Article Text

Abstract
The Defence Medical Services aims to provide gold standard care to ill and injured personnel in the deployed environment and its prehospital emergency care (PHEC) systems have been proven to save lives. The authors have set out to demonstrate, using existing literature, consensus and doctrine that the NHS Skills for Health framework can be reflected in military prehospital care and provides an existing model for defining the levels of care our providers can offer. In addition, we have demonstrated how these levels of care support the Operational Patient Care Pathway and add to the body of evidence for the use of specialist PHEC teams to allow the right patient to be transported on the right platform, with the right medical team, to the right place. These formalised levels allow military planners to consider the scope of practice, amount of training and appropriate equipment required to support deployed operations.
- emergency medical services
- prehospital
- competencies
- military
Statistics from Altmetric.com
Key messages
A systems approach improves patient outcomes.
Defence Medical Services (DMS) Prehospital Emergency Care (PHEC) will benefit from this approach.
The NHS Skills for Health framework provides an existing model that can be used by the DMS.
This approach also helps PHEC coordinate Defence Lines of Development.
Introduction
The military Prehospital Emergency Care (PHEC) system saves lives.1 The foundations of this system are the point of injury interventions to control catastrophic haemorrhage and open the airway, taught to every member of the UK armed forces. Recent conflicts have also driven the development of robust training programmes for individual groups (eg, Battlefield Casualty Drills, Team Medic, Battlefield ATLS). Doctrine has been amended to indicate the required ratios of those with additional first aid training (one-in-four patrolling soldiers are required to be Team Medic qualified) which has improved our PHEC footprint. The spectrum of PHEC extends from individual and buddy aid at its most basic through all levels of professional care and at its highest level is the provision of a physician-led multidisciplinary team treating the patient during transfer to hospital in hostile environments. Care delivered at all levels should be considered within the context of the Operational Patient Care Pathway.2
Prehospital Emergency Medicine (PHEM) is a medical subspecialty recognised by the General Medical Council which is concerned with the critical care, treatment and transfer of undifferentiated, unscheduled patients with serious illness or injury prior to their arrival at hospital. PHEM is provided by specially trained physicians as part of a dedicated team and includes the interventions and critical decisions provided by those physicians (eg, prehospital emergency anaesthesia, blood transfusion resuscitative thoracotomy). PHEC (as opposed to PHEM) includes all aspects of emergency healthcare forward of deployed hospital care regardless of whether physicians are involved or not. As such, military PHEM should be considered a part of the wider military PHEC system, itself an important component of the end-to-end Operational Patient Care Pathway.
Echoing this period of rapid military medical development, civilian services have also recognised the need for well-governed prehospital systems with defined competency levels for the personnel working within them. NHS Ambulance Trusts and charity-funded Air Ambulances have seen the development of PHEM Specialist Trainees and Consultants as well as Critical Care Paramedics and Advanced Paramedic Practitioners. There now exists a bewildering array of trained personnel who provide emergency care in the field, in both the civilian and military arenas.
The NHS Skills for Health3 framework has already been applied to prehospital care and was adopted by the Faculty of Prehospital Care of the Royal College of Surgeons of Edinburgh as a matrix of clinical skills for PHEM4 addressing the medical competencies required for each level of care provider.
The aim of all military PHEC should be that the right patient is collected from the right pick-up point, transported to the right destination on the right platform, with the right medical escort in the right time frame.5 There is a need to define the clinical structure, components and capability of the military PHEC system in order to achieve the best clinical outcome for our patients and to better coordinate the development of the overall capability. This paper establishes the utility of the NHS Skills for Health framework as applied to military PHEC.
Method
A literature search was conducted to ensure all available evidence was used to create this matrix for competencies. The literature search was applied via the OVID interface on 13 October 2016 to the following databases:
MEDLINE (R) In-Process and Other Non-Indexed Citations and Ovid MEDLINE (R) 1946 to Present.
EMBASE 1974 to Present.
The keywords used were: competencies; training; emergency medical services; prehospital and a separate search included the term: military in the above search and are included in online supplementary appendix 1.
Supplementary file 1
To minimise publication bias, no restrictions on language, publication status or publication dates were placed on the search. CINAHL, all Evidence-Based Medicine Reviews (Cochrane Database of Systematic Reviews, Database of Abstracts of Reviews of Effects and Cochrane Central Register of Controlled Trials), Google Scholar and BestBETs were also searched. No further articles were identified.
The references of all papers and their references were then hand-searched to identify further relevant studies. The proceedings of recent Emergency Medicine conferences were searched to identify relevant abstracts. There were no exclusion criteria applied.
Of the 161 articles identified, 58 were duplicates. The contents of the remaining 103 articles were reviewed and assessed according to relevance to theme. Following review of these papers and the grey literature, five full-text articles were included in the final analysis.
The authors reviewed all available literature to inform appropriate competency-based level definitions for military prehospital care providers. Teams are defined by the most senior clinician on the team Increasing the number of providers on a team does increase the numbers of casualties that the team can treat, but it does not increase the level at which that team practises.
Classification of PHEC providers
A matrix, such as the one provided in this paper, is dynamic and part of an evolution of previous descriptions.
In 2011, Schwartz et al defined competency levels of tactical emergency medical support teams in the USA to ensure uniformity of training and competencies of their teams after a modified Delphi approach was used to inform their competency matrix.6 This is similar to the technique previously described that was used by the Faculty of Prehospital Care.
Morgan-Jones and Hodgetts in 19997 suggested a UK military system described as the Unified Emergency Care System to provide integrated medical support from point of injury to the time a casualty is handed over to specialist care within hospital. This paper builds upon this original work by including the advances in PHEC in place today.
van Schuppen and Bierens8 report in their paper that the Scandinavian physician-led mobile medical teams, dispatched to critically unwell patients, have the same competency set that the already dispatched ambulance nurses do, but may deliver a further skill set and that mutual understanding of these allows better cooperation in multiagency environments.
Murphy et al 9 suggest the requirement for key performance indicators (KPI) in PHEC to improve the quality of patient care and, through a three-round Delphi consensus group, described a list of 102 civilian PHEC KPIs. In a similar way, the UK Defence Medical Services (DMS) have designed training and education around five levels listed below:
Category 1—awareness—taught to all members of the DMS.
Category 2—basic—taught to all members of the DMS with a common role (eg, clinical personnel).
Category 3—advanced—taught to members of the DMS of a specific professional group (eg, doctors).
Category 4—specialist—taught to a subset of a professional group to provide subject matter expertise in a professional field.
Category 5—expert—taught to nominated individuals to provide reference subject matter expertise in a specialist field, for example, Defence Consultant Advisers, Specialist Nurse Advisers.
The NHS ‘Skills for Health’ framework’2 is specifically designed to be applicable to all areas of healthcare delivery. We have built on the categories described by the framework and have assigned levels to each group of practitioners in the military (Table 1).
The levels of PHEC
Scope of practice
Military PHEC teams should be classified by their fully trained and equipped lead clinician (hence a team led by a level 6 practitioner is considered to be a level 6 team). The level determines the degree of scene management and the capability of intervention expected. Increasing the size of the team means more casualties may be managed at once but does not necessarily mean that the level of care has become higher. An important principle is that practitioners at each level should be confident to perform all procedures and interventions at lower levels. For example, a Combat Medical Technician (CMT) 1 must be able to use the basic airway adjuncts described in the training for an Advanced Team Medic.
There is a critical distinction between levels 1–3 and 4–8. Level 3 and below are non-vocational providers, that is, their medical training is in effect advanced first aid training. Their military role remains foremost, but they can use their medical training on demand. Thus, they are regarded as combatants under the Geneva Conventions. Levels 4 and above are considered vocational providers and should use the protection of the Red Cross symbol and be considered non-combatants on the battlefield.
Equipment levels
Teams should carry medical equipment appropriate to their level of training. For example, all personnel on board a helicopter carrying a Medical Emergency Response Team (MERT) would carry the 587 ‘on the man’ module. In addition, their enhanced skill set would be supported by the use of the 590 MERT module, which includes all of the equipment and consumables required to administer prehospital blood transfusion and prehospital anaesthesia.
Analysis of the Operational Patient Care Pathway
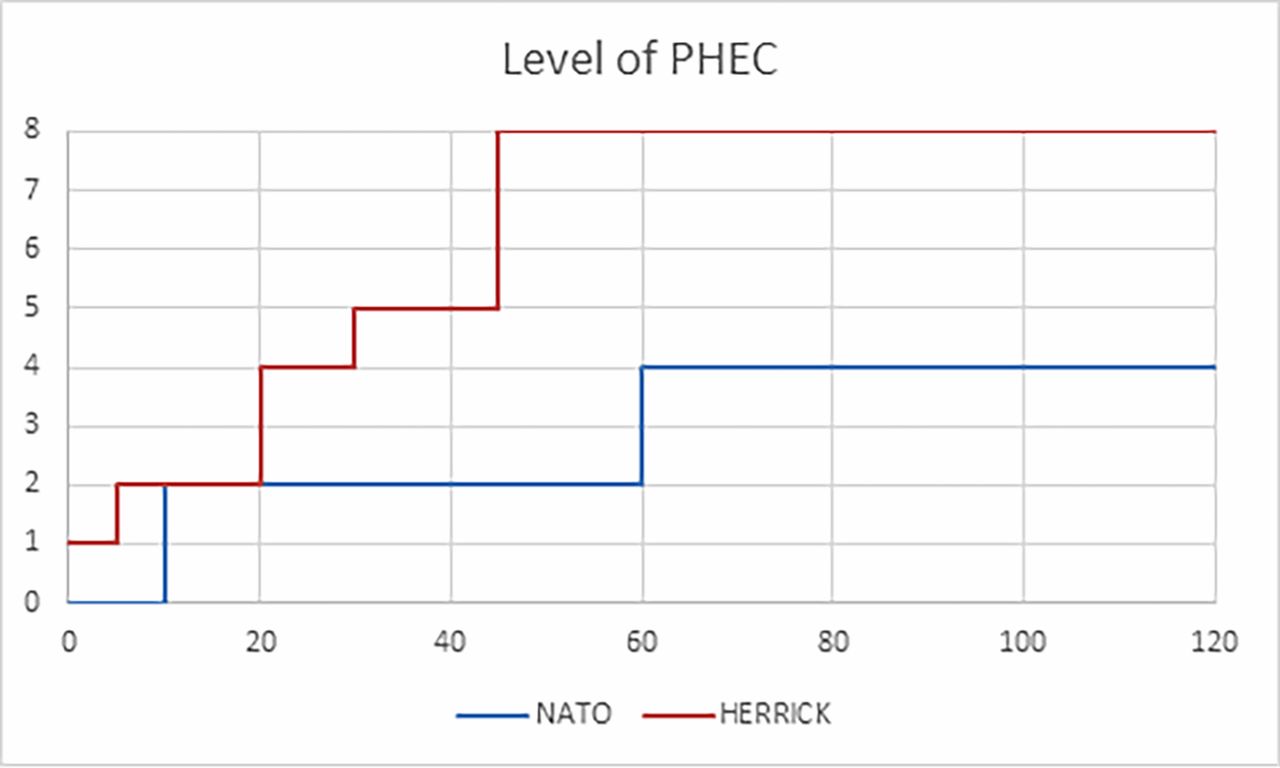
The Operational Patient Care Pathway from point of wounding through to the front door of the hospital can be analysed using this system and a level assigned to each stage of the casualty evacuation pathway (Figure 1). The levels of care should only ever increase. For example, a patient treated by a MERT (level 8) should not hand over a transfused and anaesthetised patient to a paramedic only team (levels 5–6) without continuing to escort the patient. The patient pathway can be plotted with level of care on the y-axis and time on the x-axis so that deficiencies are spotted and compared with North Atlantic Treaty Organization recommended timelines (Figure 2).
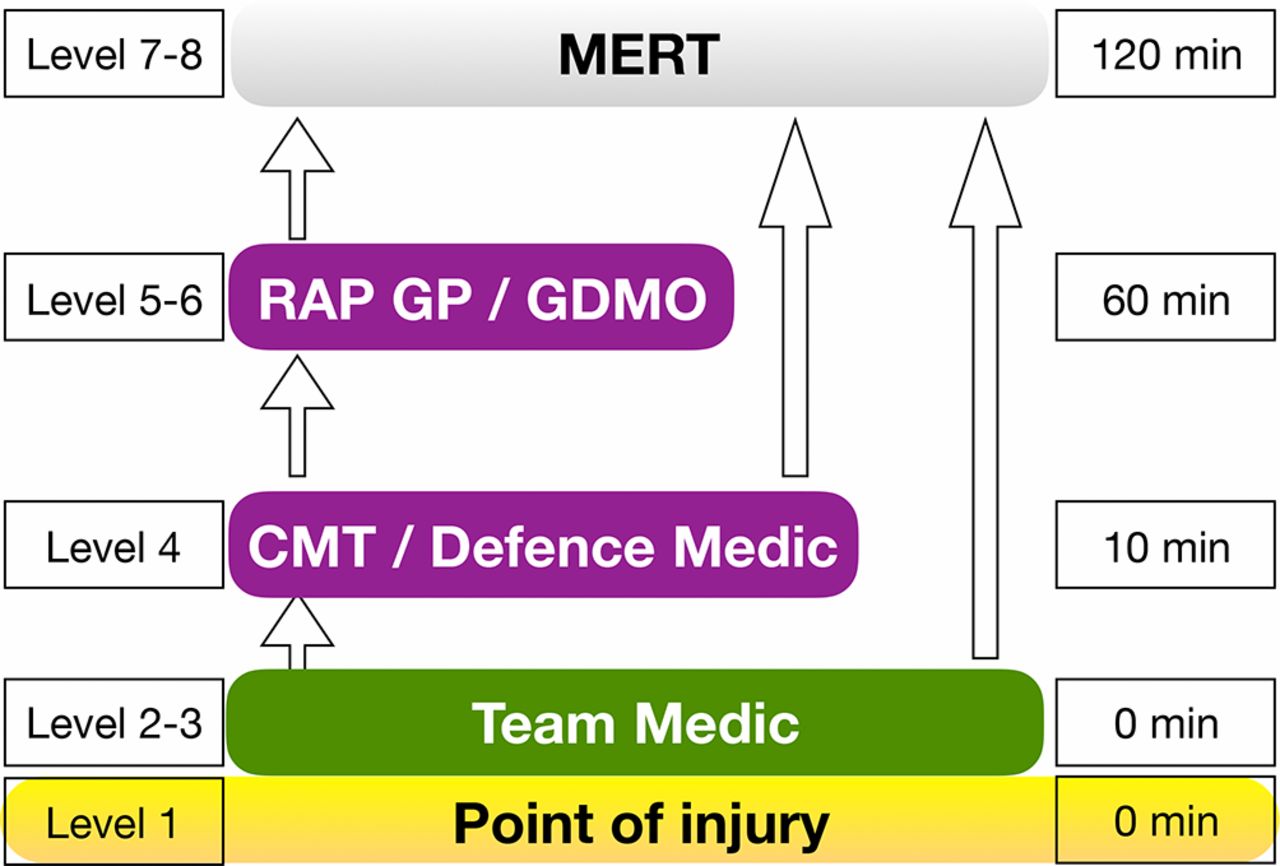
Prehospital Operational Patient Care Pathway. CMT, Combat Medical Technician; GDMO, General Duties Medical Officer; RAP, Regimental Aid Post; GP, General Practitioner; MERT, Medical Emergency Response Team.

The levels of PHEC against NATO timelines. NATO, North Atlantic Treaty Organization; PHEC, prehospital emergency care.
The utility of specialist PHEC teams
It is recommended that level 7/8 teams should be described as ‘Specialist PHEC teams’ to reflect the professionalisation of PHEM and its recognition as a clinical subspecialty by the GMC (General Medical Council). The first of these teams evolved in Helmand Province during Operation HERRICK and became known as the MERT.
In the civilian setting, there is a body of evidence that agrees that patient outcomes are better with specialist, physician-led PHEM trained teams10–12 but controversy as to who delivers what skill in the civilian prehospital setting is rife and is ongoing.13 14 von Vopelius-Feldt and Benger15 examine the current UK civilian system of enhancing standard paramedic delivered care with physicians and conclude that concentrating training and exposure on a small group of providers optimises benefits and reduces risk.
In the military setting, Morrison et al 1 reassure us that improved systems and improved training lead to better outcomes where higher level teams including physicians are compared with paramedic-led teams in Afghanistan between 2008 and 2012. It is important to note that particular benefit is seen in those patients with severe injuries and that there appears to be no survival benefit to being attended to in the prehospital environment by a physician when the patient was not severely injured.
This evidence underlines the requirement for the military to consolidate a pool of trained and continuously developed PHEM specialist physicians and supports the concept that higher levels of care improve patient outcomes. The level 8 PHEC teams currently fielded by the DMS include MERT(Air) by the Royal Air Force, MERT(Ground) by the Army Medical Regiments and Maritime MERT by the Royal Navy.
Levels of PHEC in practice—Operation HERRICK
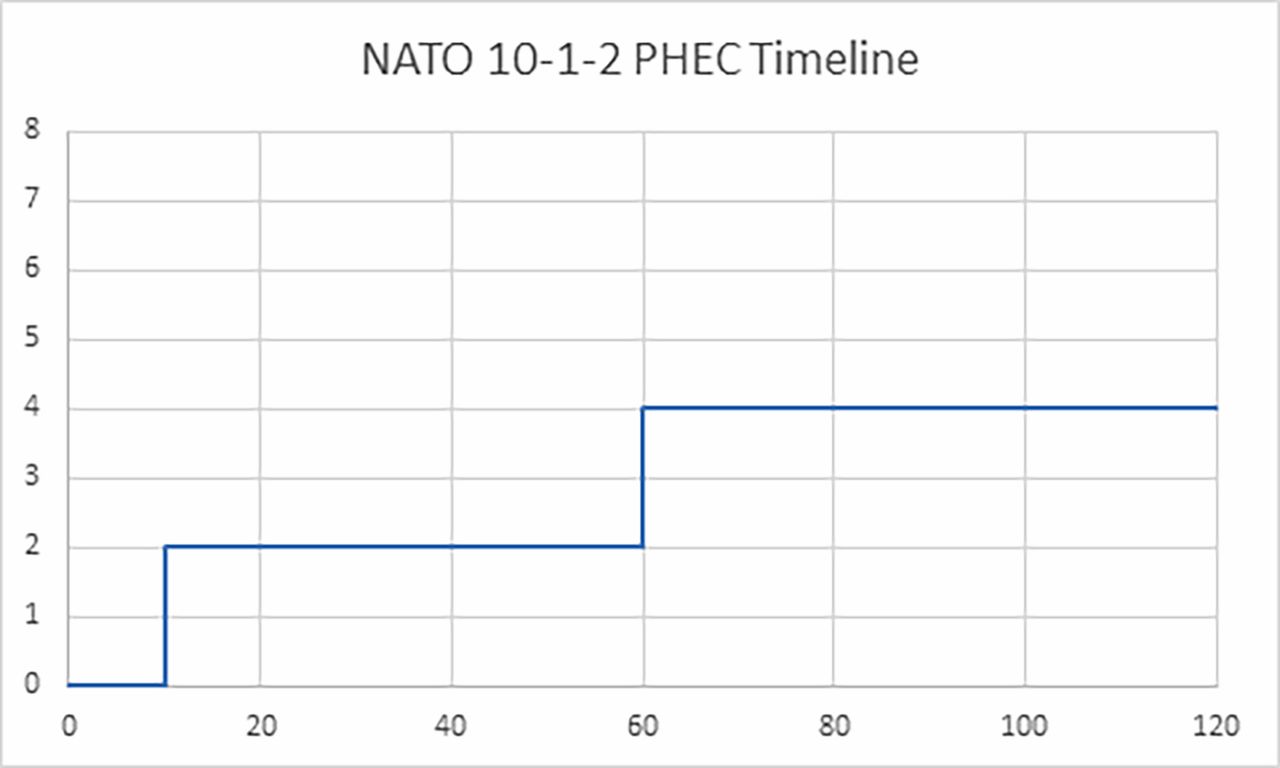
The care provided to fighting troops during Operation HERRICK has been commended.16 A retrospective look at a patient journey might show care as seen in Figure 3, although it should be noted that there is debate about acceptable timelines.17 Immediate Battlefield Casualty Drills were applied (level 1) and a Team Medic arrived within minutes (level 2). Many fighting patrols were supported by vocational providers—CMTs (level 4) and General Duties Medical Officers (level 5) who frequently took over the patient’s care, before handing over to the MERT which, towards the end of the conflict, was led by consultants in Emergency Medicine and Anaesthesia (level 8).
{kind=link}
{kind=link}
{kind=link}
The levels of PHEC on Op HERRICK compared with NATO timelines. NATO, North Atlantic Treaty Organization; PHEC, prehospital emergency care.
Summary
A systems approach to healthcare improves outcomes as witnessed by the Major Trauma System in the UK. The PHEC component of the UK Operational Patient Care Pathway would benefit from a systems approach to its organisation. The principles and assumptions for its organisation are listed in Table 2. The NHS Skills for Health framework provides us with an existing model to use when structuring military PHEC. The concept of ‘levels of care’ also enables us to coordinate the Defence Lines of Development needed to progress military PHEC, including the training and equipment required by individual practitioners from Battlefield Casualty Drills through to the specialist PHEC teams such as MERT.
Principles and assumptions
References
Footnotes
Contributors DS is the main author. JMcK was involved in literature review. SJ was involved with images. CW is the group lead and reviewer.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.