Article Text

Abstract
Introduction Smoking is a major risk factor for chronic obstructive pulmonary disease (COPD). Serving military personnel have previously been shown to be more likely to smoke, and to smoke more heavily, than civilians, but there is no clear consensus as to whether in later life, as veterans, they experience a higher prevalence and mortality from COPD than do non-veterans. We examined the risk of COPD in Scottish veterans and assessed the impact of changes in military smoking.
Methods Retrospective 30-year cohort study of 56 205 veterans born 1945–1985, and 172 741 people with no record of military service, matched for age, sex and area of residence, using Cox proportional hazard models to examine the association between veteran status, birth cohort, length of service and risk of COPD resulting in hospitalisation or death.
Results There were 1966 (3.52%) cases of COPD meeting the definition in veterans, compared with 5434 (3.19%) in non-veterans. The difference was statistically significant (p=0.001) in the unadjusted model although it became non-significant after adjusting for deprivation. The highest risk was seen in the oldest (1945–1949) birth cohort and in veterans with the shortest service (Early Service Leavers). The risk was significantly reduced in veterans born from 1960, and in those with over 12 years' service.
Conclusions Our findings are consistent with falling rates of military smoking since the 1960s, and with the reduction in smoking with longer service. The oldest veterans, and those with the shortest service, are least likely to have benefited from this, as reflected in their higher risk for COPD.
- PUBLIC HEALTH
Statistics from Altmetric.com
Key messages
Serving UK military personnel are known to smoke more, and to smoke more heavily, than civilians.
This study found that the oldest UK veterans, and those with the shortest service (Early Service Leavers), were more likely than non-veterans to develop chronic obstructive pulmonary disease (COPD).
Veterans born after 1960 and those with the longest service demonstrated reduced risk compared with non-veterans.
The findings are consistent with the reported reduction in military smoking since the 1960s.
Healthcare providers should be alert to the increased risk of smoking-related diseases in older veterans, particularly if they were Early Service Leavers, and should be proactive in offering smoking cessation services.
Introduction
Chronic obstructive pulmonary disease (COPD) is a chronic, slowly progressive disorder of the lungs characterised by increased airways resistance, with chronic cough, breathlessness and wheezing.1 The changes are not fully reversible with treatment. Chronic bronchitis, emphysema and bronchial hyper-reactivity are components of the COPD picture but not all need to be present for the diagnosis to be made. COPD is the fourth most common cause of death worldwide, and its prevalence is increasing. The global pooled prevalence is estimated at 7.6%, or 9%–10% for those aged over 40 years.2 The most important causal factor is cigarette smoking, which is estimated to account for 90% of cases, and the adjusted relative risk of death from COPD for US male current smokers compared with never-smokers is 25.61 (95% CI 21.68 to 30.25) for the period 2000–2010.3 Severe childhood asthma is also a risk factor for adult COPD.4 Over 50 years of follow-up, there has been an absolute increase in COPD mortality in male smokers affecting all birth cohorts from 1900 to 1954.3
Serving military personnel have previously been shown to be more likely to smoke, and to smoke more heavily, than civilians. The prevalence of military smoking has reduced over time, although it has remained higher than in the civilian population.5 Possible reasons include the implementation of health-promotion policies initially introduced in the early 1960s6 and the introduction of mandatory fitness testing from the late 1970s, against a background of the falling prevalence of smoking in the general population. Veterans are also known to have a higher prevalence of smoking than civilians with no history of military service, and to smoke more heavily,7 but there is no clear consensus as to whether they experience a higher prevalence and mortality from COPD than do non-veterans in the longer term. The Scottish Veterans Health Study provided an opportunity to examine rates of COPD in a large cohort of military veterans, irrespective of length of service or exposure to combat, in comparison with civilians with no record of service, and to interpret the findings in relation to trends in military smoking.
Methods
Study population
The Scottish Veterans Health Study is a retrospective cohort study of all 56 570 military veterans resident in Scotland who were born between 1945 and 1985 and who were registered with the NHS Scotland both before and after service, and a comparison group of 172 753 individuals with no record of service matched 3:1 for age, sex and postcode sector of residence (mean population 5000). The study cohort and methods have been described elsewhere.8 Demographic data obtained from electronic NHS registration records were linked at an individual level to routine hospital admissions data (Scottish Morbidity Record SMR01) and death certificates to provide information on first recorded diagnosis of COPD and all-cause death. The electronic NHS record provided dates of entering and leaving the Service for veterans. The maximum period of follow-up was from 1 January 1981 (or date of leaving the Service, for veterans, if later) to 31 December 2012. Individual-level prescribing data were obtained from the NHS Prescribing Information System for a limited range of drugs, including nicotine replacement therapy. The data extract was pseudoanonymised, and approval for the study was granted by the Privacy Advisory Committee of the Information Services Division of NHS Scotland. Historical data on military smoking were obtained from published reports.
Socioeconomic status
In Scotland, there are 6505 datazones, based on postcode of residence, with a mean population of 800. The Scottish Index of Multiple Deprivation (SIMD) for each datazone is derived from information on housing, employment, income, health, education, crime and access to services.9 The SIMD has been used to derive quintiles of socioeconomic status (SES) for the Scottish population, ranging from 1 (most deprived) to 5 (least deprived). We used latest recorded postcode of residence to categorise the cohort participants according to these quintiles; for the veterans, this was post service.
Length of service
Length of service was stratified by common lengths of military engagement. Early Service Leavers (ESL) were defined as veterans who had served for 2.5 years or less. This is a tighter definition than the current minimum engagement of 4 years, but ensured exclusion of veterans who completed the 3-year minimum engagement which was previously in place.
Statistical methods
For the purposes of the study, a diagnosis of COPD was defined as International Classification of Diseases (ICD)-10 J40-J45 or ICD-9 490–496 (excluding 494 and 495) at any position in the record. A wide span of codes was included to allow for uncertainty in clinical coding. Cox proportional hazard models were used to examine the association between veteran status and cumulative risk of COPD, using age as the time-dependent variable, age at first record of COPD as the failure time and death (if no COPD) as the censor time. A landmark analysis was performed using age of 40 years as the starting point in order to exclude obstructive airways disease of constitutional origin, as far as practicable. HRs and p values were calculated, and the a priori rejection level was set at 0.05. Proportionality was tested using methodology based on Schoenfeld residuals.10 The models were run univariately and then repeated adjusting for the potential confounding effect of SES. The analyses were repeated stratifying by grouped year of birth to examine birth cohort effects, and stratifying by length of service. Cox proportional hazard models were used to compare case fatality within 1 and 5 years of a COPD diagnosis between veterans and non-veterans. All analyses were performed using Stata V.12.1 (1985–2011 StataCorp).
Results
After data cleansing, 56 205 (99.3%) veterans and 172 741 (99.9%) non-veterans were included in the analysis. Of the veterans included in the study, 5235 (9.2%) were women, reflecting the gender balance of the Service population. The mean period of follow-up was 29.3 years, and there was a total of 6.7 million person-years of follow-up among veterans and non-veterans combined.
There were 1966 (3.52%) cases of COPD resulting in hospitalisation or death in veterans during the period of follow-up, compared with 5434 (3.19%) cases in non-veterans. In the Cox proportional hazard model, the difference was statistically significant for all veterans, HR 1.09, 95% CIs 1.04 to 1.16, p=0.001, although it became non-significant after adjusting for SES (Table 1 and Figure 1).
Cox proportional hazards model of the association between veteran status and risk of COPD
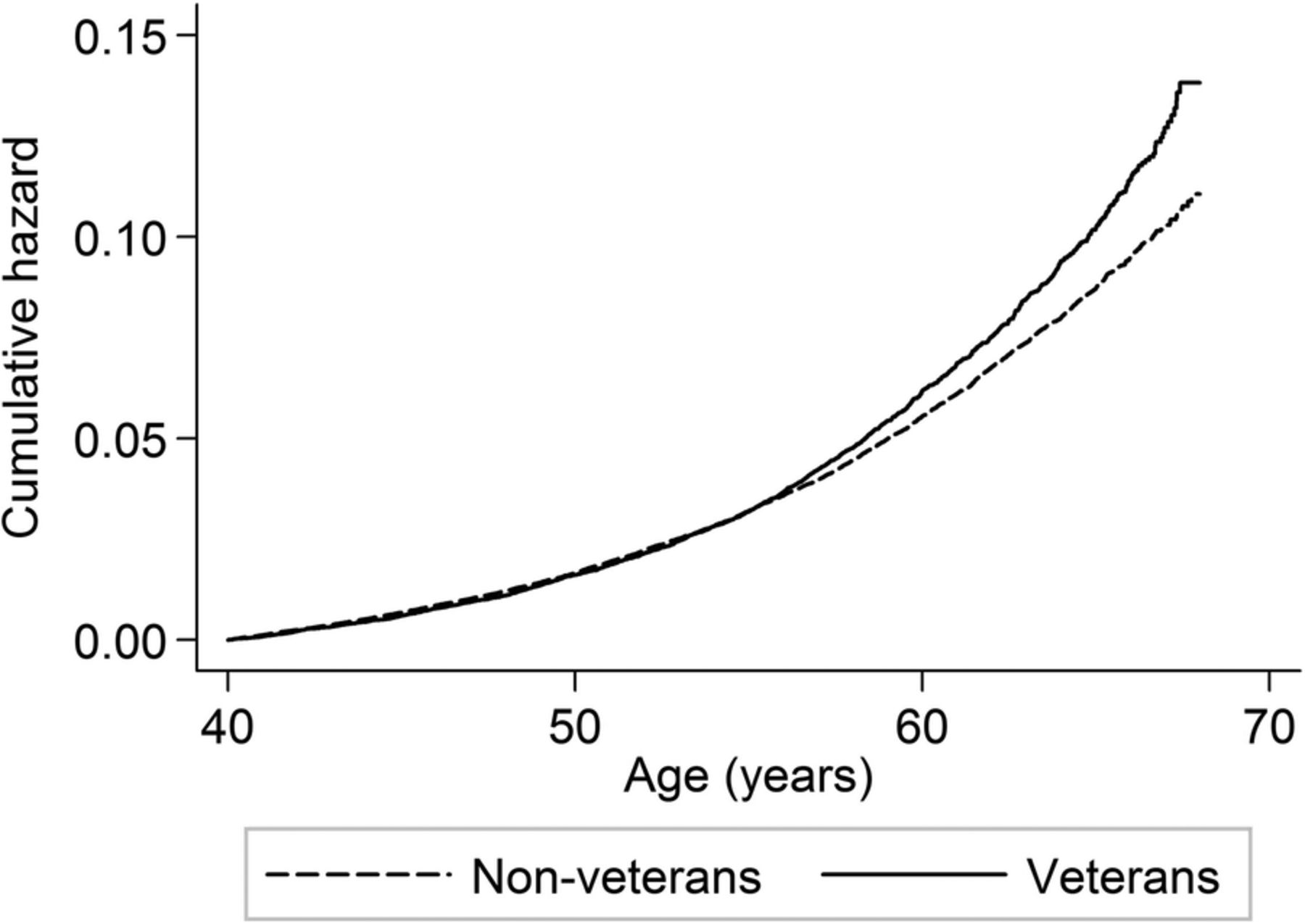
Nelson-Aalen plot of chronic obstructive pulmonary disease by veteran status.
The increase in risk was greatest for veterans born prior to 1955, adjusted HR 1.19, 95% CI 1.11 to 1.27, p<0.001. For veterans born from 1960 onwards, there was a statistically significant reduction in risk of COPD, adjusted HR 0.80, 95% CI 0.70 to 0.91, p<0.001. When analysed by birth cohort, there was a gradient from the earliest to the latest cohorts (Table 1 and Figure 2). Testing for non-proportionality of the hazards was non-significant for veterans over the age of 55 years (p=0.460); below this age, the risk of COPD was similar in veterans and non-veterans (Figure 1). In these oldest veterans, the HR was 1.28, 95% CI 1.18 to 1.39, p<0.001 unadjusted, and 1.22, 95% CI 1.13 to 1.32, p<0.001 after adjusting for SES.

{kind=link}
{kind=link}
HR for chronic obstructive pulmonary disease in veterans referent to non-veterans by birth cohort.
When analysed by length of service, the greatest increase in risk for veterans (adjusted HR 1.41, 95% CI 1.30 to 1.52, p<0.001) was seen in those with the shortest service (ESL). The increase in risk in ESL was confined to those born prior to 1960; for ESL born from 1960 onwards, their risk was unchanged from the wider population. The increase in risk diminished with longer service and was not significant, after adjusting for SES, beyond 4 years of service. For service in excess of 12 years, there was a statistically significant reduced risk of COPD compared with non-veterans in both the unadjusted and the adjusted models (Table 1).
One year case fatality after a diagnosis of COPD was higher in veterans than non-veterans: unadjusted HR 1.34, 95% CI 1.13 to 1.57, p=0.001. The difference persisted after adjusting for SES: HR 1.31, 95% CI 1.11 to 1.54, p=0.001. A similar difference was found for 5-year case fatality: HR 1.33, 95% CI 1.18 to 1.51, p<0.001 in the unadjusted model, and HR 1.31, 95% CI 1.15 to 1.48, p<0.001 after adjusting for SES.
Older veterans (born prior to 1960) were more likely than non-veterans to have received a prescription for nicotine replacement therapy: OR 1.31, 95% CI 1.14 to 1.51, p<0.001, while there was no statistically significant difference for veterans born from 1960: OR 1.03, 95% CI 0.82 to 1.27, p=0.818.
Discussion
Analysis of data from the Scottish Veterans Health Study demonstrated an increase in risk of COPD in veterans born prior to 1955 compared with non-veterans, although the difference was weaker after adjusting for deprivation. The increase in risk was greatest in those with the shortest length of service, particularly if they failed to complete the minimum engagement (ESL). For veterans born from 1960 onwards, there was a reduction in risk compared with non-veterans in those who served for longer than 3 years, which persisted after adjusting for deprivation. Older veterans were more likely to have received a prescription for nicotine replacement therapy than non-veterans, suggesting that they were more likely to be smokers. Veterans had a higher case fatality, which is likely to indicate greater severity of disease since case fatality rates for other conditions reported in the Scottish Veterans Health Study provide no evidence to suggest that veterans experience poorer outcomes which might indicate problems with access to healthcare.8
While the majority of cases of COPD are associated with tobacco smoking,1 a small number arise from genetic factors (α-1 antitrypsin deficiency),11 or environmental or occupational exposure such as atmospheric pollution and exposure to dusts.12 Military occupational health assessment precludes recruitment into service for those with symptomatic congenital disorders.13 Dust exposure is possible in the course of military operations in dry, dusty environments such as desert, but as service in these areas has increased from 1991 onwards, it is inconsistent with the pattern of reduction in risk of COPD observed in our study. The role of environmental tobacco smoke (ETS) in COPD is less well established, although an increased risk for both home and workplace exposure has been demonstrated.14 Military personnel have been described elsewhere as having been at risk of ETS exposure prior to the enforcement of smoke-free barrack rooms in 2006.8 Severe childhood asthma is associated with an increased risk of adult COPD, although mild intermittent asthma is not a risk factor.4 Recruits to the UK Armed Forces are required to meet stringent occupational health standards,15 which include freedom from ‘wheezing diatheses’ or a history thereof. A history of childhood wheeze is acceptable only if confined to the period prior to the age of 4 years, or a single episode in association with a respiratory tract infection after the age of 4 years but more than 4 years prior to application for enlistment.13 The exclusion of those with a history of severe childhood asthma from military service would be expected to introduce selection bias and should theoretically reduce the prevalence of COPD in veterans compared with the wider population, thus contributing to a ‘healthy worker effect’ in the veterans. However, any impact of the healthy worker effect in explaining the pattern of veterans' risk of COPD is overshadowed by the dominant aetiological role of smoking. Furthermore, since the healthy worker effect diminishes with time since first employment,16 it may be expected to show less impact on late-onset conditions such as COPD.
We are not aware of any other studies reporting COPD in British military veterans. A number of studies have examined the prevalence of COPD in veterans in other countries. In a large-scale study, data were examined for all patients attending a US Veterans Administration Medical Center (n=28 983) between 1999 and 2006, and 8.8% met the criteria for a diagnosis of COPD; the disease was diagnosed in 14.1% of the current smokers. The prevalence of current smoking in the veterans was 39%, and of the subjects with COPD, 54% were current smokers, both much higher than in the US population as a whole. However, the overall prevalence of COPD in the study population was similar to the prevalence in the general US population.17 A sharp increase in COPD mortality in US veterans between 1954 and 1976 has been described, although the increase was not as great as that experienced in the wider US population.18 By contrast, Australian veterans of the Vietnam War showed no difference in COPD mortality between 1966 and 2001 when compared with veterans whose only service was in Australia, or in comparison with the civilian population.19
Although formal records of Defence-wide military smoking cessation policy have not been located prior to 2001,20 Richards and Crowdy record that as early as 1962, ‘The Army Medical Services have recently started a programme of health education on smoking’, which provided the justification for their 12-year prospective study to examine changes in smoking prevalence in soldiers in the Army's junior units, in which school-leavers served in an educational and training capacity, from age 15 to 18 years, prior to moving into adult service.6 The results of the follow-up study provide an insight into the effectiveness of this early military health-promotion initiative. Successive cohorts of young soldiers were surveyed by age group in 1959, 1966 and 1971. Although there was only a 3% fall in the prevalence of current smoking in 15-year old soldiers between 1959 and 1971, the prevalence fell by 9% in 16-year old soldiers, 11% in 17-year old soldiers and 16% in 18-year old soldiers over the same period.21 It may be inferred that while the smoking habits of the newly joined 15-year old soldiers largely reflected those of the general population background from which they were drawn, exposure to health education in service had a progressively beneficial impact throughout the 3 years of junior service. In 1971, the prevalence of current smoking among serving 18-year old soldiers was 65.9%, compared with 82.3% in 1959 and 67.5% in 1966; by 1989, there had been a further fall in Army smoking to 41% (age standardised). Ex-smokers were most likely to cite fitness and health as a reason for quitting,22 suggesting a positive impact of the mandatory cardiorespiratory fitness testing programme which had been introduced in the late 1970s. It is likely that wider societal trends in smoking were also contributory, although military smoking remained higher.5 Smoking cessation support including brief intervention, nicotine replacement and pharmacological intervention is now routinely embedded in Defence Primary Care.23 More recent data have shown a smoking prevalence of 38.6% among 20–24-year old non-commissioned ranks in 2004, reduced from 43.7% 6 years earlier, but remaining higher than the overall general population rate of 36% for the same age group.24
Our results therefore suggest that the increased risk of COPD in older veterans is a consequence of the high rates of smoking by serving military personnel, especially in the 1960s and 1970s, which have been reported in a number of earlier studies.5 ,6 ,25 The results are also consistent with the increased risk of lung cancer and smoking-related cancer in older and shorter-serving veterans (especially if ESL), compared with non-veterans, which we have found in the Scottish Veterans Health Study,26 and with the increased risk of acute myocardial infarction in the same population which we attributed to higher rates of smoking.8 For all these conditions, the greatest increase in risk has been in veterans born prior to 1955, with a consistent pattern of decreased risk for those born from 1960 onwards, pointing to a progressive beneficial effect of the gradual reduction in military smoking which has been ongoing since the 1960s.5
Our finding of the greatest increase in risk of COPD in those with the shortest service is consistent with the reported observation that smoking habits are established early in military service.6 It is also consistent with decreasing rates of current smoking with increasing rank,22 the achievement of higher rank being linked to longer service. The positive association between never-smoking and higher rank is likely to be attributable in part to selection bias, including better education, in those who are more likely to succeed; a correlation has been demonstrated between smoking on enlistment, low educational attainment and deprivation.27 These factors may also therefore be associated with an increased likelihood of becoming ESL. The only relevant study to date, on a sample of only 80 ESL, has shown an association between ESL status and adverse childhood events, but was equivocal with respect to educational attainment,28 and further research would be needed to examine the association between smoking on enlistment, education and ESL status. The additional positive association between higher rank and being a former smoker22 may provide a pointer to the effectiveness of in-service military health-promotion activity in longer serving people who were smokers early in their service. We therefore conclude that those who left early at a time of high military smoking rates incurred the disadvantage of smoking initiation or recommencement as recruits, while not remaining in service long enough to benefit from military initiatives aimed at promotion of smoking cessation and fitness, and may have had little incentive to quit subsequently, as veterans.
The strengths and limitations of the present study are similar to those described elsewhere.8 A major strength was that it was based on a large cohort covering the whole of Scotland with 30 years follow-up. The diagnosis of COPD was taken from hospital admission and death records, and is therefore likely to be reliable in respect of those events occurring within Scotland. The use of record linkage to analyse individual-level data directly derived from health records allowed a robust cohort study design to be employed. The results were able to be matched or adjusted for potential confounders including sex and deprivation. It was possible to do subgroup analysis by sex, birth cohort and length of service.
Limitations of the study include possible loss to follow-up of subjects due to migration away from Scotland and the lack of any follow-up data prior to 1 January 1981. For those who are military veterans, we have not been able to link to in-service health or service records, and thus COPD occurring during service will not have been captured until the individual left the service and returned to NHS care, although since most veterans have left the Services by the age of 40 years, the landmark entry point will have minimised any loss of information. Since the clinical definition of COPD encompasses a range of respiratory conditions, not all of which need to be present, it was necessary to include a wide range of ICD codes. This may have resulted in the inclusion of some patients who did not meet the strict definition of COPD. Only the most severe end of the disease spectrum for COPD leads to hospital admission or death: as we had no access to primary care data, our results do not reflect overall disease incidence or prevalence. We have made the assumption that there are no systematic differences in the likelihood of admission between veterans and non-veterans other than the incidence and severity of disease, and that the relative magnitude of deaths and hospitalisations equates to the relative magnitude of total cases. Because the dataset was derived from demographic, vital record and hospital admissions data, no information was available on individual current or former smoking status, although we were able to use prescriptions for nicotine replacement therapy as a proxy measure for the relative likelihood of smoking.8 As our dataset was derived from NHS records and we were unable to link to Ministry of Defence records, we had no data on the Service to which a veteran belonged (Naval Service, Army or Royal Air Force) and were therefore unable to analyse whether there were differences between the three Services. Veterans with the Reserve service only could not be identified from NHS records and were therefore included among the non-veterans. This could have weakened the strength of association with military service.
We have demonstrated a complexity in the risk of COPD in veterans which may help to explain the lack of consensus observed in previous studies. The oldest members of the cohort were at increased risk compared with non-veterans, as were those with the shortest service, the risks diminishing with both year of birth and length of service. Since an improvement in lung function occurs after smoking cessation even in the presence of established disease,29 veterans who smoke should be encouraged to quit.
Conclusion
Older veterans are at increased risk of COPD compared with non-veterans. The difference is confined to those born prior to 1955, and younger veterans (born from 1960) have a reduced risk. The oldest veterans with the shortest service have the greatest increase in risk, while those who have served for more than 4 years exhibit a reduction in risk. Higher rates of smoking in older veterans and those with shortest service are likely to be an important risk factor, while more recently, military health promotion and fitness campaigns have been effective in reducing risk in younger veterans and in those who serve for longer. Healthcare providers should be alert to the increased risk faced by older veterans, especially if they left service prematurely (ESL), and should target smoking cessation in this at-risk group.
Acknowledgments
The authors thank the NHS Central Registry (NHSCR) and the Information Services Division, NHS Scotland (ISD) for extracting and linking the dataset.
References
Footnotes
Contributors BPB conceived the idea and designed the study, with advice from JPP and DFM. BPB carried out the data analysis, which was overseen by DFM, and interpreted the findings. BPB wrote the first draft of the report, which was critically reviewed and edited by all authors. BPB revised the draft following review, and all authors approved the final article.
Competing interests None declared.
Ethics approval Privacy Advisory Committee, NHS Scotland.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The Scottish Veterans Health Study remains in progress, and the data are not currently available.