Article Text

Abstract
Background Detailed knowledge of the likely volume and nature of the diseases presenting to deployed secondary care facilities aids operational planning. Now the British operation in Afghanistan has ended and a record of the experience is useful to preserve the lessons learned.
Methods Over a 2-year period from April 2011, prospective demographic and clinical data were collected on consecutive general internal medicine admissions to the Role 3 Hospital in Camp Bastion, Afghanistan. Up to four different symptoms and diagnoses were coded using the WHO International Classification of Disease, V.10 for each patient.
Results A total of 1368 medical patients were admitted. Of 1131 military admissions, 612 were from the UK (54.1%) and the remainder from 13 allied countries; 237 civilians came from 23 countries. Civilians were older than the military patients (p<0.001) but included five children. The 20 most frequent presenting symptoms were identified and there were 1626 diagnoses made. The 10 most frequent diagnoses were infectious gastroenteritis (12.6%), heat illness (4.3%), pneumonia (3.6%), epilepsy (2.6%), cellulitis (2.7%), migraine (1.8%), peptic ulcer disease (1.2%), myocardial infarction (1.2%), venous thromboembolism (1.2%) and pericarditis (0.7%). In 252 cases (18.4%) a firm diagnosis was not reached and a symptom was recorded. The five most frequent of these were undifferentiated febrile illnesses (4.6%), syncope (3.7%), chest pain (2.8%), headache (0.8%) and palpitations (0.7%). The mean hospital length of stay was 1.59 days and 72.2% of UK military patients were ‘returned to unit’. Three civilian patients died in hospital or following aeromedical evacuation and there were no deaths of any military patients.
Discussion This study demonstrates the wide variety of presentations seen by physicians at an established military field hospital. This information informs the core syllabus of military physician training and will help facilitate planning for future medical support to similar military operations.
Trial registration number RCDM/Res/Audit/1036/ 12/0305.
- INTERNAL MEDICINE
- INFECTIOUS DISEASES
Statistics from Altmetric.com
Key messages
General internal medicine admissions at the Role 3 Hospital accounted for a fifth of all hospital admission.
The majority of symptoms and diagnoses were due to a small group of diseases.
The remaining admissions consisted of uncommon diseases and presentations.
This paper supports breadth in the provision of physician training and in the diagnostic tests available in the operational environment.
Introduction
Throughout history, the majority of war casualties have been the result of disease or environmental factors.1 William Osler observed that dysentery was ‘more fatal to armies than powder or shot’.2 Accordingly, the military narrative has been shaped as often by disease as by great leadership or technical innovation. Whether the ancient Roman empire3 during the Hundred Years War4 ,5 or the current era, disease has never prejudiced for rank or status—affecting the rank and file as much as the senior commanders. Disease has been a quiet, and often unremarked, factor in history, yet it has altered the outcomes of military campaigns. An example of the role of disease is the discovery of Rickettsial disease affecting up to one-third of all French soldiers in the retreat from Russia in 1812.6 Over the previous century vaccination, modern pharmacology, improved hygiene and other public health and occupational health measures have transformed the health of the British Military. Even so, infectious disease and environmental stresses have still produced a heavy burden on deployed medical assets on both exercise7 and operations,8 and a background level of disease has always persisted.
The background burden of non-battle injury is known as ‘disease and non-battle injury’ (DNBI). The term DNBI is inclusive of underlying surgical disease, accidental injury and psychological illness, as well as the conditions managed by the speciality of General Internal Medicine (GIM). The acronym DNBI is useful at higher levels of planning, but less useful when it comes to preparing the teams of GIM doctors, nursing staff and support specialities for deployment or in the specific medical services provided in the field hospital. Understanding the spectrum of likely presenting symptoms, diagnoses, patient length of stay and disposal destinations is important to guide the appropriate scaling of specialist diagnostic modalities, provision of specific therapies and the grades, speciality and number of staff deployed, as well as informing medical logistics and evacuation planning. Training of the physician and nursing cadres will be directly influenced by operational GIM epidemiology, but more widely it will influence the deployment and training of all personnel involved in the treatment and transport of medical casualties on operations.
The ‘medical intelligence’ pertaining to a country or region attempts to quantify the risks to a deploying force, from the endemic infectious diseases, environment and climate. This knowledge helps anticipate the potential causes of both sporadic presentations and epidemics that may afflict a force located there. Not all disease is due to the specifics of the environment or geographical location, but often it is more general in nature, such as allergies, coronary artery disease and the chronic illnesses carried by troops into a theatre. As much of this disease arrives with the deployed troops, historical epidemiology data can help predict the range of future admissions. The British Armed Forces have been deployed to either Iraq or Afghanistan, in a war-fighting or nation-building role, for over a decade. A summary of the overall GIM speciality burden of disease, as seen at the field hospital level, was collected in Iraq and is now in the public domain.9 Similar large-scale cross-sectional surveys from US military deployments are also available.10
The Role 3 Medical Treatment Facility, commonly known as the ‘Role 3 Hospital’, in Camp Bastion was the British military hospital located in Helmand Province, Afghanistan. The hospital was primarily manned by British, American, Danish and Estonian military medical personnel who provided secondary medical care for the International Security Assistance Force, entitled civilian contractors and some local nationals. There has been a continual collection and dissemination of anecdotal or case-study data within the GIM cadre, based on their experience there and at other locations within Afghanistan, but as a whole this experience has not been published in the medical literature. Now UK operations in Afghanistan have closed, recording this data is important. This observational study is intended to formalise and record some of the collective experience of the GIM speciality from the Afghanistan operation. It is anticipated that this work, combined with the other UK and US studies,9 ,10 will provide a reservoir of knowledge available to the medical planners and commanders of the future.
Methods
Over a 2-year period from April 2011, demographic and clinical data were prospectively collected for consecutive admissions, under the GIM team, to the Role 3 Hospital in Camp Bastion, Afghanistan. All GIM admissions were eligible including UK and allied military personnel, civilians and those patients held in detention by the security forces. Patients who were seen in the emergency department or as consults to primary care, but who were not admitted, were not included nor were patients admitted under the surgical teams that required physician input. Data were prospectively collected by successive GIM trainees and were later cross-checked with the hospital electronic patient record to prevent omissions. Patient details recorded included gender, rank, age at admission, date of admission, length of stay, presenting symptoms, discharge diagnosis and disposal destination. Up to four different symptoms and diagnoses were recorded for each individual. Both symptoms and diagnoses were coded using the WHO International Classification of Disease, V.10.11 Coding was performed by two physicians (AC, JL) based on information entered into the database with access to the original electronic healthcare records if doubt existed about which field was most appropriate. Comparator data relating to the population at risk and total admissions were obtained from Defence Statistics. Authorisation for this study was obtained from the Research Directorate at the Royal Centre for Defence Medicine (Protocol: RCDM/Res/Audit/1036/12/0305).
The findings are presented in descriptive form. Statistical analysis was carried out using commercially available software (SPSS PASW Statistics Release V.18.0.0). Quartile–quartile plots and the Kolmogorov–Smirnov and Shapiro–Wilk tests were used to assess distribution normality. Significance testing was performed using the Student's t test, the Mann–Whitney test or Fisher's exact test. A two-tailed p<0.05 was considered significant.
Results
General observations
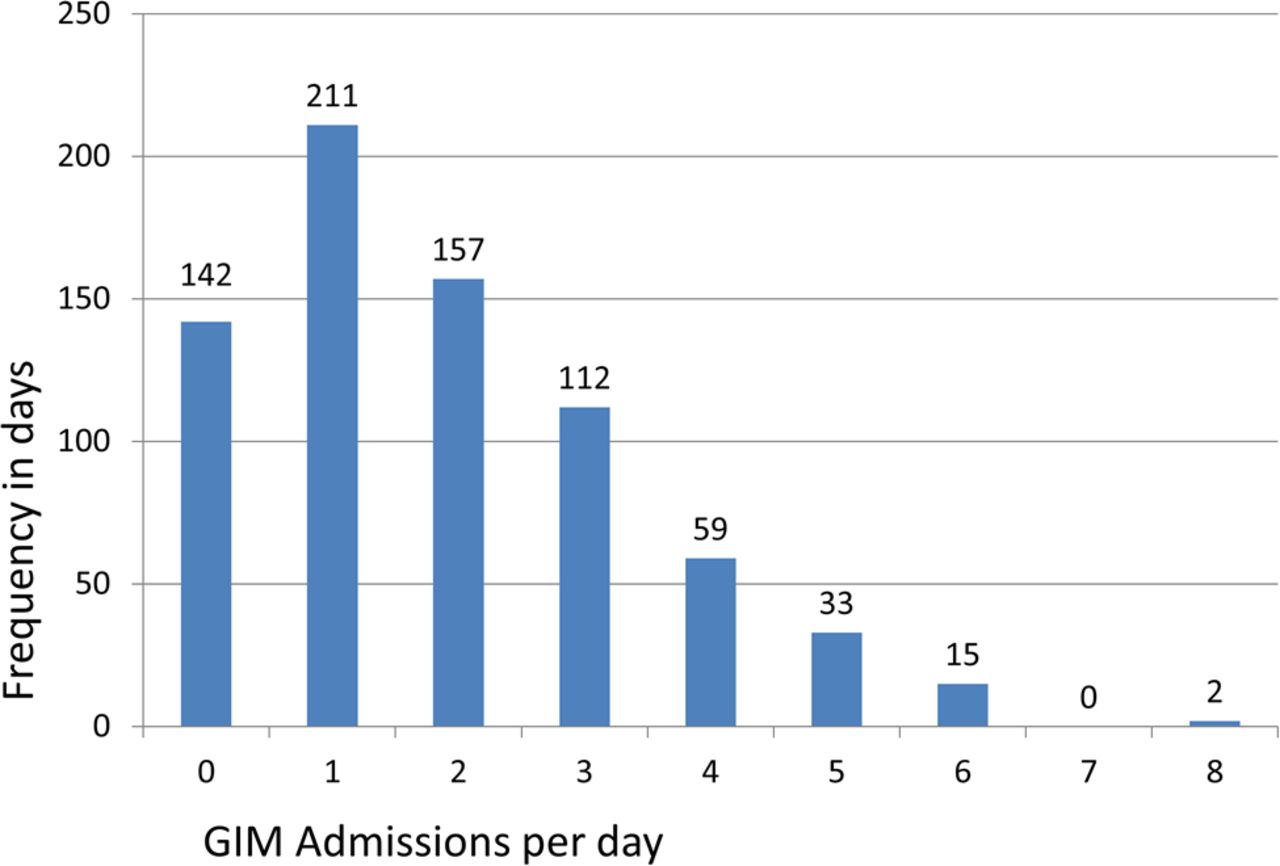
There were 12 978 presentations to the Role 3 Hospital over the 2-year period. A total of 6838 (52.7%) of these were admitted and of these 1368 patients (20% of admissions; mean 1.87 patients/day) were admitted to the hospital under the GIM team (Figure 1) with the general demographics summarised in Table 1. The 5470 non-GIM admissions (80% of admissions; mean 7.49 patients/day) were treated under the non-GIM teams and while there may have been GIM input into the care of some of these patients, this was not recorded in this study.
Demographics of GIM admissions to the Role 3 Hospital, Camp Bastion
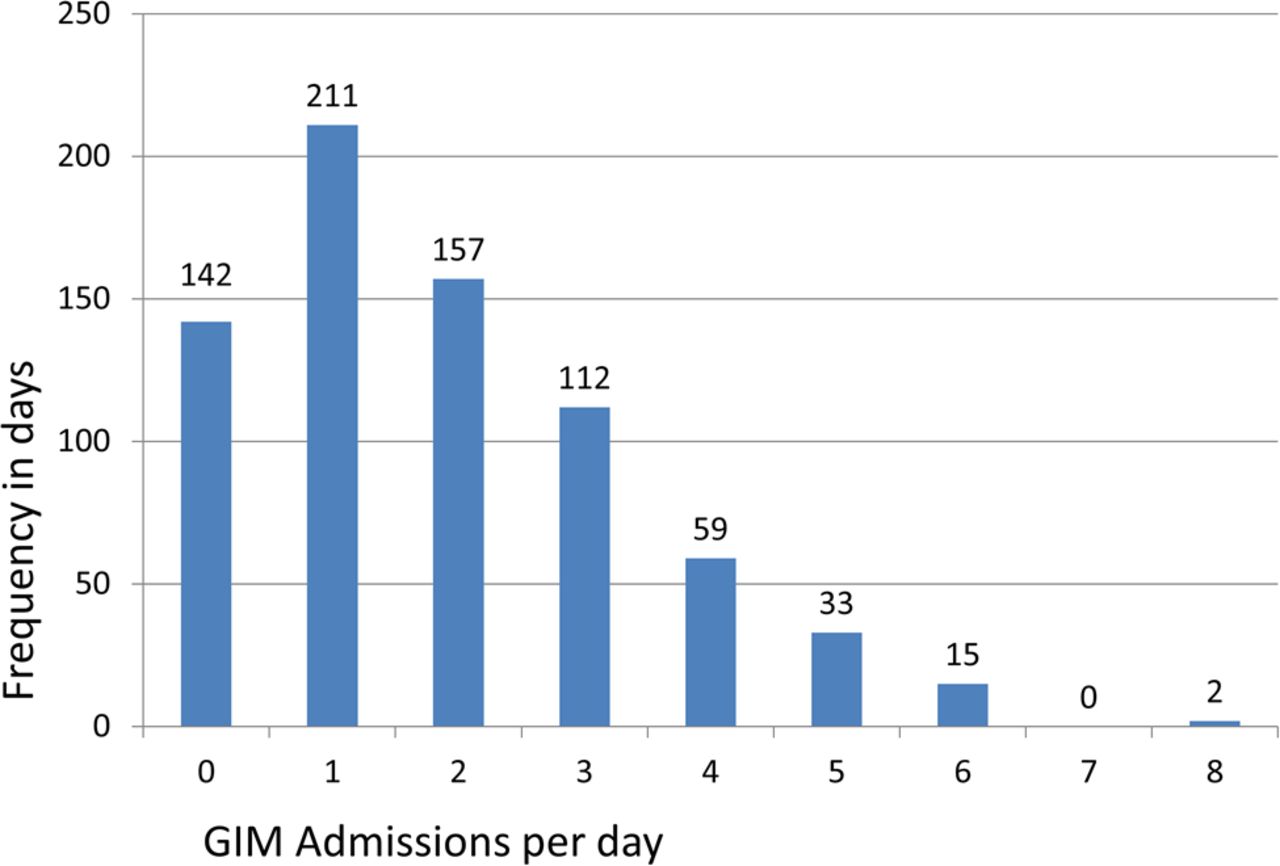
The numbers of General Internal Medicine (GIM) admission per day over the 2-year period.
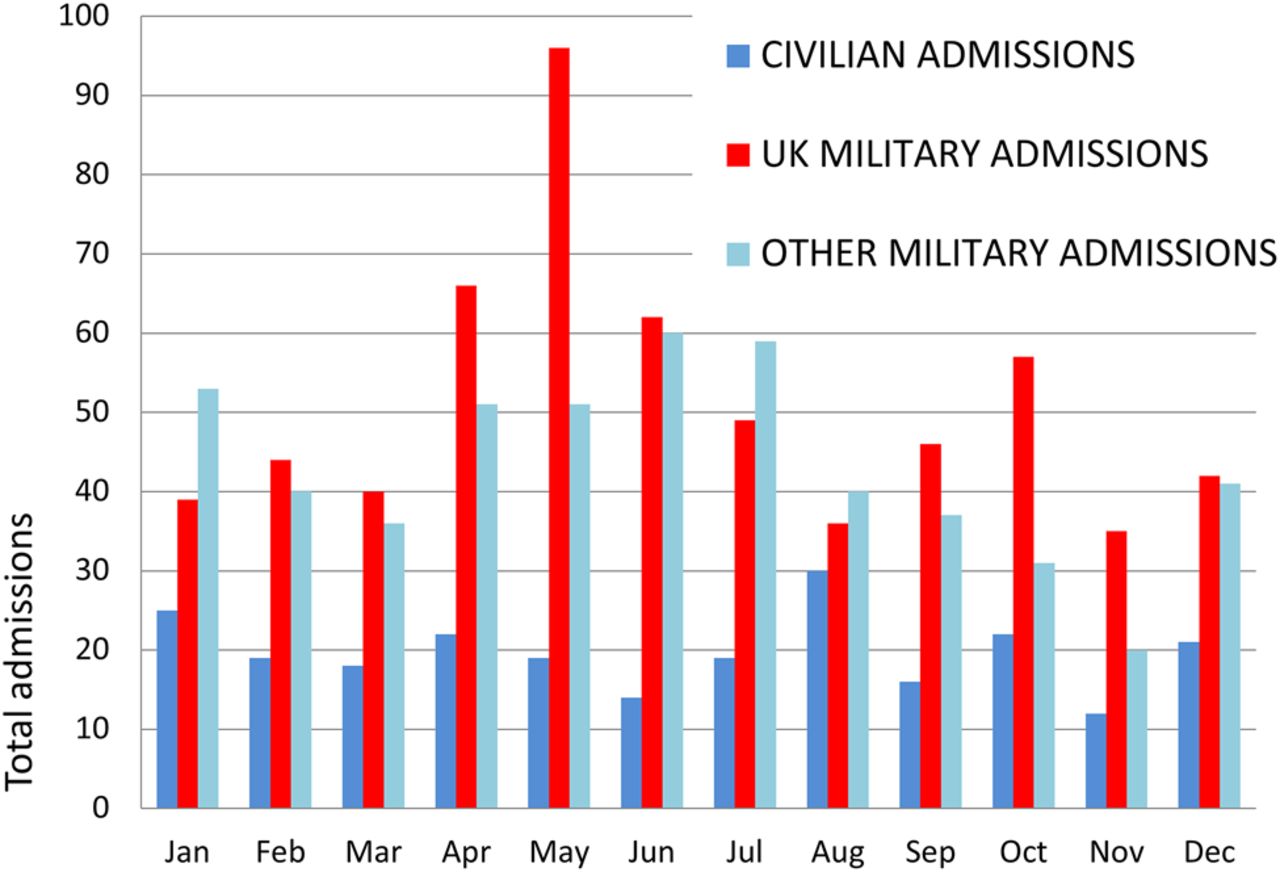
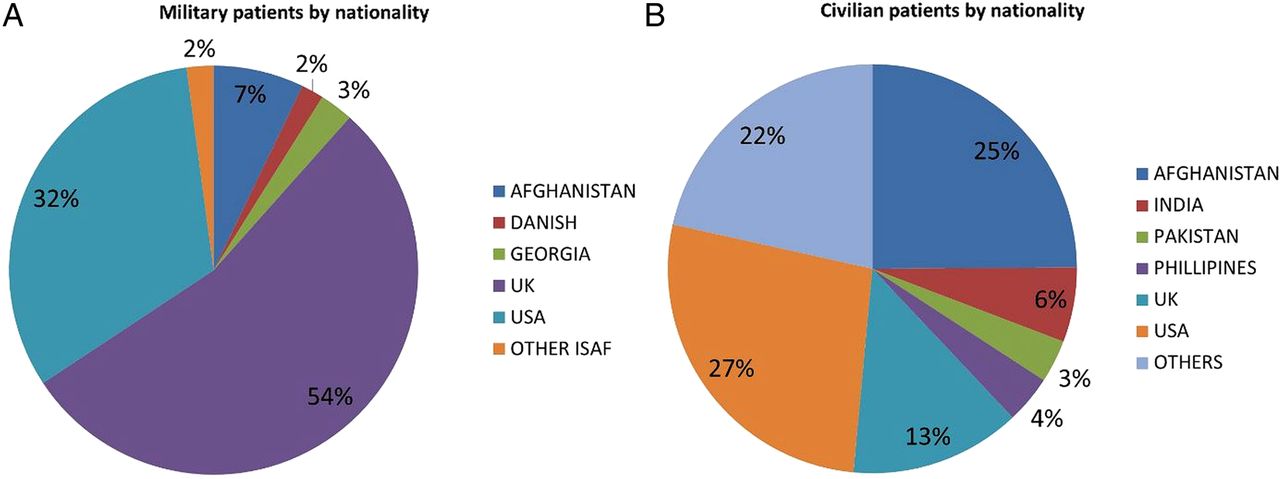
Over the 2-year period, the mean UK military population at risk was 10 941 per month. The UK military population fluctuated with increases in military personnel during the biannual handover periods, the first around April and May and the second around September and October. April and May were particularly associated with peaks in the total number of daily admissions (Figure 2). In total, there were 612 UK military admissions with a mean GIM admission rate of 23.3 per 10 000 UK military per month, but this increased to 42.2 per 10 000 UK military per month in May (p<0.005) (Figure 3). Military patients originated from only five countries (Figure 4A) while civilian admissions (Figure 4B) originated from 23 countries, including those close to or neighbouring Afghanistan in central and south Asia, as well as North America, Europe, the Middle East, Africa and Afghanistan itself. There were more male patients admitted than female patients, by a factor of nearly 17, which reflected the predominantly male nature of the population at risk, for both military and contractors alike. Although the UK military population during the operational period was under 10% women,12 the number and proportion of women in the theatre was unknown, so meaningful comparison cannot be made. There was no significant difference in the ages of UK or non-UK soldiers at 29 years (p=0.216). The civilian admissions were significantly older (p<0.001) and had a much greater age range. Five children (<18 years of age) were admitted.
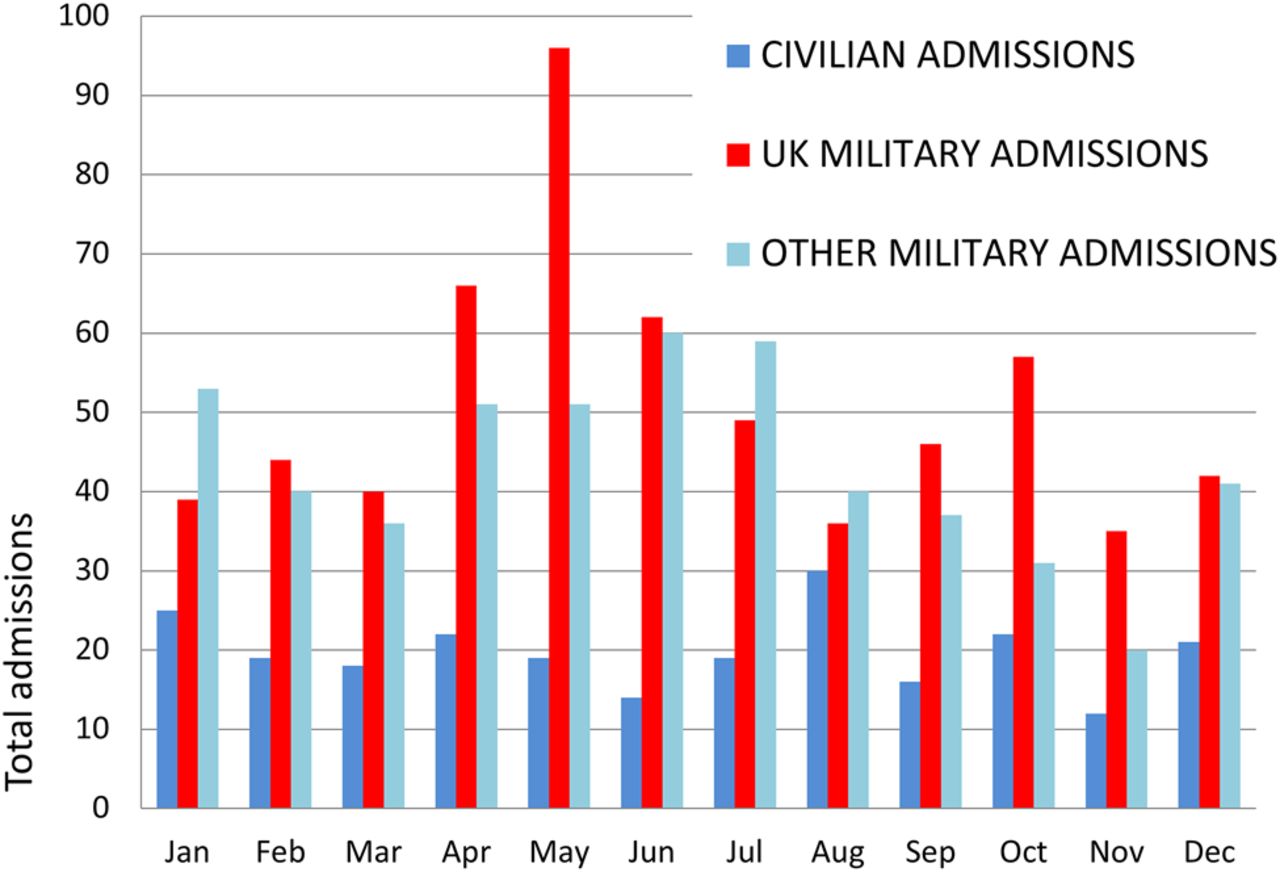
The General Internal Medicine (GIM) admissions by month and divided by patient category (Civilians, UK Military and non-UK Military).
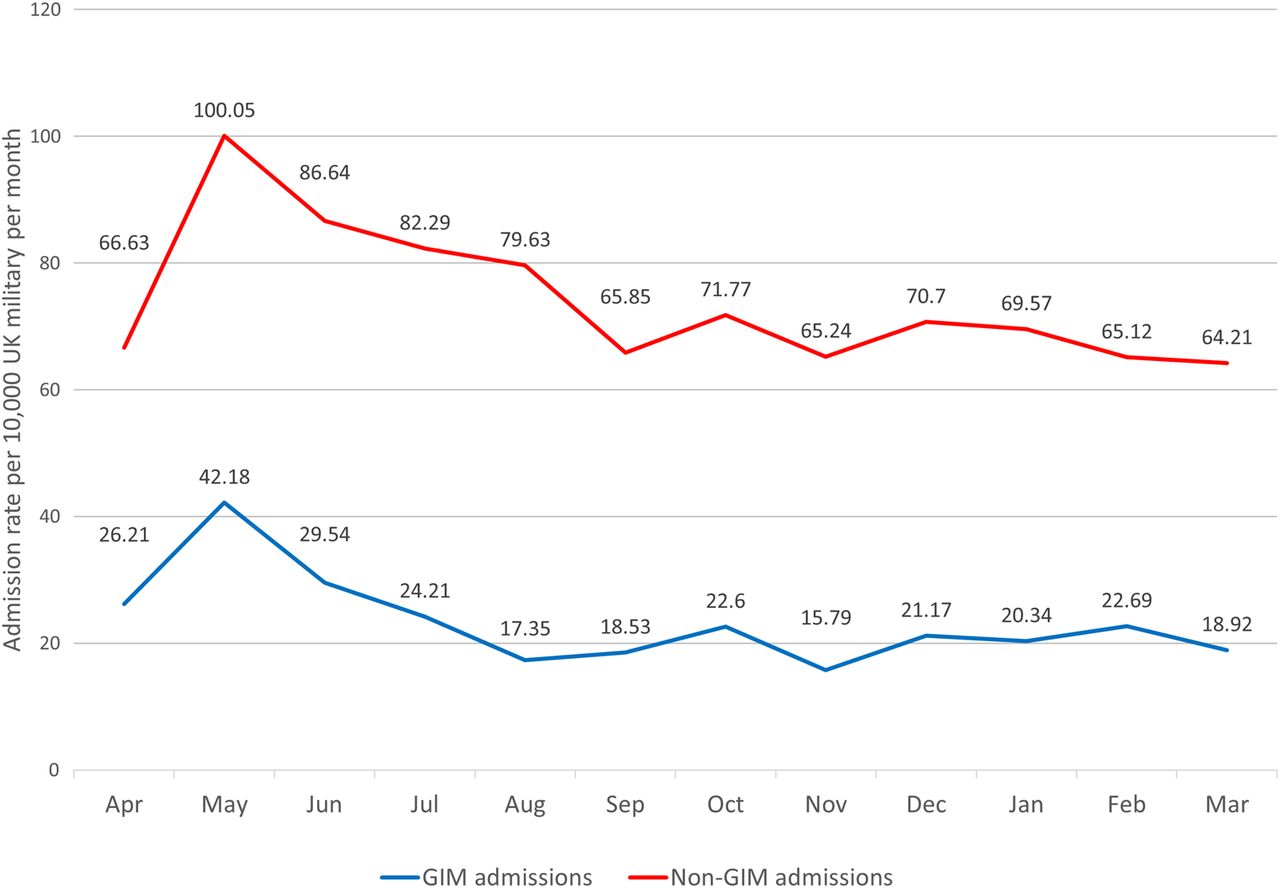
UK Military admission rates per 10 000 UK Military per month.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
The nationalities of military (A) and civilian (B) patients.
Presenting symptoms
There were 1656 reported symptoms differentiated into 142 different presenting symptoms. The 20 most frequent symptoms for each of the three groups are summarised by frequency in Table 2. There are striking similarities between the three groups with symptoms of pain in the throat and chest (158 cases), diarrhoea (total 154 cases), fever (154 cases), syncope and collapse (139 cases), nausea and vomiting (126 cases), headache (105 cases) and rash (79 cases) all occurring in the top ten symptoms for all three groups. There were 22 cases of snake or mammal bites, though none of these occurred in UK military patients, as well as a number of scorpion stings.
Summary of the 20 most frequent presenting symptoms by patient group
Diagnoses
The most frequently occurring diagnoses were similar in all three patient groups (summarised in Tables 3⇓–5) and were dominated by infectious disease, particular infectious gastroenteritis, lower respiratory tract infections and cellulitis. Other notable infectious diagnoses included Q-fever, tuberculosis and malaria. Frequent non-infectious diagnoses were neurological, particularly epilepsy and migraines; cardiovascular, including acute myocardial infarction and angina, arrhythmias, pericarditis and pulmonary emboli; and respiratory disease that included asthma. In the military groups, heat illness was a particularly common environmental condition and it constituted the second greatest group of UK military patients. Encounters with endemic fauna generated numerous admissions due to mammal bites, snake bites, with or without envenomation and scorpion stings. There was a significant number of patients in whom no definitive diagnosis was made, (Table 5) and this was dominated by symptoms of undifferentiated febrile disease, chest pain, syncope, palpitations and headache. A full list of all 1626 discharge diagnoses are collated and discussed in further detail in the online supplementary material.
Summary of the 1368 primary diagnoses by ICD 10 chapter
Summary of the discharge diagnoses occurring on three or more occasions and by patient group
Summary of the discharge diagnoses occurring in ICD10 Chapter R00-99 ‘Symptoms, signs and abnormal clinical and laboratory findings, not elsewhere classified’. Summary of those codes present on three or more occasions by patient group
Psychiatric illness
Psychiatry was not the focus of this study yet it contributed a significant minority of the patients seen (60 patients, 4.4% of admission). In the absence of a psychiatrist co-located at the hospital, any British patient with a primary psychiatric disorder, particularly when there was an issue regarding his or her safety, or the safety of others, was admitted under the GIM team. These referrals could originate from primary care, the field mental health team or the emergency department. The majority were due to acute stress reactions.
Children
Five children (civilians of age <18 years) were admitted under the GIM team. Three children presented following snake bite envenomation (two aged 10 and one aged 13 years), one with typhoid (aged 13 years) and one following an opiate overdose (aged 2 years). All five survived following appropriate and life-saving treatment. One of the snake bite patients used the hospital's entire supply of antivenom and required multiple clotting factor transfusions and several days in the intensive care unit.
Length of stay and disposal
The length of stay was relatively short for all three patient groups at less than 2 days. The hospital stays for non-UK military patients were shorter than for the UK military (p=0.001). The co-location of intermediate medical facilities in Camp Bastion, run by allied forces for their own personnel, may account for this difference. Length of stay for civilians was similar to UK military personnel (p=0.276) despite a few long-staying outliers skewing the civilian population to the right (maximum length of stay of 21 days). The overall disposal rates are summarised in Table 1 with a more detailed breakdown for the UK military only in Table 3. Almost three quarters of UK military patients were able to be returned to their units (RTUs) directly at discharge. The numbers are likely to be similar in the non-UK military cohort as further 62% were directly discharged to their units and a further 10.7% were discharged to an intermediate facility to convalesce. The RTU rate for non-GIM admissions was 40.2%. The majority of the remainder were evacuated to their home nation or, in the case of local civilians, to an Afghan civilian hospital (Role 4). Three GIM patients died. Two deaths were of western contractors following acute myocardial infarctions and one death was of a locally employed civilian following the recreational ingestion of methanol.
Discussion
There were differences between relative numbers of patients presenting to the Role 3 Hospital from different nations. It is unlikely that this accurately reflects the proportions of allied nations located in Helmand Province and it is probable that British servicemen and women had a lower threshold to present to the hospital as many were co-located with the hospital in Camp Bastion and might be more comfortable presenting to a British hospital than might a Georgian or Afghan soldier. Furthermore, the nature of the contributions of each of the allied nations meant that there were local differences in provision of both primary and secondary healthcare, intermediate discharge facilities and temporal fluctuations in the total population at risk. For example, a Role 2 facility was available for many of the American casualties elsewhere in Helmand, and the Danish, American and Afghan contingents all had intermediate facilities located within Camp Bastion. These facilities may, for example, account for the lower numbers of non-UK military presenting to the Role 3 Hospital with diarrhoeal disease as well as potentially enabling earlier discharge from hospital for non-UK military patients. This latter point might explain the shorter length of stay overall for non-UK military patients than UK military patients.
Superficial comparison with the case load following the Iraq invasion,9 as the most comparable set of data, shows some similarities. These include higher levels of heat illness and infectious gastroenteritis, and most strikingly, a spike in admissions during April/May rotations of UK military formations. This clear increase in admissions in May in Afghanistan has four likely explanations. First, more of the population at risk would be located close to the hospital prior to leaving Camp Bastion to return to the UK or to moving into forward locations. Ordinarily, being located geographically far from the hospital would mean that a majority of cases of infectious gastroenteritis would be managed locally by primary care. Second, as the population at risk was greater during rotation the implication is that the opportunity for the spread of infectious diseases might be facilitated by the more dense living arrangements. Third, the mobility of the military populations might expose them to pathogen strains to which they are immunologically naïve, resulting in disease symptoms. Fourth, personnel newly arrived in Afghanistan and still un-acclimatised might suffer from environmental disease, for example, heat illness due to the high temperature or acute asthma due to the dusty atmosphere.
Admissions came from a variety of countries; this may have presented potential communication problems. For the non-native English speakers a system of interpreters was well established and in the anecdotal experience of the investigators, communication between hospital staff and military patient was rarely a problem; however, the civilian patients came from a large number of nations and often no official interpreter was present, so reliable communication with this cohort could be challenging. This study did not investigate these potential issues associated with patient communications, but operating as part of a multinational coalition has been the reality of all recent UK military operations, and training on how to optimally work within this environment should be considered an essential part of the physician's training.
Often, whether a patient was admitted depended on the presenting symptom and on where they had arrived from and the time of their presentation. Anecdotally, many patients from isolated and remote locations would arrive in the evening or during the night on helicopter transport. We might hypothesise that when the symptoms in these patients were of a mild or ambulatory nature these patients may have been admitted to the hospital out of convenience, whereas had they arrived during the day they would have been discharged to their unit. These admissions may have skewed the data in favour of mild symptoms, but the data recorded neither time of admission or location nor the mode of transport to hospital. It is reassuring that the mean length of stay was short for all three groups. Ensuring a rapid turnover of patients meant that the maximum number of beds and hospital staff were available in case of a major incident. Given the relatively low daily admission rate of patients, their good underlying health in most cases and the limited discharge options, we hypothesise that it was possible to make earlier and easier decisions regarding discharge timing and destination than in the busier UK NHS hospital environment. Moreover, the practice of at least twice daily ward rounds may have further facilitated rapid discharge. Perhaps, the most striking figure relating to disposals though is the fact that of the British military admissions the vast majority (72.2%) return to their units and are able to continue in their operational role, with only just over a quarter requiring evacuation back to the UK. When the admissions relating to infectious diseases are examined in isolation, this RTU rate increases to 90%. This is, in particular, contrast to the non-GIM admissions where the RTU rate was only 40.2%, presumably due to the severity and frequency of the battle injuries and the prolonged recovery period following even relatively ‘routine’ surgery such as appendicectomy. What these data show is that most GIM symptoms are temporarily disabling, and following appropriate diagnosis and treatment patients can rapidly return to their operational roles.
The range of both symptoms and diagnoses in all three patient groups covered the full spectrum of general medical disease. This finding reinforces the ongoing requirement for military GIM trainees to undertake a broad range of training in addition to their more specialised subspecialty skills. It also reinforces the need for GIM consultants to continue managing unselected acute medical patients, while not deployed, in order to maintain their clinical skills.
Differences were seen between modern western medicine, as practiced in the NHS, and that seen in the operational environment. These differences highlight that the deployed physician requires additional training beyond that required of a purely UK-based, civilian practitioner. First, the presenting symptoms had a broader range than seen by most UK-based GIM doctors. These included more infectious diseases such as malaria, Q-fever and other causes of undifferentiated fever, as well as many cases of climate-related injury, snakebite and scorpion stings. These findings further inform the curriculum of the Defence Medical Services tropical medicine course. This course provides education in recognising and managing these conditions to clinicians throughout the Armed Forces and has developed into an integral part of physician training. The case mix also included a small number of children. Anecdotal reports of the management of paediatric cases highlighted a collaborative approach to the care of the child, drawing particularly on the experience of the Emergency Department and intensive care staff at the hospital. Psychiatric disease represented a significant minority of the case load and in these patients close liaison with the deployed field mental health team was vital. An understanding of the clinical features and acute management of the most important psychiatric disorders should be included in the education of the GIM and Emergency Medicine cadres.
Second, the range of investigations and treatments are more limited in the field environment and so clinical decisions are often made based on a thorough history and physical examination, tempered by clinical experience, than would be made in the First World environment where sophisticated diagnostics are available. Expanding the portable diagnostic skills of a military physician might be led by these data. An example might be competency in basic thoracic ultrasound, to enable safe chest drain insertion, basic ECG to allow immediate assessment of ventricular filling and function and improved laboratory diagnostics such as polymerase chain reaction to rapidly identify culprit infectious organisms. In other diseases, the ‘gold standard’ treatment might not be available. An example of this is acute myocardial infarction, where ideally primary percutaneous coronary intervention would be performed. Clearly, this is unavailable in Afghanistan so an understanding of thrombolysis, a therapy almost redundant in the UK, is required. In situations such as these, clear clinical guidelines and predeployment exercise in these therapies is useful to maintain operational efficiency. In situations where a diagnosis cannot be made, or recovery from illness might not be complete, understanding the operational requirements of the patient following discharge enables an appropriate occupational risk assessment. Thus, occupational medicine will remain at the core of differentiating the deployed military physician from their civilian counterpart.
Conclusions
In summary, these data provide a record of the numbers of GIM admissions, the admission rates in UK military personnel, the range of their symptoms and diagnoses and the length of stay and disposal that may improve operational planning in the future. These benefits can be seen in identifying training and material requirements prior to future military expeditions and in ensuring that the resources in theatre most closely mirror clinical need.
Acknowledgments
For their assistance in data collection the authors are grateful to the following: Capt Thomas Linton, Maj Jason Biswas, Maj Thomas Fletcher, Sqn Ldr Joanne Rimmer, Sqn Ldr Senti Baladurai, Sqn Ldr Christopher Adcock, Maj Kate Clay, Maj Damian Jenkins and Maj Christopher Johnson. For their assistance in collating the data pertaining to the population at risk, hospital admissions and aeromedical evacuations the authors are grateful to Surg Cdr Jo Leason at PJHQ and Caroline Trerise, Lea Trela-Larsen and Rachel Graham at Defence Statistics.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Contributors ATC conceived the project. AC, MS, MO designed the study. ATC, JL, SW, DSB, IP, MO and MS, collected the data. ATC, JL, SW, DSB, MS confirmed and analysed the data. SS and DW advised on methodology. All authors contributed to the manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.