Article Text

Abstract
Introduction Modern body armour clearly reduces injury incidence and severity, but evidence to actually objectively demonstrate this effect is scarce. Although the Joint Theatre Trauma Registry (JTTR) alone cannot relate injury pattern to body armour coverage, the addition of computerised Surface Wound Mapping (SWM) may enable this utility.
Method Surface wound locations of all UK and NATO coalition soldiers, Afghan National Army and Police and local nationals injured by explosively propelled fragments and treated in the Role 3 UK-led Field Hospital in Camp Bastion, Afghanistan, between 8 July and 20 October 2012 were prospectively recorded. The Abbreviated Injury Scores (AIS) and relative risk of casualties sustaining injuries under a type of body armour were compared with those that did not wear that armour.
Results Casualties wearing a combat helmet were 2.7 times less likely to sustain a fragmentation wound to the head than those that were unprotected (mean AIS of 2.9 compared with 4.1). Casualties wearing a body armour vest were 4.1 times less likely to sustain a fragmentation wound to the chest or abdomen than those that were unprotected (mean AIS of 2.9 compared with 3.9). Casualties wearing pelvic protection were 10 times less likely to sustain a fragmentation wound to the pelvis compared with those that were unprotected (mean AIS of 3.4 compared with 3.9).
Discussion Computerised SWM has objectively demonstrated the ability of body armour worn on current operations in Afghanistan to reduce wound incidence and severity. We recognise this technique is limited in that it only records the surface wound location and may be specific to this conflict. However, gathering electronic SWM at the same time as recording injuries for the JTTR was simple, required little extra time and therefore we would recommend its collection during future conflicts.
- FORENSIC MEDICINE
- ORAL & MAXILLOFACIAL SURGERY
- TRAUMA MANAGEMENT
- body armour
- combat helmet
Statistics from Altmetric.com
Key messages
-
Although modern body armour unquestionably prevents many injuries, evidence to actually objectively demonstrate its effectiveness is scarce.
-
A novel electronic three-dimensional wound mapping programme has been developed to be used prospectively at the patient's bedside.
-
Wound locations can be related to body armour coverage and injury outcome linked through the Joint Theatre Trauma Registry.
-
This pilot trial has objectively demonstrated the ability of body armour worn on current operations in Afghanistan to reduce wound incidence and severity.
-
We would recommend this method for collecting wound mapping data and relating it to injury outcome for future conflicts.
Introduction
The ability to accurately compare between body armour designs remains one of the key strategic priorities for Defence Equipment and Support within the UK Ministry of Defence (MoD). However, objective evidence demonstrating the effectiveness of different armour designs in the literature is rare. Some publications suggesting the effectiveness of ballistic eye protection, for example,1–3 have not compared equal cohorts nor known the actual uptake of the protection itself and therefore care must be taken in their interpretation. Information used in the UK to date has generally pertained to early attempts at paper-based surface wound mapping (SWM)4 ,5 and the use of injury models such as the MAVKILL tool.6 Although it is possible that further unpublished restricted information does exist, a recent search by the lead author using the Dstl ATHENA database, the restricted MoD library and the Barrington library at the Defence Academy based at Cranfield university could not find any additional unpublished objective information on the subject.
Ideally one type of armour would be prospectively compared with another, with users blinded to the differences in a method analogous to a pharmaceutical drug trial. However, not only would this be impractical to achieve as most differences in design would likely be obvious to the user, for understandable reasons such a trial would be unlikely to obtain ethical approval and would have to be immediately stopped should such differences be shown. Two methods of practically comparing the potential effectiveness of different types of body armour therefore currently exist; the first is SWM linked to outcome through Joint Theatre Trauma Registry (JTTR) and the second is an injury model. Injury models such as the aforementioned MAVKILL and its replacement the Weapon Target Interaction (WTI) programme6 continue to increase in fidelity. However, injury models even to this day are most effective in making comparisons between armour types and care has to be taken in interpreting the injuries themselves that are predicted.
SWM is the process by which the entry wound locations of projectiles perforating the skin are recorded graphically.4 ,5 The key advantage of it over a computerised injury model is that it is based upon known injury outcomes and not just a theoretical output. SWM has been attempted intermittently by US and Israeli forces since World War I,7–9 with the most comprehensive results undertaken by the USA in Korea at the same time as the introduction of the ballistic nylon fragmentation vests to infantry soldiers.10 However, all of these studies were limited in that although they demonstrated the distribution of surface wounds, they did not relate them to the body armour worn at the time of injury. The USA is believed to currently have a SWM capability9 specifically designed to enable recommendations on body armour, but to our knowledge no reports of its results have ever been externally published.
SWM was not attempted by UK forces until as late as 2010 and has to date only focused specifically on face4 and neck5 wounds. Although both UK papers were able to make recommendations on body armour coverage, the authors acknowledged significant limitations that would be needed to be overcome for such an approach to progress further. Data collection used individual paper mapping templates, which could not be linked directly to the UK JTTR, the primary database providing epidemiological information on the types of injuries sustained by UK service personnel. Separate templates had to be constructed for each body armour design with the direction of threat being limited to that from a horizontal plane. In addition, all SWM information was collected retrospectively, meaning that the type of body armour was often not known and that wound entry locations were only available for those evacuated or repatriated to the UK, where notes or images would allow.
In an attempt to overcome previous limitations in data capture, a novel electronic three-dimensional SWM programme designated IMAP (Interactive Mapping Analysis Platform) has been developed in conjunction with RiskAware Ltd (Bristol, UK). This was designed to be used prospectively at the patient's bedside and to link in with the JTTR. IMAP has been built using dimensions based on an anthropometrically accurate 50th centile UK male service person and allows the geometries of any type of body armour to be imported in a computer-aided design format. The aim of this study was to undertake a prospective trial of SWM using the IMAP tool in order to demonstrate its potential utility in validating existing body armour coverage and in understanding the potential of protection to reduce injury occurrence or severity.
Method
The IMAP tool was loaded onto a laptop and set up in the Role 3 UK-led Field Hospital in Camp Bastion, Afghanistan. Wound entry locations were prospectively recorded on all UK soldiers, NATO coalition soldiers (US, Georgian and Danish during this period), Afghan National Army (ANA), Afghan National Police (ANP), Afghan Local Police (ALP) and Local National civilians (LN), sustaining penetrating wounds from explosively propelled fragmentation between 8 July and 20 October 2012. Paediatric patients were excluded from the analysis. For security reasons to enable external publication, the wearing of types of body armour by UK soldiers and NATO coalition soldiers will be grouped together. Explosively propelled fragments were derived from the following sources during this period: improvised explosive devices, rocket propelled grenades, mines and mortars. However, again for security reasons to enable external publication, all types of fragmentation will be grouped together in the analysis. Within this particular iteration of the IMAP programme, the following pictorial descriptions were used: red dots signified an individual explosive propelled fragment that was large enough to be identified surgically and excised; blue triangles indicated the location of smaller fragments seen either clinically or radiologically that were either not excised or were removed by scrubbing of the wound at the beginning of the operation. A green disc signified the site of a limb amputation (ie, a limb that was either traumatically amputated by the force of the injury mechanism or later removed by surgical intervention). The IMAP programme inherently cannot differentiate between the severity of wounds, either by their size, depth or underlying structures damaged. The wound mapping point was placed at the centre of where the surgeon felt the entry point would have been. For linear wounds in which a central point could not be determined, two corresponding points in IMAP were placed reflecting ends of the wound.
Body armour was recorded as the wearing of a combat helmet, body armour vest, tier 1 and tier 2 pelvic protection. In this analysis, the term tier 1 pelvic protection was used to describe underwear designed to be worn beneath trousers that has been reinforced with ballistic protective material. Tier 2 pelvic protection is designed to be worn over the trousers and is worn in conjunction with tier 111 to provide additional protection. Examples of the types of body armour worn by UK soldiers and their NATO counterparts during this period are demonstrated in Figure 1. The effect of wearing specific types of body armour on the incidence of injuries to areas covered by that type of PPE and the mean Abbreviated Injury Severity (AIS) scores associated with these injuries was determined. The OR was calculated for those wearing body armour sustaining an injury to that body area that it is designed to protect compared with those that were not wearing body armour to protect it. The version of IMAP used in this analysis did not have an inherent analytical capability necessitating these calculations to be made manually each time the type of body armour worn or the casualty cohort to be analysed changed.

Types of body armour worn by UK soldiers during the period covered by this study; (A) low-impact sunglasses, (B) medium impact goggles, (C) Mark IV OSPREY body armour vest, (D) Mark 7 general service combat helmet, (E) tier 2 pelvic protection and (F) tier 1 pelvic protection.
Results
SWM was undertaken on a total of 174 casualties who entered the field hospital during the time of this study following injury by explosively propelled fragmentation (Table 1). These were immediately entered into the IMAP tool and the wound location in relation to the body armour worn immediately checked. For security reasons, the positions of the items of body armour in relation to entry locations and outcomes are not displayed in this paper.
Cause of injuries to personnel whose wounds were mapped during this period; UK and NATO coalition soldiers, Afghan National Army (ANA), Afghan National Police (ANP), Afghan Local Police (ALP) and Local National civilians (LN)
Effect of combat helmet use on head wound incidence
Overall, 51/54 (94%) of UK and NATO coalition soldiers injured by explosively propelled fragments were believed to have been wearing a combat helmet at the time of injury. No PPE to protect the head was reported to have been worn by the casualty at the time of injury by the remaining cohorts. Table 2 details the distribution of head injuries with regard to helmet wearing; the manual calculation of risk ratios shows that 8/67 (0.12) soldiers wearing a helmet sustained a head wound and 59/67 (0.88) wearing a helmet did not. In comparison, 29/107 (0.27) soldiers not wearing a helmet sustained a head wound and 78/107 (0.73) not wearing a helmet sustained no head wound. The odds of sustaining a wound that perforated the skin or scalp potentially covered by a helmet was 0.12/0.88 (0.14) in those wearing a combat helmet compared with 0.27/0.73 (0.37) in those that did not (Table 2). The resultant OR highlights those wearing a helmet were 0.37/0.14 (2.7) times less likely to sustain a fragmentation wound to the head than those that were unprotected. The mean AIS score of the head injuries in those wearing a combat helmet was 2.9 compared with 4.1 in those that were unprotected. The visual representation of the effect of the combat helmet in reducing head injury is presented in Figure 2.
Incidences of patients sustaining head wounds in those wearing a combat helmet versus those that were unprotected and ORs

Interactive Mapping Analysis Platform demonstrating entry wound locations for those casualties sustaining face and head wounds only: (A) wearing a combat helmet; (B) unprotected casualties.
Effect of body armour vest use on thoracoabdominal wound incidence
All 54 UK and NATO coalition personnel included in this analysis were believed to have been wearing a fragmentation vest at the time of injury. The odds of sustaining a chest or abdominal wound (Table 3) was 0.07/0.93 (0.08) in those wearing a body armour vest compared with 0.24/0.76 (0.32) in those that were unprotected. Therefore, those wearing a vest were 0.32/0.08 (4.1) times less likely to sustain a fragmentation wound to the chest or abdomen than those that were unprotected. The mean AIS score in those wearing a vest was 2.9 compared with 3.9 in those that were unprotected. The visual representation of the effect of the body armour vest in reducing thoracoabdominal injury is presented in Figure 3.
Incidences of casualties sustaining chest or abdominal wounds in those wearing a body armour vest versus those that were unprotected

Interactive Mapping Analysis Platform demonstrating entry wound locations for all casualties within this study: (A) wearing body armour vest; (B) unprotected casualties.
Effect of pelvic protection on pelvic wound incidence
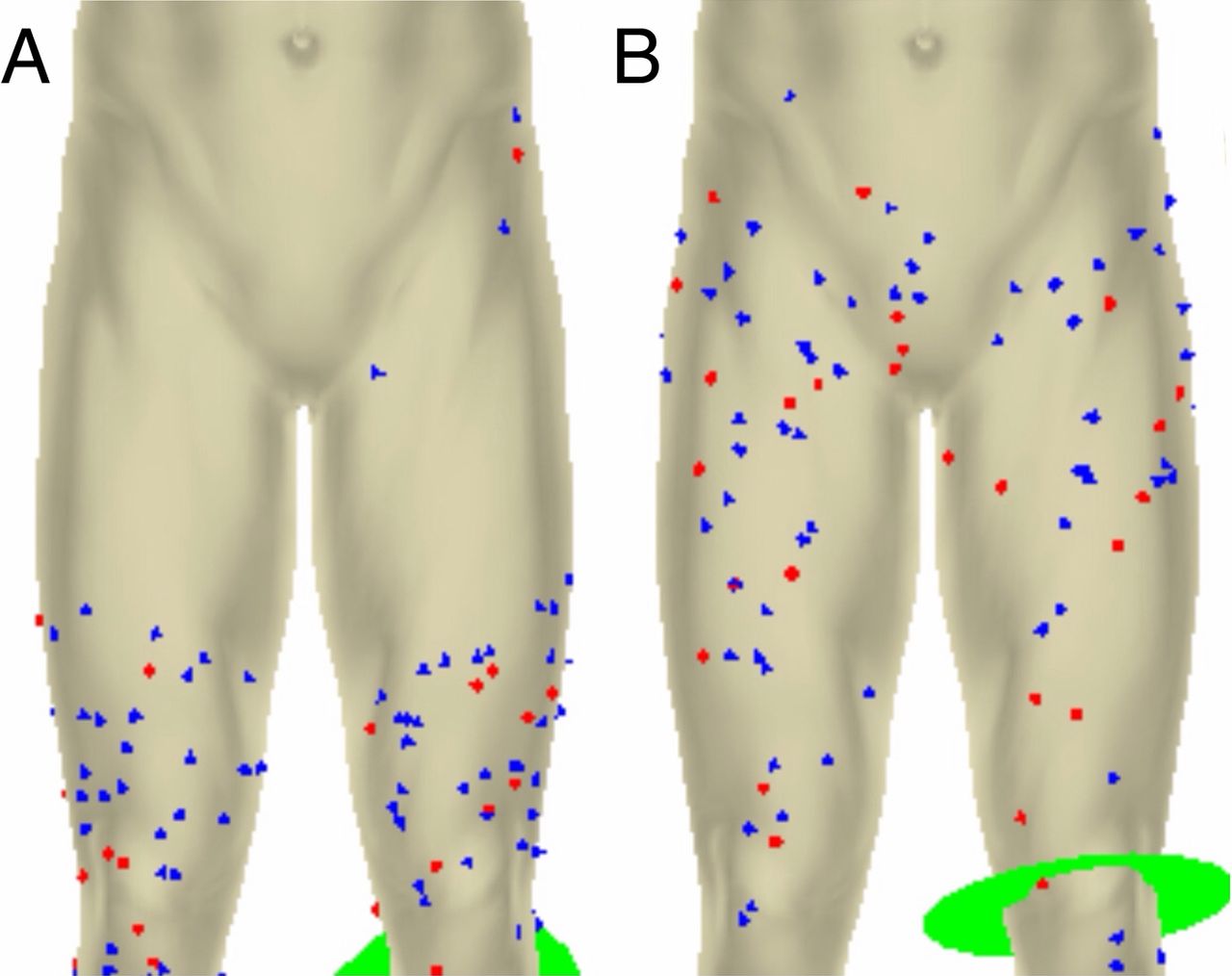
In total, 39/54 (72%) of UK and NATO coalition soldiers injured by explosive fragmentation during this period were believed to have been wearing pelvic protection analogous to either tier 1 or 2 at the time of injury. Only UK service personnel wore tier 2 pelvic protection. The odds of sustaining a pelvic wound (Table 4) defined as occurring within the area of skin coverage provided by tier 1 pelvic protection was 0.16/0.84 (0.19) in those wearing tier 1 alone, 0.15/0.85 (0.18) in those wearing tiers 1+2 and 0.64/0.36 (1.81) in those wearing no protection. Therefore, those wearing tier 1 alone were 9.5 times less likely, and both tiers 1+2 were 10.1 times less likely, to sustain a fragmentation wound to the pelvis compared with those that were unprotected. The mean AIS score for groin and pelvis injuries sustained by those wearing tier 1 alone was 3.5, for those wearing tiers 1+2 was 3.4 and 3.9 in those wearing no protection at all. A pictorial representation of the effect of pelvic protection on reducing the incidence of wounds to the pelvis is demonstrated in Figure 4.
Incidences of patients sustaining pelvic injury in those wearing pelvic protection versus those that were unprotected

Interactive Mapping Analysis Platform demonstrating entry wound locations in casualties wounded in either the leg or pelvic regions: (A) wearing pelvic protection (tier 1 or 2); (B) unprotected casualties.
Discussion
The aim of this study was to undertake a prospective trial of SWM using the IMAP tool in order to demonstrate its potential utility in validating existing PPE coverage and in understanding the potential of protection to reduce injury occurrence or severity. The trial clearly demonstrated the effectiveness of combat helmets, body armour vests and pelvic protection in decreasing wound incidence and severity. Although this pilot trial demonstrated no additional benefit from wearing tier 2 in addition to tier 1, this is likely to reflect the low numbers of casualties mapped in the analysis and we believe that the additional benefit of tier 2 protection would be expected to be demonstrated in a larger study. Computerised SWM using the IMAP tool was quick, and it was easy to collect wound entry locations if performed at the same time as collecting injury information for JTTR. This ease of data collection will in turn be increased when the slimmed down version of IMAP that uses a touch screen tablet computer is introduced in 2014.
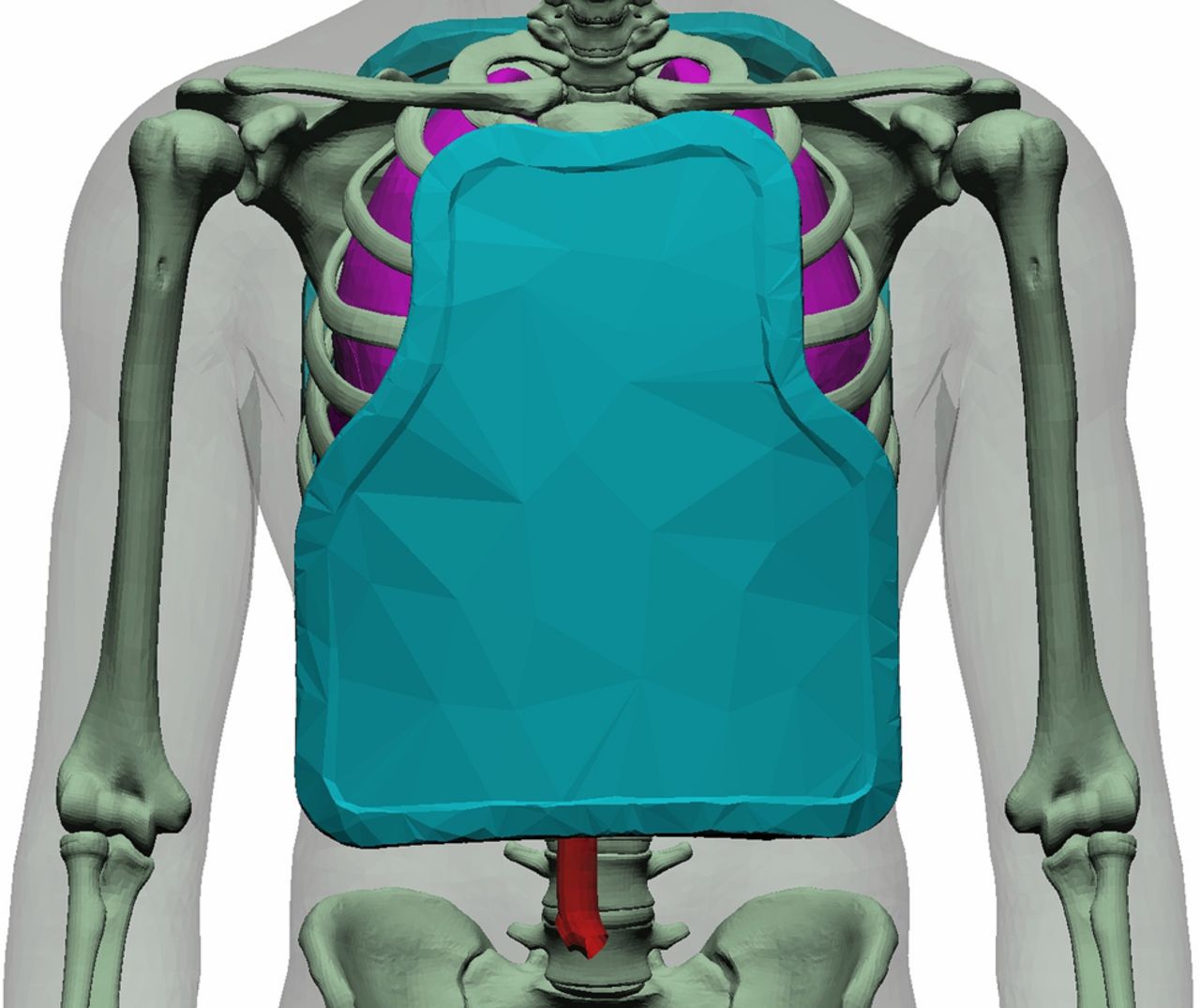
We recognise that there are a number of limitations with SWM that inherently cannot be overcome. We accept that by grouping ANP and civilians together for security reasons it may not reflect that each may have been exposed to different threats. The use of outcome data for a particular conflict may make any conclusions made using SWM specific for that conflict. For example, SWM has been instrumental in the development of a modified OSPREY neck collar for the Afghanistan conflict, but this may not be appropriate for the VIRTUS procurement programme that aims to provide protection for the UK soldier in future conflicts. Currently, the IMAP programme uses anthropometric measurements scaled to a 50th centile male with body armour overlays scaled to fit that; ideally the model will in the future have the ability to be adjusted to body measurements and armour sizes specific to the casualty being mapped. Finally, SWM can only record the surface entry wound location, although the anatomical human model used within both IMAP and injury models being developed within WTI now have the capability to accurately represent the underlying anatomy. A recent report has described how WTI is now being used to demonstrate ideal thoracoabdominal organ coverage and provide objective comparisons between hard armour ceramic plates for VIRTUS (Figure 5)12; when used in conjunction with surface anthropometric landmarks to define the boundaries of those thoracoabdominal structures requiring protection and three-dimensional printing of prototype ceramic materials, this has the potential to produce individualised ceramic body armour plates for every shape and size of UK soldier.13

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The Coverage of Armour Tool within the Weapon Target Interaction programme being used to demonstrate anatomical coverage provided by an OSPREY ballistic ceramic plate.
Conclusions
This pilot trial has objectively demonstrated the ability of body armour worn on current operations in Afghanistan to reduce wound incidence and severity. We recognise that computerised SWM is inherently limited in that it only records the surface wound location and may be specific to the conflict from which the data are collected. However, gathering SWM at the same time as recording injuries for the JTTR was simple, required little extra time and therefore we would recommend its collection during future conflicts.
Acknowledgments
This paper was also published with the permission of Joint Medical Command and the Defence Science and Technology Laboratory on behalf of the Controller of HMSO. The authors would like to thank Major Chris Birkby for her invaluable assistance in gathering some of the data on which this paper is based.
Footnotes
-
Contributors Design: JB and LAB. Literature review: JB. Manuscript preparation: JB, LAB, AEH and MJM.
-
Competing interests None.
-
Ethics approval This research was approved by the Defence Medical Services Research and Ethics committee and all patient data have been anonymised.
-
Provenance and peer review Not commissioned; externally peer reviewed.