Article Text

Abstract
Introduction Prevention against head wounds from explosively propelled fragments is currently the Mark 7 general service combat helmet, although only limited evidence exists to define the coverage required for the helmet to adequately protect against such a threat. The Royal Centre for Defence Medicine was tasked by Defence Equipment and Support to provide a framework for determining the optimum coverage of future combat helmets in order to inform the VIRTUS procurement programme.
Method A systematic review of the literature was undertaken to identify potential solutions to three components felt necessary to define the ideal helmet coverage required for protection against explosively propelled fragments.
Results The brain and brainstem were identified as the structures requiring coverage by a helmet. No papers were identified that directly defined the margins of these structures to anatomical landmarks, nor how these could be related to helmet coverage.
Conclusions We recommend relating the margins of the brain to three identifiable anatomical landmarks (nasion, external auditory meatus and superior nuchal line), which can in turn be related to the coverage provided by the helmet. Early assessments using an anatomical mannequin indicate that the current helmet covers the majority of the brain and brainstem from projectiles with a horizontal trajectory but not from ones that originate from the ground. Protection from projectiles with ground-originating trajectories is reduced by helmets with increased stand-off from the skin. Future helmet coverage assessments should use a finite element numerical modelling approach with representative material properties assigned to intracranial anatomical structures to enable differences in projectile trajectory and helmet coverage to be objectively compared.
- NEUROPATHOLOGY
- ORAL & MAXILLOFACIAL SURGERY
Statistics from Altmetric.com
Key messages
-
The ideal coverage provided by a combat helmet should be defined as one that protects the brain and brainstem.
-
No papers defined the margins of these structures to anatomical landmarks nor how these could be related to helmet coverage.
-
We recommend relating the margins of the brain to the nasion, external auditory meatus and superior nuchal line.
-
The UK Mark 7 combat helmet covers the majority of the brain and brainstem from projectiles with a horizontal trajectory, but not from those that originate from the ground.
-
Future coverage assessments should use a finite element approach with representative material properties assigned to intracranial anatomical structures.
Introduction
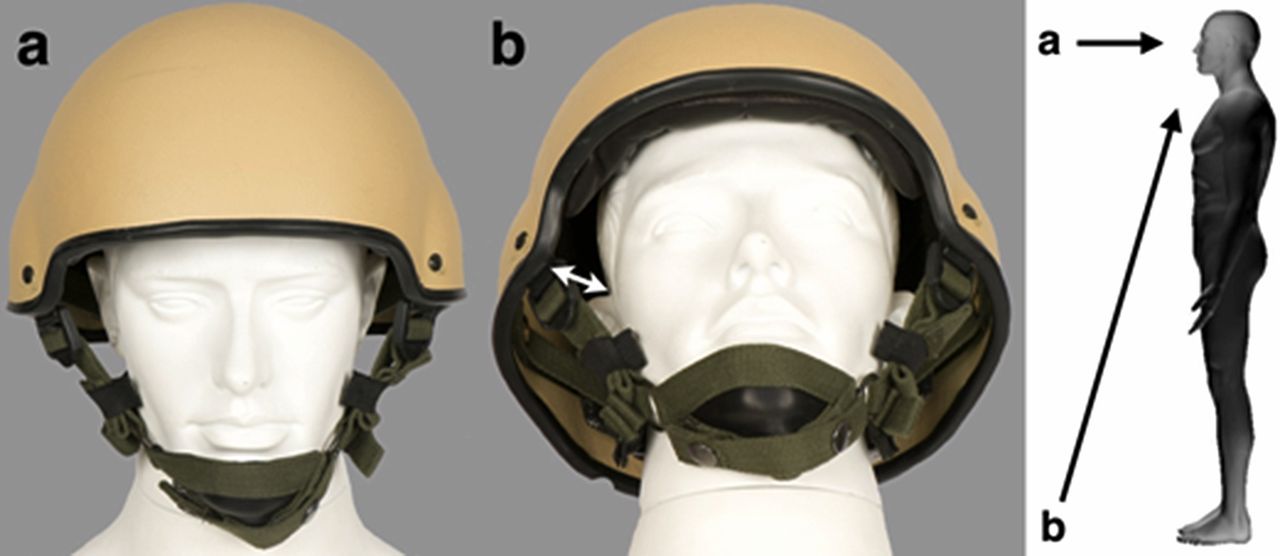
Penetrating head wounds are the most common cause of death experienced by both UK and US service personnel.1–,4 Head wounds are currently present in 15–19% of all combat wounds and are primarily due to penetrating explosive fragments.3 ,4 Prevention against such wounds for the individual soldier remains the combat helmet,5–9 in the form of the Mark 7 general service combat helmet issued to all UK service personnel deploying to Afghanistan (Figure 1). Although such helmets unquestionably provide substantial protection,1 ,5 ,6 ,8 finding objective evidence to quantify this effect is difficult because nowadays they are almost always worn by coalition soldiers at the time of injury.4 For example, the lower incidence of head wounds found in US forces compared against their Iraqi counterparts during Operation Desert Storm in 1991 has been ascribed to the greater use of helmets by the US cohort.2 However, without knowing if either the US or Iraqi soldiers were wearing a helmet at the time of injury, nor accurately knowing the mechanism of injury, true comparisons cannot be made. In fact until recently the only paper that ascribed numerical values to the effectiveness of helmets was from World War 1, where it was suggested that the introduction of helmets to US forces reduced the incidence of fatal head injuries from 25% to 14–22%.8 In an attempt to provide truly objective evidence for the effectiveness of personal protective equipment (PPE), including helmets, a prospective cohort trial has recently been completed on Op HERRICK in Afghanistan.10 This approach used a novel computerised surface wound mapping (SWM) tool to relate wound location to resultant injury, in combination with accurate knowledge of what PPE was worn at the time. Early results from the trial are already statistically significant, demonstrating that the odds of sustaining a head injury when wearing a helmet was 2.7 times lower than when not wearing one.10
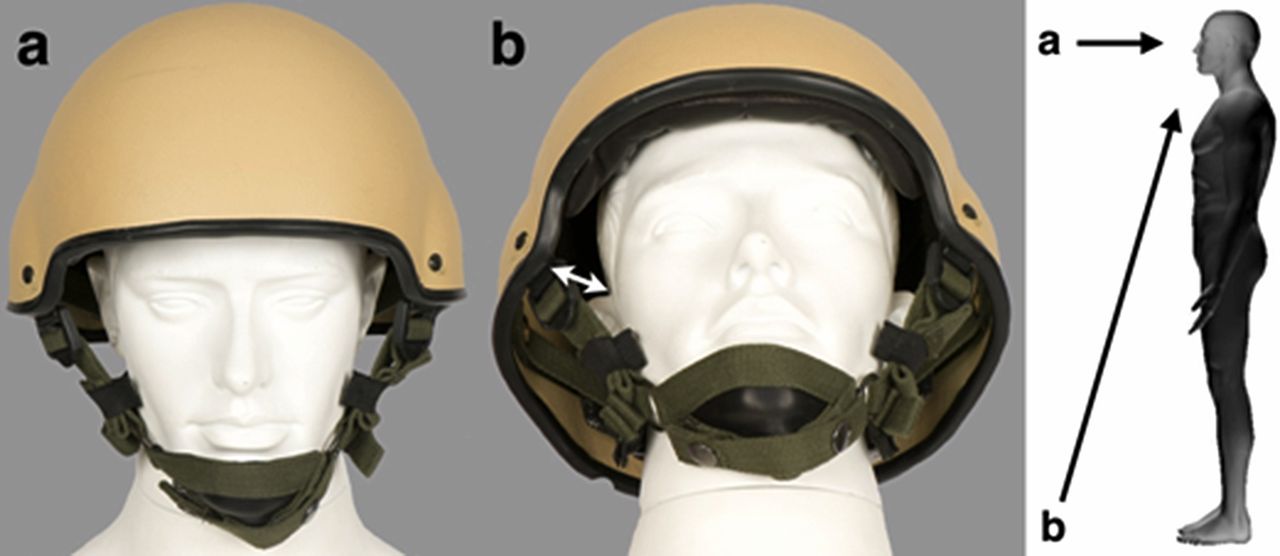
UK Mark 7 general service combat helmet demonstrating a horizontal trajectory (left) compared to a ground-originating trajectory (right). The white arrow demonstrates the distance between scalp and helmet (so-called ‘stand-off’).
The shape and design of the current Mark 7 combat helmet is a direct derivative of the first modern combat helmet, which was issued to soldiers in World War I to counter the effects of fragmenting explosive munitions.6 ,8 In addition to protecting against fragments, there is also now a requirement for bump protection which, in UK helmets, is achieved through a helmet suspension system. The US solution to bump protection is achieved using pads, which results in the distance between skin and helmet (so called ‘stand-off’, Figure 1B) being less compared to its UK equivalent (12 mm vs 25–31 mm11). It should also be noted that although combat helmets will also protect against some bullets from handguns,11 this is not a requirement for the UK helmet unlike its US equivalent.
The current VIRTUS procurement programme will define the Ministry of Defence's requirements for equipment to protect the future UK dismounted soldier, including replacing the current Mk 7 helmet. However, limited evidence to define the coverage required for the helmet to protect against perforating explosive fragments exists.1 Defence Equipment and Support (DE&S) tasked the Royal Centre for Defence Medicine (RCDM) and Cranfield University (home of the Defence Academy) to suggest a framework for determining the optimum coverage for a future combat helmet from a medical standpoint. Similar concepts developed recently by RCDM have been employed successfully by DE&S in the procurement of future neck protection.12 The aim of this paper is to identify potential solutions to three components felt necessary to define the ideal helmet coverage required for protection against explosively propelled fragments. Although bump protection is also a requirement, it was agreed that the coverage required for such protection would likely to be inherently included in the greater coverage required for fragmentation protection.
Method
A systematic review of the literature was undertaken using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) methodology.13 The following scientific databases were searched: PubMed, ProQuest, Web of Science, Google Scholar. An internet search was undertaken using Google, Internet Explorer and Firefox. Finally, three limited-access sources were interrogated: the defence online library, the Barrington digital library at Cranfield University and the Dstl Athena online library. The Barrington digital library now holds copies of the papers presented at previous Personal Armour Systems Symposia (PASS), a multinational conference dedicated to developments in PPE. Although the PASS conferences are freely open to all to attend, most of the papers presented are never published and have historically been impossible to search.
The following keywords were used in all searches; helmet, combat, military, ballistic, fragment, shape, coverage, outcome, head, death, mortality, morbidity, brain, brainstem, explosive. Only primary sources providing original experimental data were included and any identified in a non-English language were translated. The references from every article identified at this point were also hand searched and requested if not already done so. Information was divided into the following three components felt necessary to define the coverage provided by a helmet to protect against explosively propelled fragments:
-
What anatomical structures should ideally be covered by a combat helmet?
-
What surface landmarks could be used to determine the boundaries of the structures requiring protection?
-
How could these surface landmarks be related to the margins of a combat helmet thereby defining its coverage?
Results
A scientific database search identified 36 potential publications (28 papers and eight books) using these keywords (Figure 2). A further three papers were found through examining the references in these sources. Four papers were identified that required translation (French and Russian). Following screening, 10 papers1 ,2 ,5 ,7 ,11 ,14–18 and two books had pertinent information when analysed.6 ,8 An internet search identified 24 additional publications, only two of which had pertinent information to those three questions,9 ,19 and that had not been found in the database searching. The Barrington digital library identified three additional limited access publications,20–22 and five unpublished papers presented at previous PASS conferences.23–27 Although the keywords identified 28 publications in the Dstl Athena database and 11 publications in Defence intranet, respectively, none contained original information capable of answering any of the three questions and were therefore excluded. Civilian definitions of helmet coverage, such as the British Standards Institute,14 were also excluded as it was found on reading that the standard pertained to bump protection alone.

Results of systematic review to answer the three relevant questions.
What structures should ideally be covered by a combat helmet
Eight publications stated that the anatomical area of protection required for a combat helmet was the head6 ,14 ,20 ,23–27 but all failed to elaborate further.
What surface landmarks could be used to determine the boundaries of the structures requiring protection
Five publications described potential surface landmarks for sizing a combat helmet when issuing it to the soldier.6 ,9 ,20 ,21 ,23 Landmarks included the eyebrows,21 external ear or canal,21 ,23 occiput21 and glabella.21 However, with the exception of the external ear canal and the glabella, there was insufficient information in either paper to provide an accurate and reproducible anatomical landmark. Tobin and Iremonger6 and McManus et al20 both suggested that helmet coverage should be determined by drawing a line from under the chin to the bottom of the skull, but did not further define either landmark.
How could these surface landmarks be related to the margins of a combat helmet thereby defining its coverage
Only a single paper could be found that related surface landmarks to the coverage provided by a helmet.23 Eberius and Gillich23 described the ideal margin of the helmet as 12.7 mm above the eyebrow anteriorly and at the level of the ear canal laterally but did not provide a reason why these landmarks were chosen or how they related to the anatomical structures requiring protection.
Discussion
The aim of this paper was to identify potential solutions to three components felt necessary to define the ideal helmet coverage required for protection against explosively propelled fragments. The only publications that could be found that defined the anatomical area of protection required for a helmet stated that it should protect the head, and did not elaborate further.6 ,14 ,20 ,23–27 However, the term ‘head’ is broad in anatomical terms, and encompasses the brain, brainstem, skull vault, base of skull and scalp; it could also be possible to interpret it as including such anatomy as the facial soft tissues, facial bony skeleton, eyes and ears. Analysis of military papers describing head injuries would indicate that the primary structures demonstrated to be associated with poor outcomes, and thereby require protection, are the brain and brainstem.4 We would therefore recommend that the ideal coverage provided by a combat helmet be defined as one that protects these two structures, as opposed to the term ‘head’. It is also important to clarify that although the helmet is designed to protect the brain, it also provides protection to the top of the face and neck from projectiles with a horizontal trajectory. Similarly, the helmet is potentially not the only way to protect the brain and brainstem; for example, the anterior part of a helmet could be moved superiorly if a visor with similar ballistic protective properties was used in conjunction.
A number of surface landmarks have been described to enable a helmet to be sized correctly, including soft tissue and bony landmarks.6 ,9 ,20 ,21 ,23 However, the use of soft tissue landmarks, such the eyebrow, display considerable inherent variability between individuals.28 The use of bone landmarks should reduce such variability; such a system is used in orthognathic surgery and uses cephalometric points that can be identified on lateral plain radiographs.28 More helpfully, there is considerable population data available for cephalometric positions. Two easily identifiable cephalometric points on both radiology and by palpation are the nasion (the point of maximum depression between nose and forehead) anteriorly and the external auditory meatus laterally (Figure 3). Magnetic Resonance (MR) scans would suggest that these points are just below the most anterior and inferior extensions of the brain (Figure 4). The identification of a posterior bony landmark is more problematic, as no recognised cephalometric landmark exists and none is easy palpable. It has previously been suggested that the occiput21 be used, but we would argue that is not an easily identifiable single landmark in real life. Therefore, it is proposed that the superior nuchal line be used, as this can be felt as the point at which the trapezius muscle inserts into the occipital bone. Superimposition of this landmark onto a saggital MR scan would suggest this landmark is just below the most posterior and inferior extension of the brain and brainstem (Figure 4).

Sagital section through the skull demonstrating surface anthropometric landmarks to which the margins of the brain can be related. Arrow a=horizontal projectile path, Arrow b=ground originating projectile path.

Sagital magnetic resonance slice of brain demonstrating (1) nasion, (2) external auditory meatus (estimated position) and (3) superior nuchal line
To demonstrate the utility of our suggested technique we undertook a coverage assessment using an anatomical mannequin in conjunction with the current Mark 7 helmet (Figure 5). Such a mannequin was representative of a 50th percentile UK male soldier in terms of head circumference. The helmet was 15 mm above the nasion and 20 mm below the superior nuchal line. Interestingly the helmet was level with the external auditory meatus, which is identical to the lateral coverage provided by the US Advanced Combat Helmet (ACH) helmet, as described by Eberius and Gillich.23 The Mark 7 helmet covers the pterion, an area of inherent anatomical weakness where the skull vault is thinnest and the middle meningeal artery runs beneath.17 However, although the helmet covers the majority of brain and brainstem from projectiles with a horizontal trajectory (Figure 1A), coverage is significantly reduced for a projectile trajectory that originates from the ground (Figure 1B). This effect will be further potentiated by those helmets with increased stand-off, such as the UK Mark 7 helmet in comparison to the US ACH helmet.

UK Mark 7 general service combat helmet worn on an anatomical mannequin with surface anthropometric landmarks superimposed (1) nasion, (2) external auditory meatus and (3) superior nuchal line.
We recognise that such an approach still requires physical prototypes to be constructed, with resultant time and financial implications. It also assumes that the individual anatomical components of the head have equal vulnerability and susceptibility, without respect to the differing functions of its individual components. As part of a new finite element numerical approach to injury modelling, a mathematical anatomical mesh of a human body derived from CT scans has been recently procured.12 Currently, only the surface skin layer is being used for the purposes of SWM, enabling different types of PPE (including helmets) to be superimposed in the model (Figure 6). This anatomical mesh has also been scaled for a 50th percentile male UK soldier, but has the potential, if required, to be adjusted to fit the anthropometric data from different populations. The fidelity of the mesh can be increased to include internal anatomical structures, such as the brain or spinal cord, enabling differences in projectile trajectories and helmet coverage to be compared. The final step in the development of this numerical injury model would be to assign material properties to each individual anatomical structure and PPE component representative of that projectile passing through it. Such an approach is technically complex and requires experimental data that is difficult to obtain and in many cases does not yet exist29; however, early results simulating the penetration of fragment simulating projectiles into neck tissues has demonstrated the potential for such a model to predict the different potential injury mitigating effects of neck protection.12 We believe such an approach should be extrapolated to the head region to provide robust evidence for objectively comparing future helmet coverage.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
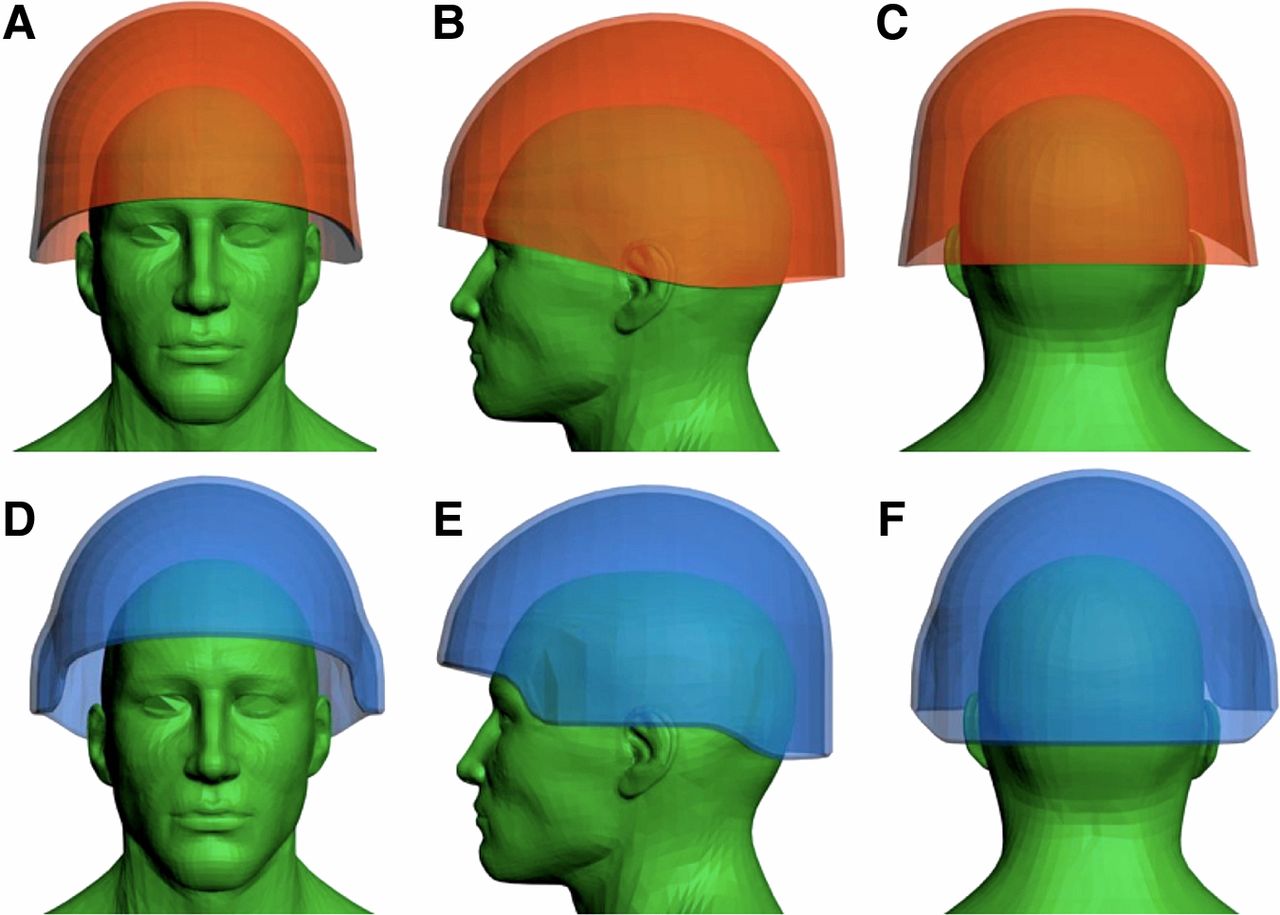
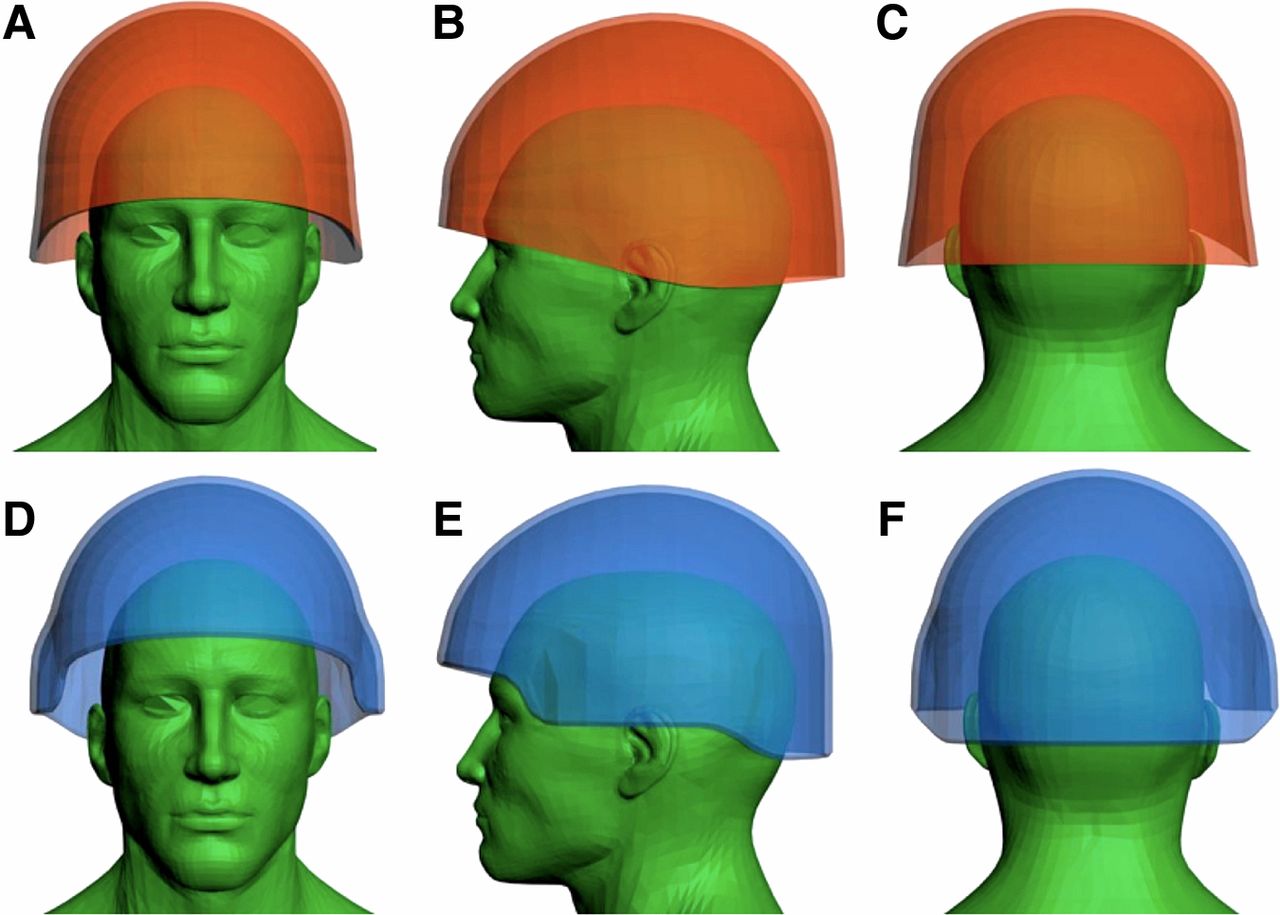
Computerised surface wound mapping demonstrating the similar overall head coverage produced by the Mark 6A (A–C) and Mark 7 (D–F) general service combat helmets, despite their differing shapes.
Conclusion
Despite the high mortality associated with head wounds from perforating explosive fragments, a paucity of evidence was found to justify the area of coverage provided by current combat helmets. The brain and brainstem were identified as the structures requiring coverage by a helmet, but no publications directly related the margins of these structures to surface landmarks nor to the coverage provided by a helmet. We would recommend relating the margins of the brain and helmet to the nasion, external auditory meatus and superior nuchal line. We believe that the use of an anatomical mannequin in conjunction with these cephalometric landmarks has demonstrated the potential utility of such an approach in the interim. However, future helmet coverage assessments should use a finite element numerical modelling approach with representative material properties assigned to intracranial anatomical structures to enable differences in projectile trajectory and helmet coverage to be objectively compared.
References
Footnotes
-
Contributors JB: guarantor of this work. JB: conceived of and designed the research study. JB and DC: searched the literature. JB, DB, DC and MJM: preparing and editing the manuscript.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.