African outbreak of Ebola virus disease (EVD), which rapidly developed into the largest and most complicated in history [1–3]. Caused by the transmission of Zaire Ebola virus (EBOV) in body fluids [4], the disease is characterised by a clinical syndrome of a viral prodrome, followed by severe gastrointestinal involvement, intravascular volume depletion, and multi-organ dysfunction due to both direct viral injury and a systemic inflammatory response syndrome (SIRS) [5–10]. Currently, no specific antiviral therapies have been proven to be of benefit. Investigations into the possible efficacy of human convalescent plasma, humanised monoclonal antibodies, interfering RNA drugs and viral RNA polymerase inhibitor therapies are ongoing [11]. The condition is often fatal, with an aggregated case fatality rate of up to 75 %—the highest of the Ebola strains [12, 13]. There is considerable risk of transmission to those caring for patients with EVD [14–18], and special personal protective equipment (PPE) with strict attention to infection prevention and control procedures are mandated [19–22]. Control of the outbreak has been further compounded by its occurrence in a zone struggling with poverty, dysfunctional healthcare systems, and its spread from rural areas into urban settlements and across international borders [23, 24].
In August 2014, the World Health Organisation declared the outbreak a public health emergency of international concern, and called for a strong and coordinated international response [25]. As part of the UK’s contribution, a 12-bed military EVD treatment unit (EVDTU) was deployed to Sierra Leone. Its main aims were to provide intensive medical care for healthcare workers either as a bridge to recovery, or prior to aeromedical evacuation [26]. The clinical team comprised a bespoke multidisciplinary physician cadre of senior intensive care medicine, acute internal medicine and infectious disease specialists, combined with acute nursing personnel, laboratory staff, and administrative and command elements. The clinical aim was to provide safe, effective care at a level as close to that available in the UK as practicable, within the logistic and environmental limitations inherent in operating in West Africa [19]. Equipment deployed included extensive PPE and all the items required to provide intravenous volume replacement, concentrated electrolyte solutions, antimicrobial therapy, gastric protection, and symptom control agents. In addition, the EVDTU deployed with a stock of blood products, and with on-site laboratory support able to provide Ebola diagnostics by means of real-time quantitative reverse-transcriptase polymerase chain reaction, plus standard haematology and biochemistry assays. Near-patient testing was also available within the EVDTU “Red Zone”, using the handheld Abbot iSTAT 1™ system, combined with Chem8+, CG4, and ACTk test cartridges.
The most important initial aspect in providing care to patients with EVD is believed to be the conscientious correction of volume and electrolyte losses. Certainly, the provision of early oral rehydration therapy using electrolyte solutions is cheap, and easy to administer in almost any setting. However, in the vast majority of patients, once the disease progresses, severe lassitude, fatigue and vomiting prevent this from being a viable therapy beyond the first few days of illness [27]. Even if oral therapy were to provide adequate water input, it would not be sufficient to provide electrolytes in the quantities needed to keep pace with gut losses of up to 5 L daily during the diarrhoeal phases of illness [28]. Significant dehydration and severe sepsis combine to put patients at increased risk of acute kidney injury—a condition with sinister consequences in the setting of any severe systemic infection [29–31]. Without adequate electrolyte replacement, profound hypokalaemia and hypomagnesaemia ensue, which may contribute to the sudden deaths noted in EVD outbreaks, possibly related to malignant ventricular arrhythmias. Additionally, marked hypophosphataemia, noted especially as part of a refeeding syndrome in the recovery phase, frequently required intravenous therapy in patients in the EVDTU [32, 33]. Despite the obvious requirement to augment or replace oral intake with parenteral fluid and electrolyte therapy [34], across the outbreak the uptake of intravenous therapy has been lower than required [35]. We postulate that intravenous therapy will be required in all but the mildest cases, ideally augmented and guided by laboratory or near-patient electrolyte testing.
Early CVC insertion is a novel approach in EVD, and although common in critical care practice [36, 37] its routine use has not been previously reported [38]. In the EVDTU it was used as a means of optimising intravascular access, allowing the delivery of concentrated electrolyte and volume replacement solutions, and to facilitate easier access to repeat blood samples.
Methods
Initial management and EVD staging
All patients testing positive for EVD were admitted to the EVDTU. On admission, their disease was staged according to clinical syndrome. Disease stages are outlined in Table 1. Acute kidney injury was defined using the Risk, Injury, Failure, Loss and End-Stage Kidney classification [39].
For patients in Stage 1, early oral rehydration was encouraged, baseline haematological and biochemical tests were performed, and peripheral venous access was obtained. Intravenous fluids were commenced at this point if oral intake was inadequate and/or if clinical and laboratory variables suggested dehydration (characterised by elevated urea, creatinine or haematocrit). On developing Stage 2 disease, if not already performed, intravenous fluids were commenced with daily monitoring of blood biochemistry. More frequent sampling was performed if clinically indicated. Serum magnesium and phosphate levels were checked on alternate days, where laboratory availability permitted. All patients in Stage 2 of the disease were considered for central venous access, and the decision to proceed was made by the physician team on the basis of clinical indications, disease severity, and following a risk–benefit assessment.
CVC placement
CVC placement was achieved using an Arrow™ multi-lumen central venous catheterisation set, comprising a 7-French, triple-lumen 20-cm catheter, with antimicrobial silver sulphadiazine and chlorhexidine acetate surface treatment. After gaining informed consent, insertion was performed by a senior, experienced physician in full PPE comprising a protective barrier suit, boots, endoscopy apron, visor and double nitrile gloves (Fig. 1). An assistant was made available during the insertion process. The insertion site was selected at the operator’s discretion, and an Accuson Freestyle™ ultrasound device was usually available within the EVDTU. Full aseptic procedures were employed, including skin preparation using chlorhexidine, followed by sterile drapes. On top of the PPE, following washing the gloved hands in a 0.5 % chlorine solution, a further sterile gown and sterile gloves were worn. Local anaesthetic was infiltrated, and 2-mg aliquots of intravenous midazolam for sedation were administered at the operator’s discretion. Pulse oximetry was performed throughout to monitor heart rate and oxygen saturations. Although electrocardiographic monitoring was not routine it was immediately available, as was an external defibrillator, in case of induction of an iatrogenic malignant tachyarrhythmia during insertion of the guide wire. A Seldinger technique was used for CVC placement, using a 6.35-cm 18-gauge needle attached to a Raulerson spring-wire introduction syringe, through which a 45-cm 0.32″ guide wire with a soft “J” tip was introduced. As a result of concerns about possible CVC dislodgment in patients with agitation secondary to encephalopathy, all lines were fully inserted to 20 cm, and secured firmly using three interrupted 2/0 silk sutures. Needlestick injury (NSI) during CVC suturing has previously been a cause of healthcare worker infection. In order to avoid this all needle handling was performed using sterile needle-holders and forceps. Following suturing, all lumens were aspirated to confirm function, and a two-way sterile needle-free access system attached to each lumen prior to flushing. A standard transparent CVC site dressing was then applied. Routine follow-up included regular nursing observation of the CVC site, and a daily inspection by the EVDTU physicians. There was no facility to perform a chest radiograph within the EVDTU.

Military EVDTU consultant inserting a central venous catheter under aseptic conditions whilst wearing full protective equipment plus additional sterile gown and gloves
Where a CVC was placed, demographic and disease staging data were collected, as were all current and subsequent blood test results. Data were also collected on the frequency of blood sampling, intravenous therapies delivered, and regarding the occurrence of any healthcare worker exposure incidents, either due to contamination with blood or via NSI. The results of periprocedural and postprocedural cardiac and lung ultrasound examinations were also documented.
Results
During the 56 days of the reporting period, 38 patients were admitted to the EVDTU. Twenty-four (63 %) tested positive for Ebola, of which 15 were male, with a mean age of 34 (range 21–50). Seven patients were tertiary referrals, having undergone initial therapy at another Ebola treatment unit. Twenty-three patients underwent CVC insertion. Of these, 11 survived to discharge, one was transferred to a European centre and subsequently survived to discharge, and 11 died. The one patient who did not undergo CVC insertion received peripheral IV fluid and electrolyte replacement and was discharged after 3 days. Overall, the median duration of EVDTU admission was 9 days.
Indications and insertion techniques
Seven CVCs were inserted as a result of difficulty achieving peripheral IV access. This was defined as either one or more failed attempts at IV cannulation, or predicted difficulty following clinical evaluation. The remainder were inserted to allow delivery of concentrated potassium chloride infusion, and to increase the available access for multiple infusions, as all patients required IV maintenance plus antibiotics and other supportive agents. There was no facility to monitor central venous pressure.
CVC insertion was performed most frequently on the second day of admission (range 1–4). This took place on day 7 of illness in the majority of cases (range 3–11). The mean duration of CVC placement was 5 days overall, and 6.1 days in survivors, compared with 4.1 days in those who died of their illness.
There were no operator Ebola exposure incidents or NSIs related to CVC insertion, and no healthcare worker infections in the EVDTU during the reporting period.
Baseline variables
At CVC insertion, mean vital signs were as follows: respiratory rate 27/min, pulse 95/min, blood pressure 117/72 mmHg, temperature 37.9 °C. Coagulopathy, evidenced by abnormalities in activated clotting time (ACT), activated partial thromboplastin time (APTT), prothrombin time (PT), platelet count or the presence of overt abnormal bleeding, was common, and was present in 18 cases (75 %) at the point of CVC insertion. Interestingly, marked thrombocytopaenia was seen in seven cases (29 %). In these patients, the mean platelet count was 77 × 109/L at CVC insertion, falling to 74.8 at peak illness. Overall mean coagulation variables are shown in Table 2.
Technical aspects of CVC insertion
The following anatomical insertion sites were used: subclavian, 21 lines; internal jugular, two lines; axillary, one line. Insertion was performed easily, at first pass in 16 cases (70 %), at second pass in three cases (13 %). CVC insertion was recorded as being ‘difficult’ in four cases (17 %), but was successfully achieved in all cases at the initial attempt. Immediate complications were rare. There was one case of inadvertent carotid artery puncture, which occurred following temperature-related failure of the ultrasound device batteries, during internal jugular access. Following direct pressure, there was no ongoing bleeding, and an alternative approach was successfully used.
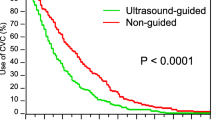
Ultrasound guidance was used during CVC insertion in 25 % of cases. However, 54 % underwent subsequent ultrasound examination to exclude pneumothorax, which itself has been shown to be superior to conventional chest radiography [40, 41]. Additionally, transthoracic echocardiography was performed which allowed us to confirm CVC tip placement in or near the right atrium, in keeping with a high uptake of echocardiography within our critical care practice [42–44]. Both of these examinations were performed together, within 24 h of CVC placement. In all cases where this took place, line placement was found to be satisfactory, and there were no cases of pneumothorax. All but two cases received small doses of midazolam as procedural sedation, and monitoring with pulse oximetry was performed in all cases throughout CVC insertion and until fully recovered. The maximum total dose of midazolam administered was 7.5 mg. There were no reported or documented adverse events associated with procedural sedation.
There were no confirmed episodes of CVC-associated bacteraemia. Blood cultures taken at clinician discretion from three cases with indwelling CVCs several days after insertion were negative.
Therapy via CVC
Following insertion, all cases received further electrolyte solutions via CVC, and all patients required concentrated potassium chloride (usually multiple aliquots of 40 mmol in 100 mL 0.9 % saline) to maintain serum potassium levels above 3.5 mmol/L. Intravenous magnesium supplementation was also required in all cases. A total of 48 % of cases also received blood products, most commonly fresh frozen plasma and cryoprecipitate. Platelets were infused in cases of profound thrombocytopaenia complicated by bleeding. In three cases, drugs were infused which require central vein access for safe delivery (norepinephrine, dopamine and amiodarone).
Blood sampling via CVC
Once a CVC had been inserted, all further blood testing was performed via this route. This avoided the requirement to perform further needle venepuncture. Over the reporting period, 152 needle venepunctures were avoided by implementation of the early CVC strategy—a mean of seven per case (range 1–15). This is particularly significant as the most critically ill patients generally required the most frequent blood sampling. Sicker patients have been shown to have the highest viral loads, and thus are likely to present the most risk to healthcare workers should contamination or NSI occur.
Discussion
Achievable with proper preparation and planning
Early CVC therapy appears to be achievable in this cohort of EVD patients treated within a military EVDTU. Insertion was achieved at the initial attempt in all cases, with an acceptable side-effect profile. Despite operating in high ambient temperatures whilst wearing cumbersome PPE, it was possible to follow standard infection control procedures by wearing an additional sterile gown and sterile gloves. Most importantly, there were no cases of NSI or significant contamination during CVC insertion. This was avoided, in part, by careful planning by the operator, and meticulous attention to sharps disposal discipline. All items were carefully pre-positioned prior to commencing the procedure, and an assistant was on hand to fetch any additional equipment, and to assist with procedural sedation as required. Also, all operators were senior consultants with daily responsibility for advanced vascular access procedures in their non-deployed hospital roles. No CVCs were undertaken by physicians who do not routinely perform the procedure. We feel that this is crucial to the successful use of CVCs in this way, and potential operators should be fully proficient in the technique before attempting to employ it in the harsh environmental setting of the EVDTU.
In this cohort, there was some oozing noted from CVC sites, most commonly immediately after insertion. Usually this responded to pressure dressings, and did not present a clinical or nursing problem. Only one case went on to have significant-site related bleeding, for which he received both red cell and component therapies, over the course of several days. Insertion of the CVC had been straightforward, and some of the total blood loss was also attributable to bleeding from other peripheral access sites. This patient had very severe EVD, as evidenced by multisystem involvement, and a long hospital course (12 days), though he eventually made a full recovery.
We acknowledge that, ideally, a control group would be of value for comparison, perhaps using only peripheral IV access. However, this prospective cases series is primarily intended to provide urgent descriptive data, and to inform on the feasibility of this mode of venous access to both deployed EVD treatment facilities and the wider intensive care community.
Facilitates fluid, electrolyte and drug therapies
The presence of CVCs made electrolyte administration straightforward. In our clinical setting, concentrated potassium and magnesium solutions were all delivered centrally via a syringe driver or infusion pump. To give the equivalent doses of potassium supplementation via the peripheral IV route, much more volume infusion would have been required. As our clinical practice and experience with EVD evolved, it appeared that there was some advantage in a carefully controlled fluid regimen, comprising focused electrolyte replacement with carefully titrated volume optimisation. This is in keeping with the broader critical care literature [45–47]. Rapidly infused volumes seemed to be associated with a tendency to develop relative hypoxaemia early in the disease process. Impaired gas exchange in Ebola patients is unforgiving, certainly when operating without the ability to institute mechanical ventilation. Avoidance of inadvertent over-filling facilitated by central delivery of targeted, concentrated electrolytes may assist in avoiding this situation.
Another benefit of reducing the volumes of sodium chloride solution delivered is a reduced incidence of iatrogenic hyperchloraemia. Recently published work has confirmed the adverse association between intravenous chloride load during resuscitation and in-hospital mortality in the setting of SIRS, and during perioperative and critical care fluid resuscitation [48, 49].
Drug administration in the EVDTU is often complex, with most patients in Stage 2 receiving intravenous antibiotics, vitamin K, ranitidine and paracetamol, in addition to background maintenance fluids. Half of the patients in this cohort also received blood products, and a number required continuous dextrose infusions. The number of access ports required would defeat a single peripheral IV cannula, necessitating further cannulation. On the basis of the number intravenous therapies delivered as part of the bundle of care, and the durations for which they were required, we calculated that to deliver EVDTU therapy to this cohort without CVCs, a minimum further 38 IV cannulations would have been required.
In addition to the problems in providing sufficient access for therapy, peripheral lines frequently dislodge. The risk associated with this event is significant—not only is therapy interrupted, but significant bleeding can occur especially in the presence of concomitant coagulopathy. Blood loss from EVD patients presents a risk to staff, and takes nursing personnel time and effort to safely contain it. Even once these issues have been addressed, further cannulation, with its inherent risks will then need to be undertaken. In the context of the heavily viraemic patient, agitated through encephalopathy, with the operator in PPE in a high ambient temperature, this is neither easy nor safe. In contrast, CVC dislodgement was rare, following assiduous attention to anchorage with sutures. Even if dislodgement does not occur, peripheral cannulae need to be observed carefully for signs of phlebitis and infection, and most national guidelines recommend changing them every 3–4 days [50, 51]. More cannulation sites effectively mean more potential bleeding points during the coagulopathic phase of the illness, and should be avoided.
The presence of a CVC was also a useful venous access adjunct in one patient who required aeromedical evacuation, allowing secure multilumen access for our staff whilst transferring the patient to the airhead (a 2-h road move), and during the patient’s 6-h flight to a European facility. During the flight he required therapy with intravenous drugs and was given fresh frozen plasma for coagulopathy. The receiving hospital team also used the CVC for drug administration and sampling on the patient’s arrival. Marked hypovolaemia following aeromedical transfer has been a feature of a number of recent cases in the literature, in one case compounded by inability to achieve venous access during the flight [28]. Our group has significant operational experience of providing medical support to critically ill patients in-flight [52], and insertion of a CVC prior to aeromedical evacuation greatly enhances the ability to deliver maintenance fluids, volume support and other drugs during a potentially long, hazardous transfer.
Regular sampling easier
CVC placement facilitates regular blood sampling by removing the need for repeated venepuncture. All interventions with sharps should undergo a dynamic risk–benefit assessment in the setting of EVD patients, as they have the potential to cause harm to the patient by generating pain, and by forming a new potential bleeding site. Bleeding from old venous access and venepuncture sites is well documented in EVD. Staff may become contaminated with blood, or NSI could occur. In our cohort, 152 needle venepunctures alone were avoided over the reporting period, with a concomitant possible reduction in both risk of NSI to the operator, and of pain and discomfort for the patients. It is accepted that our threshold for obtaining repeat blood samples may have been lower in patients with an indwelling CVC. Even if this were to be the case, however, more regular sampling leads to better, more individualised therapy with fluids and electrolytes—a key tenet of good EVD care.
Choice of access site, and timing
In this case series, the most frequently used access site was the subclavian vein. This reflects the training and clinical practice of the operators (two intensivists, one cardiologist). The EVDTU team assessed that this route had a number of advantages over internal jugular cannulation, particularly that patient tolerance might be improved, the line would not be affected by neck movement, and that the risk of accidental dislodgment might be reduced. However, there is no evidence to strongly support this, and operators should use the site with which they have most expertise. The potential for inadvertent subclavian artery puncture is noted, as is the slightly higher risk of pneumothorax, and for these reasons we do not endorse the subclavian site above other routes except in the hands of experienced operators. Ultrasound usage rates were relatively low, again reflecting the subclavian as the primary site, and that equipment movement around the EVDTU is often difficult [53]. In the heat of the day in West Africa, temperatures often exceed the operating limits of medical equipment, and this was noted to affect the ultrasound device batteries. Internal jugular access lends itself better to ultrasound guidance, but might be less well tolerated in the encephalopathic patient. Femoral access was avoided altogether, because of concerns regarding contamination due to high volume diarrhoea. Axillary vein access is an attractive option, as the site is more compressible in case of oozing or bleeding, but it requires functioning ultrasound for optimal success [54]. We also found ultrasound to be of value in selecting deep arm veins, where IV access was needed either prior to a diagnosis of EVD, or after CVC removal in patients with difficult venous access. This has been previously described in the literature [55, 56].
The timing of CVC insertion was deliberately chosen to enhance availability of the line during the patients’ peak illness, hence deferring until Stage 2. On review, we would not change this approach. The delay ensured that the CVC, in most cases, endured until the recovery phase, or in some cases until just prior to discharge. Deferring until later in the disease would result in CVC insertion in a more coagulopathic milieu, as evidenced by the progressive nature of the deterioration in ACT, APTT, PT and platelet counts outlined above. Also, deferring until a patient is sicker means a higher viraemia and thus presents more risk to the operator. As with all interventions in EVD patients, we advocate an “early and elective” approach to CVC placement in preference to “late and emergent” [38]. At the same time, we acknowledge that this strategy may not be an option in some EVD facilities, where the medical skill-mix, clinical caseload and reduced levels of equipment may render it unachievable.
Summary
We have demonstrated, for the first time in a military Ebola virus disease treatment unit, that a strategy of early central venous access is safe and feasible. Even in an austere clinical environment, with harsh environmental challenges, it is possible to provide central venous access which results in significant enhancements to clinical and nursing care of critically ill patients suffering from this deadly disease.
References
Baize S, Pannetier D, Oestereich L, Rieger T, Koivogui L, Magassouba N, Soropogui B, Sow MS, Keita S, De CH, Tiffany A, Dominguez G, Loua M, Traore A, Kolie M, Malano ER, Heleze E, Bocquin A, Mely S, Raoul H, Caro V, Cadar D, Gabriel M, Pahlmann M, Tappe D, Schmidt-Chanasit J, Impouma B, Diallo AK, Formenty P, Van HM, Gunther S (2014) Emergence of Zaire Ebola virus disease in Guinea. N Engl J Med 371:1418–1425
Editorial (2014) Ebola: a call to action. Nat Med 20:967
WHO Ebola Response Team (2014) Ebola virus disease in West Africa—the first 9 months of the epidemic and forward projections. N Engl J Med 371:1481–1495
Colebunders R, Borchert M (2000) Ebola haemorrhagic fever—a review. J Infect 40:16–20
Wauquier N, Becquart P, Padilla C, Baize S, Leroy EM (2010) Human fatal zaire ebola virus infection is associated with an aberrant innate immunity and with massive lymphocyte apoptosis. PLoS Negl Trop Dis 4:e837
Gatherer D (2014) The 2014 Ebola virus disease outbreak in West Africa. J Gen Virol 95:1619–1624
Tattevin P, Durante-Mangoni E, Massaquoi M (2014) Does this patient have Ebola virus disease? Intensive Care Med 40:1738–1741
Feldmann H, Geisbert TW (2011) Ebola haemorrhagic fever. Lancet 377:849–862
Nakayama E, Saijo M (2013) Animal models for Ebola and Marburg virus infections. Front Microbiol 4:267
Fletcher TE, Fowler RA, Beeching NJ (2014) Understanding organ dysfunction in Ebola virus disease. Intensive Care Med 40:1936–1939
Yazdanpanah Y, Arribas JR, Malvy D (2015) Treatment of Ebola virus disease. Intensive Care Med 41:115–117
Kortepeter MG, Bausch DG, Bray M (2011) Basic clinical and laboratory features of filoviral hemorrhagic fever. J Infect Dis 204(Suppl 3):S810–S816
Schieffelin JS, Shaffer JG, Goba A, Gbakie M, Gire SK, Colubri A, Sealfon RS, Kanneh L, Moigboi A, Momoh M, Fullah M, Moses LM, Brown BL, Andersen KG, Winnicki S, Schaffner SF, Park DJ, Yozwiak NL, Jiang PP, Kargbo D, Jalloh S, Fonnie M, Sinnah V, French I, Kovoma A, Kamara FK, Tucker V, Konuwa E, Sellu J, Mustapha I, Foday M, Yillah M, Kanneh F, Saffa S, Massally JL, Boisen ML, Branco LM, Vandi MA, Grant DS, Happi C, Gevao SM, Fletcher TE, Fowler RA, Bausch DG, Sabeti PC, Khan SH, Garry RF (2014) Clinical illness and outcomes in patients with Ebola in Sierra Leone. N Engl J Med 371:2092–2100
Hyde-Price C (2000) Under siege. An outbreak of the Ebola virus in Uganda has already taken its toll on nurses. Nurs Stand 15:20
Baron RC, McCormick JB, Zubeir OA (1983) Ebola virus disease in southern Sudan: hospital dissemination and intrafamilial spread. Bull World Health Organ 61:997–1003
Duffin C (2014) Ebola death toll rises in Africa with at least 14 nurses among the dead. Nurs Stand 28:9
Barry M, Traore FA, Sako FB, Kpamy DO, Bah EI, Poncin M, Keita S, Cisse M, Toure A (2014) Ebola outbreak in Conakry, Guinea: epidemiological, clinical, and outcome features. Med Mal Infect 44:491–494
Tomori O, Bertolli J, Rollin PE, Fleerackers Y, Guimard Y, De RA, Feldmann H, Burt F, Swanepoel R, Killian S, Khan AS, Tshioko K, Bwaka M, Ndambe R, Peters CJ, Ksiazek TG (1999) Serologic survey among hospital and health center workers during the Ebola hemorrhagic fever outbreak in Kikwit, Democratic Republic of the Congo, 1995. J Infect Dis 179(Suppl 1):S98–S101
Brett-Major DM, Jacob ST, Jacquerioz FA, Risi GF, Fischer WA, Kato Y, Houlihan CF, Crozier I, Bosa HK, Lawler JV, Adachi T, Hurley SK, Berry LE, Carlson JC, Button TC, McClellan SL, Shea BJ, Kuniyoshi GG, Ferri M, Murthy SG, Petrosillo N, Lamontagne F, Porembka DT, Schieffelin J, Rubinson L, O’Dempsey T, Donovan SM, Bausch DG, Fowler RA, Fletcher TE (2014) Being ready to treat Ebola virus disease patients. Am J Trop Med Hyg 92:233–227
Raabea VN, Borcherta M (2012) Infection control during filoviral hemorrhagic fever outbreaks. J Glob Infect Dis 4:69–74
Wichmann D, Schmiedel S, Kluge S (2015) Isolation in patients with Ebola virus disease. Intensive Care Med 41:511–513
Pasquier P, Ficko C, Merens A, Dubost C (2015) Preparing an ICU room to welcome a critically ill patient with Ebola virus disease. Intensive Care Med 41:118–119
Chan M (2014) Ebola virus disease in West Africa—no early end to the outbreak. N Engl J Med 371:1183–1185
Fauci AS (2014) Ebola—underscoring the global disparities in health care resources. N Engl J Med 371:1084–1086
Hawkes N (2014) Ebola outbreak is a public health emergency of international concern. WHO Warns BMJ 349:5089
Rees PSC, Ardley C, Bailey M, Dickson S, Fletcher T, Hinsley D, Lamb L, Nicholson-Roberts T (2015) Op GRITROCK: the Royal Navy supports defence efforts to tackle Ebola. J R Nav Med Serv 100(3):228–230
Kreuels B, Wichmann D, Emmerich P, Schmidt-Chanasit J, de HG, Kluge S, Sow A, Renne T, Gunther S, Lohse AW, Addo MM, Schmiedel S (2014) A case of severe Ebola virus infection complicated by gram-negative septicemia. N Engl J Med 371:2394–2401
Lyon GM, Mehta AK, Varkey JB, Brantly K, Plyler L, McElroy AK, Kraft CS, Towner JS, Spiropoulou C, Stroher U, Uyeki TM, Ribner BS (2014) Clinical care of two patients with Ebola virus disease in the United States. N Engl J Med 371:2402–2409
Antonelli M, Bonten M, Chastre J, Citerio G, Conti G, Curtis JR, De BD, Hedenstierna G, Joannidis M, Macrae D, Mancebo J, Maggiore SM, Mebazaa A, Preiser JC, Rocco P, Timsit JF, Wernerman J, Zhang H (2012) Year in review in Intensive Care Medicine 2011: I. Nephrology, epidemiology, nutrition and therapeutics, neurology, ethical and legal issues, experimentals. Intensive Care Med 38:192–209
Joannidis M, Metnitz PG (2005) Epidemiology and natural history of acute renal failure in the ICU. Crit Care Clin 21:239–249
Legrand M, Bezemer R, Kandil A, Demirci C, Payen D, Ince C (2011) The role of renal hypoperfusion in development of renal microcirculatory dysfunction in endotoxemic rats. Intensive Care Med 37:1534–1542
Boateng AA, Sriram K, Meguid MM, Crook M (2010) Refeeding syndrome: treatment considerations based on collective analysis of literature case reports. Nutrition 26:156–167
Marinella MA (2005) Refeeding syndrome and hypophosphatemia. J Intensive Care Med 20:155–159
West TE, von Saint Andre-von Arnim A (2014) Clinical presentation and management of severe ebola virus disease. Ann Am Thorac Soc 11:1341–1350
Lamontagne F, Clement C, Fletcher T, Jacob ST, Fischer WA, Fowler RA (2014) Doing today’s work superbly well–treating Ebola with current tools. N Engl J Med 371:1565–1566
Hockenhull JC, Dwan K, Boland A, Smith G, Bagust A, Dundar Y, Gamble C, McLeod C, Walley T, Dickson R (2008) The clinical effectiveness and cost-effectiveness of central venous catheters treated with anti-infective agents in preventing bloodstream infections: a systematic review and economic evaluation. Health Technol Assess 12:iii–xii
Antonelli M, Bonten M, Chastre J, Citerio G, Conti G, Curtis JR, De BD, Hedenstierna G, Joannidis M, Macrae D, Mancebo J, Maggiore SM, Mebazaa A, Preiser JC, Rocco P, Timsit JF, Wernerman J, Zhang H (2012) Year in review in Intensive Care Medicine 2011: III. ARDS and ECMO, weaning, mechanical ventilation, noninvasive ventilation, pediatrics and miscellanea. Intensive Care Med 38:542–556
Public Health Agency of Canada, Canadian Critical Care Society, Canadian Association of Emergency Physicians, The Association of Medical Microbiology and Infectious Diseases Canada (2014) Ebola clinical care guidelines. A guide for clinicians in Canada (interim report)
Bellomo R, Ronco C, Kellum JA, Mehta RL, Palevsky P (2004) Acute renal failure—definition, outcome measures, animal models, fluid therapy and information technology needs: the second international consensus conference of the acute dialysis quality initiative (ADQI) group. Crit Care 8:R204–R212
Volpicelli G (2011) Sonographic diagnosis of pneumothorax. Intensive Care Med 37:224–232
Xirouchaki N, Magkanas E, Vaporidi K, Kondili E, Plataki M, Patrianakos A, Akoumianaki E, Georgopoulos D (2011) Lung ultrasound in critically ill patients: comparison with bedside chest radiography. Intensive Care Med 37:1488–1493
Cholley BP, Vieillard-Baron A, Mebazaa A (2006) Echocardiography in the ICU: time for widespread use! Intensive Care Med 32:9–10
Expert Round Table on Ultrasound in ICU (2011) International expert statement on training standards for critical care ultrasonography. Intensive Care Med 37:1077–1083
Hutchings SD, Rees PSC (2013) Trauma resuscitation using echocardiography in a deployed military intensive care unit. J Intensive Care Soc 14(2):120–125
Simmons RS, Berdine GG, Seidenfeld JJ, Prihoda TJ, Harris GD, Smith JD, Gilbert TJ, Mota E, Johanson WG Jr (1987) Fluid balance and the adult respiratory distress syndrome. Am Rev Respir Dis 135:924–929
Kanji HD, McCallum J, Sirounis D, MacRedmond R, Moss R, Boyd JH (2014) Limited echocardiography-guided therapy in subacute shock is associated with change in management and improved outcomes. J Crit Care 29:700–705
Antonelli M, Bonten M, Chastre J, Citerio G, Conti G, Curtis JR, De BD, Hedenstierna G, Joannidis M, Macrae D, Mancebo J, Maggiore SM, Mebazaa A, Preiser JC, Rocco P, Timsit JF, Wernerman J, Zhang H (2012) Year in review in Intensive Care Medicine 2011. II. Cardiovascular, infections, pneumonia and sepsis, critical care organization and outcome, education, ultrasonography, metabolism and coagulation. Intensive Care Med 38:345–358
Shaw AD, Raghunathan K, Peyerl FW, Munson SH, Paluszkiewicz SM, Schermer CR (2014) Association between intravenous chloride load during resuscitation and in-hospital mortality among patients with SIRS. Intensive Care Med 40:1897–1905
Krajewski ML, Raghunathan K, Paluszkiewicz SM, Schermer CR, Shaw AD (2015) Meta-analysis of high- versus low-chloride content in perioperative and critical care fluid resuscitation. Br J Surg 102:24–36
O’Grady NP, Alexander M, Burns LA, Dellinger EP, Garland J, Heard SO, Lipsett PA, Masur H, Mermel LA, Pearson ML, Raad II, Randolph AG, Rupp ME, Saint S (2011) Summary of recommendations: guidelines for the prevention of intravascular catheter-related infections. Clin Infect Dis 52:1087–1099
Pratt RJ, Pellowe CM, Wilson JA, Loveday HP, Harper PJ, Jones SR, McDougall C, Wilcox MH (2007) Epic2: national evidence-based guidelines for preventing healthcare-associated infections in NHS hospitals in England. J Hosp Infect 65(Suppl 1):S1–S64
Kehoe A, Rees PSC (2006) Developments in pre-hospital care: is the specialty coming of age? J R Nav Med Serv 92:140–142
Moore CL (2014) Ultrasound first, second, and last for vascular access. J Ultrasound Med 33:1135–1142
O’Leary R, Ahmed SM, McLure H, Oram J, Mallick A, Bhambra B, Bodenham AR (2012) Ultrasound-guided infraclavicular axillary vein cannulation: a useful alternative to the internal jugular vein. Br J Anaesth 109:762–768
Meyer P, Cronier P, Rousseau H, Vicaut E, Choukroun G, Chergui K, Chevrel G, Maury E (2014) Difficult peripheral venous access: clinical evaluation of a catheter inserted with the Seldinger method under ultrasound guidance. J Crit Care 29:823–827
Egan G, Healy D, O’Neill H, Clarke-Moloney M, Grace PA, Walsh SR (2013) Ultrasound guidance for difficult peripheral venous access: systematic review and meta-analysis. Emerg Med J 30:521–526
Acknowledgments
The authors would like to acknowledge the support and hard work of all the nursing, biomedical science and support staff at the UK Defence Medical Service Ebola Virus Disease Treatment Unit, Kerry Town, Sierra Leone.
Conflicts of interest
The authors declare they have no conflicts of interest related to this paper.
Author information
Authors and Affiliations
Corresponding author
Additional information
Take home message: A strategy of early CVC insertion is safe and effective in Ebola patients. It allows multiple drug and electrolyte therapies to be safely delivered, and makes repeat blood sampling easier and safer.
Rights and permissions
About this article

Cite this article
Rees, P.S.C., Lamb, L.E.M., Nicholson-Roberts, T.C. et al. Safety and feasibility of a strategy of early central venous catheter insertion in a deployed UK military Ebola virus disease treatment unit. Intensive Care Med 41, 735–743 (2015). https://doi.org/10.1007/s00134-015-3736-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-015-3736-y