Article Text

Abstract
Background It is increasingly recognised that diarrhoeal disease is an important contributor to disease non-battle injury (DNBI) rates on operations. Current data collection methods (J97/EPINATO) rely on self-presentation of patients to medical care, which is likely to under-record the true incidence of diarrhoea in theatre. Along with this, the data recording itself is less than adequate, with acknowledged issues in classification of diarrhoeal disease within J97/EPINATO categories.
Methods Two post-tour diarrhoeal disease questionnaire surveillance exercises were carried out at the end of Operation HERRICK 6 (H6) and 10 (H10), respectively.
Results Crude diarrhoeal disease attack rates were similar across the two surveillance periods with approximately 40% of troops questioned reporting at least one diarrhoeal illness episode. The severity of illness increased from H6 to H10 as measured by disease-related symptomatology and days ill and/or off work. Mission burden was substantial and increased in H10 compared with H6.
Conclusions Diarrhoeal disease is a significant cause of DNBI on operations. Current data collection methodologies underestimate its incidence and true operational burden.
- EPIDEMIOLOGY
- INFECTIOUS DISEASES
- PUBLIC HEALTH
Statistics from Altmetric.com
Key messages
-
Diarrhoeal disease remains a common and burdensome condition on operations.
-
Official data collection methods underestimate the incidence and operational burden of infectious diarrhoea.
-
Effective, prospective disease surveillance would assist in focusing Environmental Health/Public Health resources on the highest risk location and troops.
Introduction
Diarrhoeal disease in military populations is a common problem1–6 and has the ability to undermine the operational mission. For many years military diarrhoea has been classed alongside traveller’s diarrhoea with the assumption that the microbiology and the factors affecting its acquisition are the same. While the geography of risk and therefore the microbiological causes in general may well be the same, there are sufficient differences between these two populations to suggest we should look on them as separate and distinct populations from a disease susceptibility viewpoint. Factors that lead to the development of diarrhoea in military populations on operational deployments are, therefore, potentially distinct from those causing diarrhoea in travelling civilian populations and warrant further consideration. The burden of diarrhoea in deployed British servicemen has never satisfactorily been determined, but is likely to be substantial both to the unit and the mission.
With the maturation of the military operation it might be expected that problems identified, lessons learnt and adaptations made would have an impact on the attack rates of diarrhoea, its severity and the burden it places on the operational mission. On the other hand, might the changing shape of the mission and the intensity of the operation itself impact the measurable parameters of diarrhoea, such that its impact increases despite available knowledge?
Data produced by the Defence Analytical Services Agency (DASA) for the UK Surgeon Generals Disease Non-Battle Injury (DNBI) working group (http://www.dasa.mod.uk) show no significant reduction in reported gastrointestinal disease collected from primary care databases (J97/EPINATO). These data however relate to illness presentation rather than disease incidence. True incidence of disease is acknowledged to be underestimated in this type of surveillance data7–9 due to limitations in the collection tools and under-reporting of disease by troops.
Understanding factors leading to disease acquisition and the burden it produces is crucial in our ability to maximise force protection, the health of our deployed service personnel and, thereby, unit effectiveness and prosecution of the operational mission.
In an effort to understand this better, postoperational diarrhoeal disease questionnaire studies were undertaken at the end of two UK 6-month operational tours to Afghanistan, Operation HERRICK 6 (H6) and HERRICK 10 (H10). These examined factors that might be implicated in the acquisition of diarrhoea on deployment to Afghanistan as well as attempting to gauge the potential burden that diarrhoea placed on individuals and the mission, and attempted to draw conclusions regarding personal, environmental and public health issues that may be addressed to alleviate the burden of disease encountered in order to understand the real operational burden attributable to diarrhoea.
Methods
This study was a cross-sectional survey study assessing diarrhoeal disease surveillance at the end of Operation H6 (April–October 2007) and H10 (April–October 2009) deployments. The H6 surveillance exercise was carried out during post-tour decompression in Cyprus during the autumn of 2007 when diarrhoeal disease questionnaires were distributed to 2000 troops returning directly from Operation H6 on their way back to their home unit locations. All personnel were briefed on the nature of the surveillance, its intent and the potential use of the data. Strong emphasis was placed on the voluntary nature of the study but the importance of the exercise in understanding diarrhoeal disease in Afghanistan was stressed. The study briefing was delivered by personnel not involved in the study and not within the Chain of Command of the soldiers involved. Completed questionnaires were returned to the UK for entry onto a Microsoft Excel spreadsheet and after double entry verification all paper copies were securely destroyed.
The H10 surveillance exercise was conducted at Camp Bastion, Afghanistan, as troops were being processed for departure at the end of their operational tour in Autumn 2009. A similar questionnaire was distributed to over 2500 troops as they ‘checked in’ for their flights at the departure point, after a similar brief to that given in 2007. The briefing was given by a member of the Royal Logistics Corp movements staff independent of the study team and Chain of Command; questionnaires were identified but not directly handed to individuals. Completed questionnaires were collected when each flight had departed and an identical data entry, verification and paper disposal undertaken as in 2007.
The questionnaires were designed for ease of use, simplicity of understanding and with little option for free text entries to allow ease of analysis. Data collected included anonymous demographic data (gender and age), relevant military data (rank, unit), disease-specific data (diarrhoea, number of episodes, length of episodes, associated symptoms), illness behaviour data (presentation for care, self treatment) and potential risk/confounding factors (drinking non-certified water, eating local food, swimming/bathing/patrolling in open water sources, history of chronic bowel diagnoses, current smoker, history of appendicectomy, compliance with antimalarial prophylaxis and history of insect bites). H6 and H10 questionnaires were similarly constructed in content and form, but for the H10 surveillance, data were collected on specific geographical locations in an attempt to identify higher risk areas. No personally identifiable information was collected at any point in the surveillance exercise. This study was exempt from the Ministry of Defence Research and Ethics Committee (MODREC) approval (JSP 536 dated 21 January 2011).
Statistical analysis
In addition to descriptive analysis, risk factors for diarrhoea were sought. Categorical data were analysed using the χ2 test, Fisher’s exact test and χ2 test for trend as appropriate. Dimensional variables were analysed using a parametric or non-parametric tests depending on normality assumptions. Factors found to be significant in univariate analysis were used in a multivariate regression analysis using a backward stepwise iterative model to identify variables that were independently associated with the development of diarrhoea. For H6, a multivariate logistical regression model was used. For H10, a negative binomial model was used given the event and person-time data that were available. Statistical analyses were performed using Statistical Package for the Social Sciences (Chicago, Illinois, USA) and Stata V.11 (Statacorp Inc, College Station, Texas, USA). Two sided p values less than 0.05 were considered significant in all analyses.
Results
For the H6 surveillance exercise, 1988/2000 (99.4%) questionnaires were returned and analysed. Of the completed questionnaires, 97.8% of the 46 412 requested data fields were completed satisfactorily. In the H10 surveillance exercise, 2135/2631 questionnaires were completed and analysed giving an overall response rate of 81.15%, ranging between 32% and 100% between departing flights; 99.6% of 42 045 requested data fields were completed.
At least one episode of diarrhoea during their tour of duty was reported by 40.3% (H6) and 39.2% (H10) of respondents with an incidence rate of 12.9 and 12.1 per 100 person months, respectively. The average number of distinct diarrhoeal episodes, defined as episodes of diarrhoea separated by at least 48 h of normal bowel function, was 1.93 and 1.92 episodes per person per 6 months for H6 and H10, respectively.
Univariate and subsequent logistic regression and negative binomial models were used to assess risk factors for diarrhoea (Tables 1 and 2). The strongest risk factors were associated with patrolling activity and environmental location such as exposure to open water sources, insect bites and forward operating base (FOB) location; having a colleague suffering with diarrhoea was also a risk factor in this analysis.
Variables associated with diarrhoea on HERRICK 6
Variables associated with diarrhoea on HERRICK 10
For H10, data analysis was stratified by FOB location as well as Camp Bastion and Gurkha soldiers (Table 2). Variations in incident rates were noted, indicating a significantly higher risk of diarrhoea in two FOBs (referred to as FOB A and FOB B for operational security reasons) (23.4 and 20.3, respectively) compared with the overall rate, and a reduced risk in Bastion and within the Gurkha soldier population (5.0 and 3.4, respectively).
The burden of diarrhoea was measured: self-reported number of days lost to duty were measured at 9616 (H6) and 18 943 (H10) and number of days underperforming was 13 046 (H6) and 27 313 (H10); with an approximate population at risk (PAR) of 9000, this suggests overall aggregates of 22 662 and 46 256 days lost to effective duty (due to diarrhoea alone) for H6 and H10, respectively (Figure 1). Figures 2⇓⇓⇓⇓–7 summarise demographic and important disease-related data outcomes.

Calculated mission burden of diarrhoea in days.

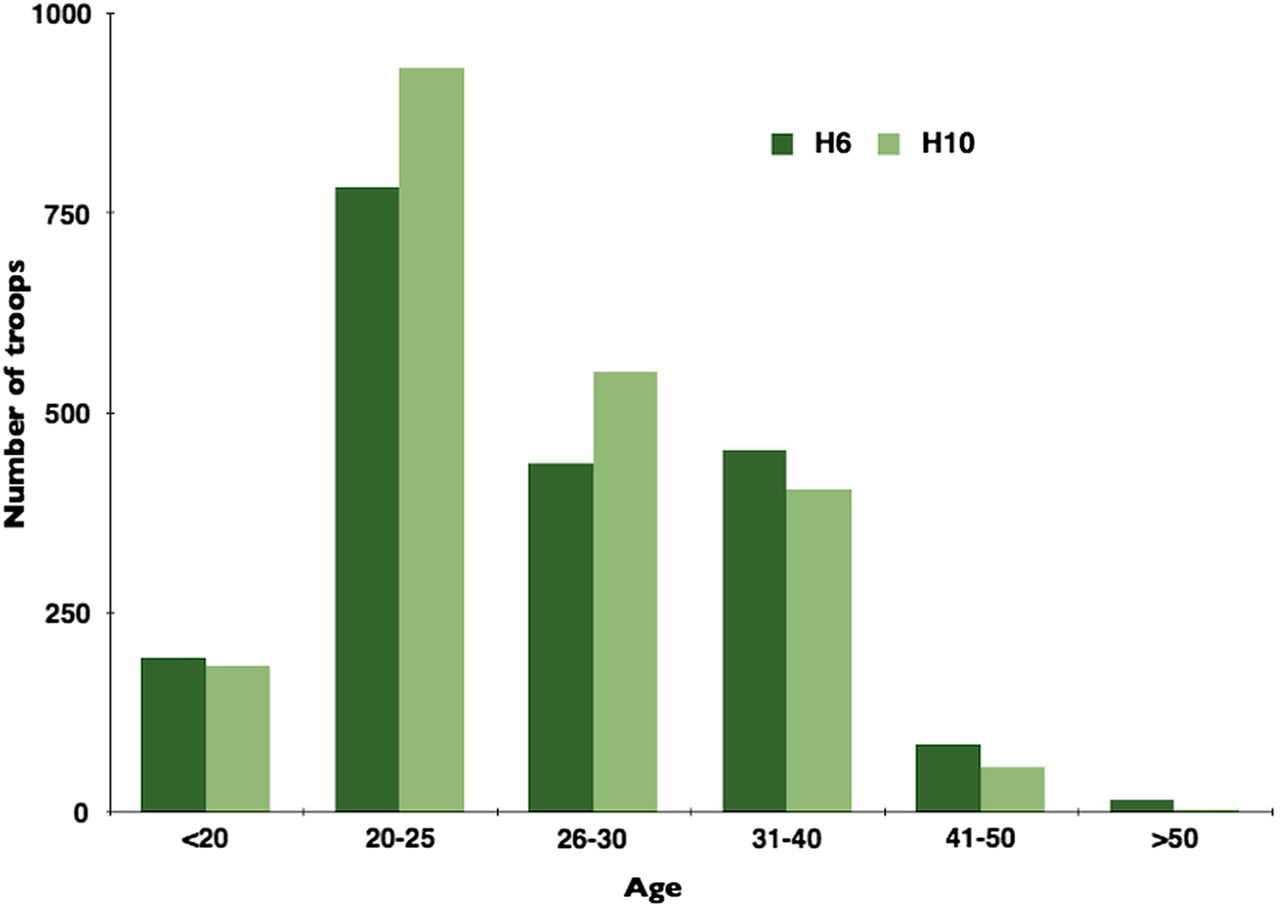
Age distribution of study respondents.

Rank distribution of study respondents.
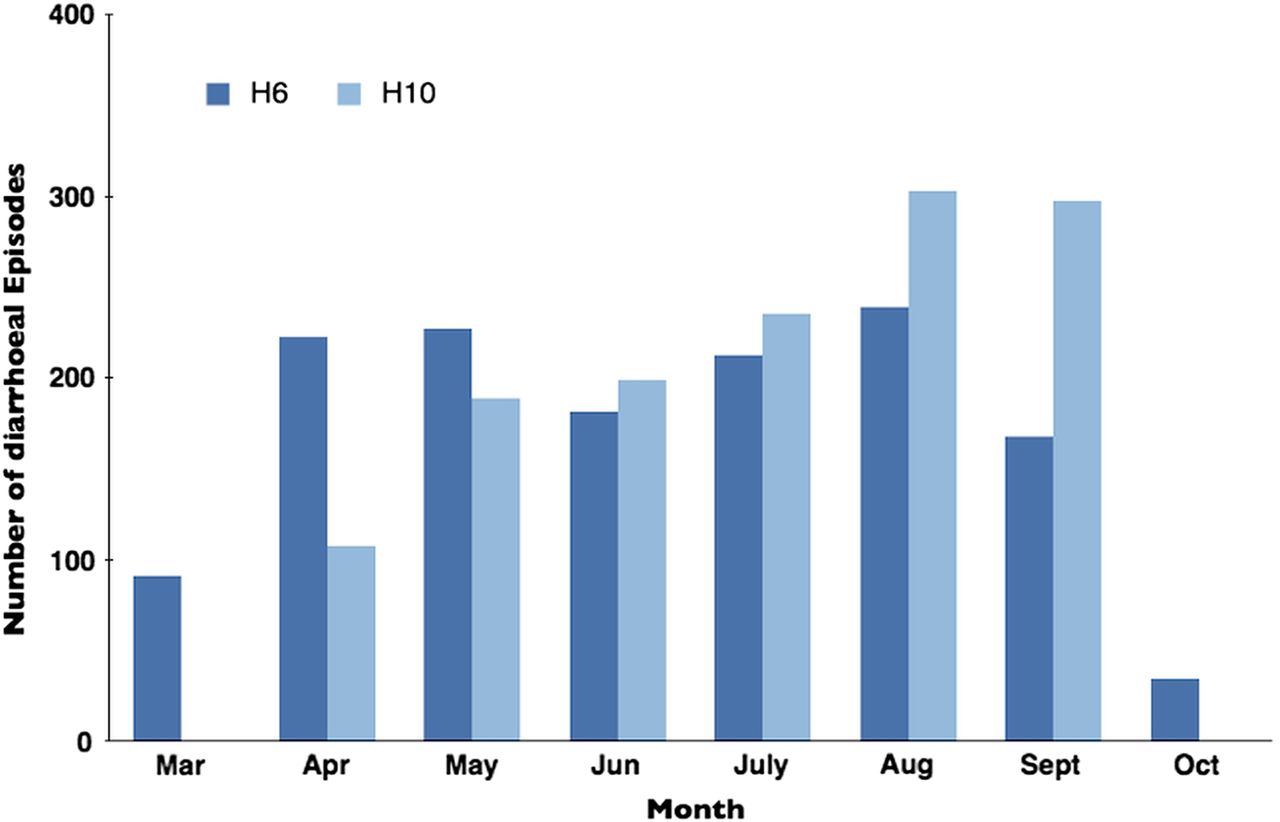
Number of diarrhoea episodes by month.
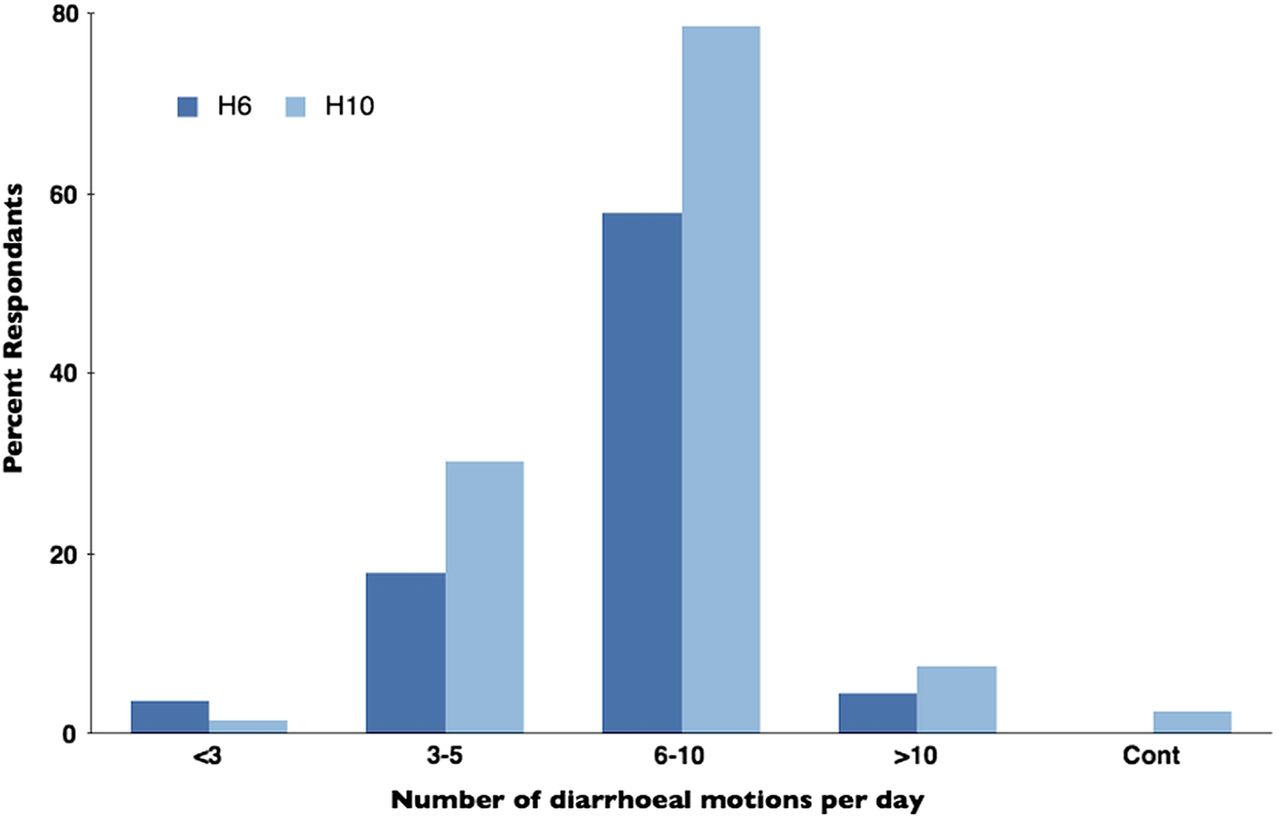
Reported frequency of bowel movements per diarrhoeal illness.

Length of diarrhoeal illness.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Number of respondents reporting symptoms associated with diarrhoeal illness.
Discussion
These data confirm the continued current threat of diarrhoea to individuals, units and mission in Operation HERRICK. The overall diarrhoea attack rate is consistent across the two data periods but the individual burden (measured by markers of attack severity) and the mission burden (measured by days lost to effective front line duty) increased significantly on H10 despite only a small uplift in PAR.
Anecdotally, it is acknowledged within theatre that some bases have a higher risk for diarrhoea than others. During the H10 surveillance exercise, we asked respondents to indicate if they were located in FOB A, FOB B or Camp Bastion, or were part of a Gurkha battalion. The first two were renowned (anecdotally) among troops for the high risk of diarrhoea, Bastion was anticipated to be low risk, and Gurkha soldiers were expected to be at lower risk of diarrhoea given previous studies in this subject10 and unpublished data from British and Gurkha troops exercising in Kenya (personal communication, Connor P, data from UK military soldiers exercising in Kenya 1999–2001). The overall diarrhoea attack rate and incident rate for the two FOBs was significantly higher than the overall rate and, as expected, the attack rate at Bastion and in the Gurkha population was significantly lower. These are the first data to support the anecdotal difference between deployed locations and more comprehensive data should be collected in order to best direct in-theatre resources. Person-specific risk factors that may be important for the acquisition of diarrhoea remain anecdotal, and assumptions are made with regard to behaviour and demographics that are expected to either enhance or reduce the risk of diarrhoea. Of all factors analysed, only swimming, bathing or patrolling in or through open water sources, having a colleague also with diarrhoea or suffering insect bites seemed to increase the risk of diarrhoea. These risk factors can all be seen as environmental—although not all avoidable nor able to be mitigated. Base location is clearly a geographic and environmental issue, and almost certainly influences the risk of insect bites (being more common near areas with vegetation), which appeared to act as an independent risk factor. Of the locations we found to be of higher risk, both border the ‘green zone’ and therefore would seem to be ‘environmentally’ at high risk, while patrolling activity brings troops into contact with open water sources on a regular basis. Colleagues who are sick seem to increase the risk—possible acting as a surrogate for camp environmental conditions and local infection control inadequacies, although this may well indicate similar levels of risk exposure in these high-risk locations. Environmental conditions and personal waste control within the camp environment—although not factored in this surveillance exercise—may well also play a part, and the contribution of deep trench latrines which are on their third or fourth dig on local insect load is unknown, although Riddle et al previously showed a differential diarrhoea attack rate with different latrine types.11
Interestingly, data collected in these two surveys did not reveal demographic risks for acquisition of diarrhoea. The number of women captured in the dataset was too small to reliably analyse. Age and rank did not show significant differences, although on both datasets age did show a trend towards protection for older soldiers. If age is taken as a surrogate for multiple previous exposures to high-risk environments and therefore pathogens, it may be that some protection is garnered, but insufficient to show significance.
Of critical importance, the data show a significant increase in the reported burden of diarrhoea on H10 compared with H6. Individual episodes of diarrhoea lasted longer (number of days until normal stool), were more severe (number of stools passed per day) and more individuals reported associated symptoms (vomiting, abdominal pain, anorexia). This is also reflected in the overall burden data. When asked how long they had to take off their primary work because of diarrhoea (per episode), the average number of days lost on H10 was 2.8 (1.17 on H6) giving a total duty days lost across the PAR of 18 943. When asked how long they functioned at less than 100% either when they were back at work after time off or when they carried on working despite their illness, the average on H10 was 4.0 (3.3 on H6) giving a total of approximately 27 313 days of underperforming across the PAR.
These underperforming data are important and an understanding of their effect on front line patrolling is crucial if we are to fully appreciate the burden diarrhoea produces on units. Days when a patrolling soldier is lost to duty because of illness can to some extent be mitigated by the unit either altering the pattern of activity to take account of a smaller team or by calling in a stand-by soldier to fill in. In one case there is some burden, albeit mitigated to some extent, and in the other case there is no effect (best case scenario). If however (because either they have not taken time off despite their illness or they have returned to duty before they have fully recovered) soldiers are patrolling at reduced performance levels, by the very nature their underperformance cannot be mitigated by command. Indeed, the effect on the patrolling team is often magnified as colleagues will often be guarded, and focus will switch at times between the task and the underperforming colleague according to direct conversations with front line soldiers. Time on task is reduced in a very hostile environment—something command is blind to. This increases the risk to the patrol, is unmitigated illness and when combined with days off duty we produce a ‘mission burden’ figure of over 45 000 days for H10.
It can only be postulated as to why the burden of diarrhoea increased over the 2 years between surveillance exercises despite no effective increase in PAR. The overall attack rate of diarrhoea remained fairly constant, but the burden of each episode has grown. Little is known of the microbiology of diarrhoea in Afghanistan, although this is being addressed. The surveillance periods covered the same months of the year and it therefore seems counter to what is understood about the microbiology of environments to imagine there has been a significant microbiological change to account for this increased burden. What did change during this period was the operational tempo and therefore the intensity of effort troops required for their daily tasks. It is likely that, although some clearly continue to perform despite disease, longer recovery for most indicates an awareness of the difficulty they face on return to duty and therefore reluctance to accept the associated risk and effort that goes with that if not performing as well as they expect. Again, this is based on face-to-face interviews with soldiers, is reflective and subjective, but nevertheless intuitive. A recently published paper12 has shown a significant gastrointestinal burden on soldiers undergoing severe physical stress, and relates this to evidence of increased gut permeability, perhaps suggesting a physiological cause for the increased burden when operational tempo is higher.
Attempts were made to compare data with formal J97/EPINATO data for the comparable period obtained through DASA. Definitive comparison is however difficult because of EPINATO categorisation leading to assumptions regarding defined diagnoses. Diarrhoea can be logged against three separate categories, none of which can be broken down and analysed for specific conditions. Also, while attempts were made to gain data from all locations, data provided from the two FOBs noted as high risk are not included in the Epi/NATO breakdown for this period. Headline data can be compared and show official estimates of ‘days off duty’ due to diarrhoea to be approximately 1996 with official days light duties approximating 792 for the whole 6 months. Other data from both of our surveillance exercises (not shown here) showed that less than 50% of those reporting a diarrhoeal episode reported anywhere in the ‘medical chain’. Given that a majority of these reported to team/platoon medics and were not recorded, the official recorded rate of diarrhoea is substantially less than our data suggest in keeping with other published data in these environments.7 ,8
Conclusions
The consistency of outcomes in the data collected during the two periods of H6 and H10 validates the accuracy of the data and reliability of the collection method in these retrospective cohorts. There is a consistent pattern of risk factors emerging for the acquisition of diarrhoea in Afghanistan. The operational burden due to diarrhoea increased significantly over the two periods and is likely related to operational tempo. Reliance on J97 Epi/NATO data significantly underestimates the prevalence of disease and the operational burden expected. Diarrhoea remains a consistent health concern and an important DNBI issue impacting directly on the ability of individuals and commands to prosecute their operational mission.
References
Footnotes
-
Contributors PC and EH designed, planned and conducted the study. MSR and HEM performed statistical analysis. All authors contributed to the writing, review and final construction of the manuscript.
-
Competing interests None.
-
Provenance and peer review Not commissioned; internally peer reviewed.
-
Ethics approval Obtained.