Article Text

Abstract
Introduction Musculoskeletal injury represents the leading cause of medical discharge from the UK Armed Forces. This study evaluates effectiveness of care provision within a large primary care rehabilitation facility (PCRF) against directed defence best practice guidelines (BPGs)
Methods All new patient electronic records from January to July 16 were interrogated to identify demographics, causation, injury pathology, timelines and outcomes.
Results 393 eligible records (81.9% male) were identified. 17.6% were officers, 32.8% were seniors and 49.6% were juniors. The average age was 35.1 years (mode 30). The average wait to treatment was 8.3 days with 75.6% key performance indicator compliance. 47.3% were repeat injuries. The average care timeline was 117.1 days with 8.7 average treatment sessions needed. 30 remained under care at 2 years. 17.8% accessed hydrotherapy and 44% underwent exercise remedial instructors care. 14.2% of individuals required concurrent DCMH care (15.9% male and 26.8% female). 28.5% required multidisciplinary injury assessment clinic intervention with 74.1% compliance against BPGs. 2.9% used the Defence Medical Rehabilitation Centre. Common pathologies were low back pain (LBP) (n=67), upper limb (UL) soft tissue (n=40) and knee trauma (n=38). LBP had the highest recurrence rates (71.6%). Anterior knee pain took the longest (173.1 days) but had the best outcome on discharge. Ankles and lower limb muscle injuries had the best outcomes. Patella tendinopathy and knee trauma had the poorest outcome on discharge. LBP and patellar tendinopathy had the lowest fully fit rates at 2 years (56.7% and 53.8%, respectively). At 2 years, 58.2% of individuals achieved full fitness (60.7% men and 46.4% women), rising to 64% and 55%, respectively, when including those retained with limitations.
Conclusions The PCRF was generally compliant with BPGs, achieving good functional outcomes on discharge. Women were disproportionally represented, had higher concurrent DCMH attendance and poorer overall long-term outcomes. Repeat injury rates were significantly high.
- musculoskeletal injury
- rehabilitation
- outcomes
Data availability statement
Data may be obtained from a third party and are not publicly available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
Musculoskeletal injury remains the leading cause of medical discharge from the UK Armed Forces.
Military rehabilitation services can achieve good functional outcomes on discharge, although repeat injury rates can be high.
Female personnel may have higher presentation rates, higher concurrent mental health involvement and poorer long-term outcomes compared with male personnel.
Introduction
Musculoskeletal injuries represent the leading cause of medical discharge from the UK Armed Forces.1 In the current climate of high manning pressures and low recruitment, maintaining deployable numbers of personnel becomes operationally imperative.2–4 It is therefore vital to rehabilitate injured personnel back to full occupational fitness as efficiently and effectively as possible to maintain sufficient personnel to cover operational requirements. While there are increasing volumes of data regarding battle injuries and non-battle injuries in deployed personnel,5 6 little accurate data exists for injuries sustained in the home base areas. The Department of Defence Rehabilitation (DDR) has published a comprehensive series of best practice guidelines (BPGs) for the management of specific musculoskeletal pathologies. These are evidence-based clinical guidelines that include timeline recommendations for when onward referral should occur from primary care to ensure efficient progression of care as required. In general, these suggest that patients should be referred on from primary care at 6 weeks if failing to progress appropriately. At the time of writing, there is no published large-scale accurate primary care rehabilitation facility (PCRF) effectiveness data or audit of performance against these recommended BPG timelines.
Aim
The objective of this study was to evaluate care pathways and long-term outcomes for musculoskeletal injuries against DDR BPG timelines within a UK defence PCRF.
Background
Every UK military establishment will have an associated PCRF to provide injury assessment and rehabilitation services. The complement of each PCRF will vary depending on the size of population at risk (PAR). PCRF Drake is one of the largest rehabilitation departments in the UK covering a PAR of over 6000. The PAR comprises almost entirely Royal Navy (RN) and Royal Marines (RM) personnel; while there are some triservice personnel, these numbers are comparatively small. The department itself comprises five full-time equivalent (FTE) clinical physiotherapists and two FTE civilian exercise remedial instructors (ERIs) offering a comprehensive rehabilitation service, including direct access clinics, exercise and manual therapy, acupuncture and hydrotherapy facilities. UK Defence operates a paper-free electronic medical record and data system (Defence Medical Information Capability Programme - DMICP). Historically, accurate data capture from primary care has been extremely challenging and unreliable primarily due to poor injury coding and data entry, combined with inaccuracies in DMICP searches. While some performance data are captured through DMICP, this predominantly comprises key performance indicators (KPIs), such as waiting times, and does not include either demographics or reliable long-term effectiveness outcomes. This service evaluation aimed to capture long-term care pathway information, demographics and effectiveness data to provide a baseline for future studies. It also aimed to evaluate the PCRF performance against the BPG referral timeline recommendations.
Military musculoskeletal injury
Musculoskeletal injury represents a significant attrition threat to military populations and is a leading cause of aeromedical evacuation, primary care attendance and lost work days.5 7 Within the US military population, it is estimated that musculoskeletal injury cost $548 million in direct patient costs in 2007 alone.8 The UK military population is significantly smaller and accordingly has less ability to accommodate high levels of non-deployable personnel without affecting operational capability. Several common factors have been identified that appear to contribute to musculoskeletal injury in the military population, including previous injury, gender, fitness levels, age and rank.9–16 Furthermore, certain injury presentations appear to be common with low back pain (LBP), regularly cited as a leading presentation associated with poor outcomes.10 17–19 In view of the detrimental impact that musculoskeletal injuries have on manning, operational deployability and the associated financial implications, it is essential to gain a clear understanding of the issue within the home base area. This may then assist in the direction of appropriate targeted injury prevention strategies.
Military rehabilitation poses unique challenges compared with a civilian population as occupational functional demands will generally be significantly higher. For the purpose of this study, the primary outcome of interest was achievement of a P2 Medical Employment Standard (MES) as this indicated a return to full occupational function. While individuals could be retained in service with a lower MES (ie, had some functional limitations to duty), this was no guarantee of compatibility with ongoing service.
Methods
The appointment book for PCRF Drake was interrogated for the dates 1 January to 30 June 2016 and all new patients identified. These dates were selected to allow up to a 2-year period of treatment to attempt to ensure capture of discharge and outcome data. Individual DMICP records were manually interrogated, and anonymised demographics and care pathway data were collected. Records were excluded if the care pathway was not initiated in HMS Drake, that is, were already under care from a different healthcare provider and transferred to the PCRF. This was intended to try to capture true end-to-end care pathway data and to attempt to limit treatment inputs to PCRF Drake alone where possible. Outcome data were captured through the individual’s current MES at the time of interrogation and the validated patient self-reported Functional Activity Assessment (FAA) score on admission and at the time of discharge from the PCRF. FAA 1 or 2 both represent the ability to perform the individual’s primary role and broadly represent a P2 or P3 MES. Table 1 indicates a summary of FAA scoring.
Patient self-reported FAA score
Pathology type was categorised using the pre-existing generic J97P injury codes entered on assessment by PCRF staff . Causation was identified from the initial assessment notes and placed into a set of categories agreed within the department. Repeat injury rates were determined by whether evidence of the same injury was located within the individual’s DMICP record. This was not time limited.
Results
A total of 422 individuals were identified in the 6-month study period. Twenty-nine data sets were unavailable due to having been archived (with the individual either medically discharged or having left the service). This provided 393 complete records for interrogation.
Demographics
Demographics were extracted from the individual’s DMICP registration section. Men represented 81.9% (n=322) of injury presentations compared with women at 18.1% (n=71). The average age was 35.1 years, with a mode of 30 years. RN and RM personnel represented the bulk of the total patients seen (96.7%). Army and RAF personnel represented 2.3% and 1.0%, respectively.
Rank
Table 2 shows the breakdown of the presenting patient population by rank against the RN manning proportions.20
Population breakdown by rank versus overall RN population
Injury causation
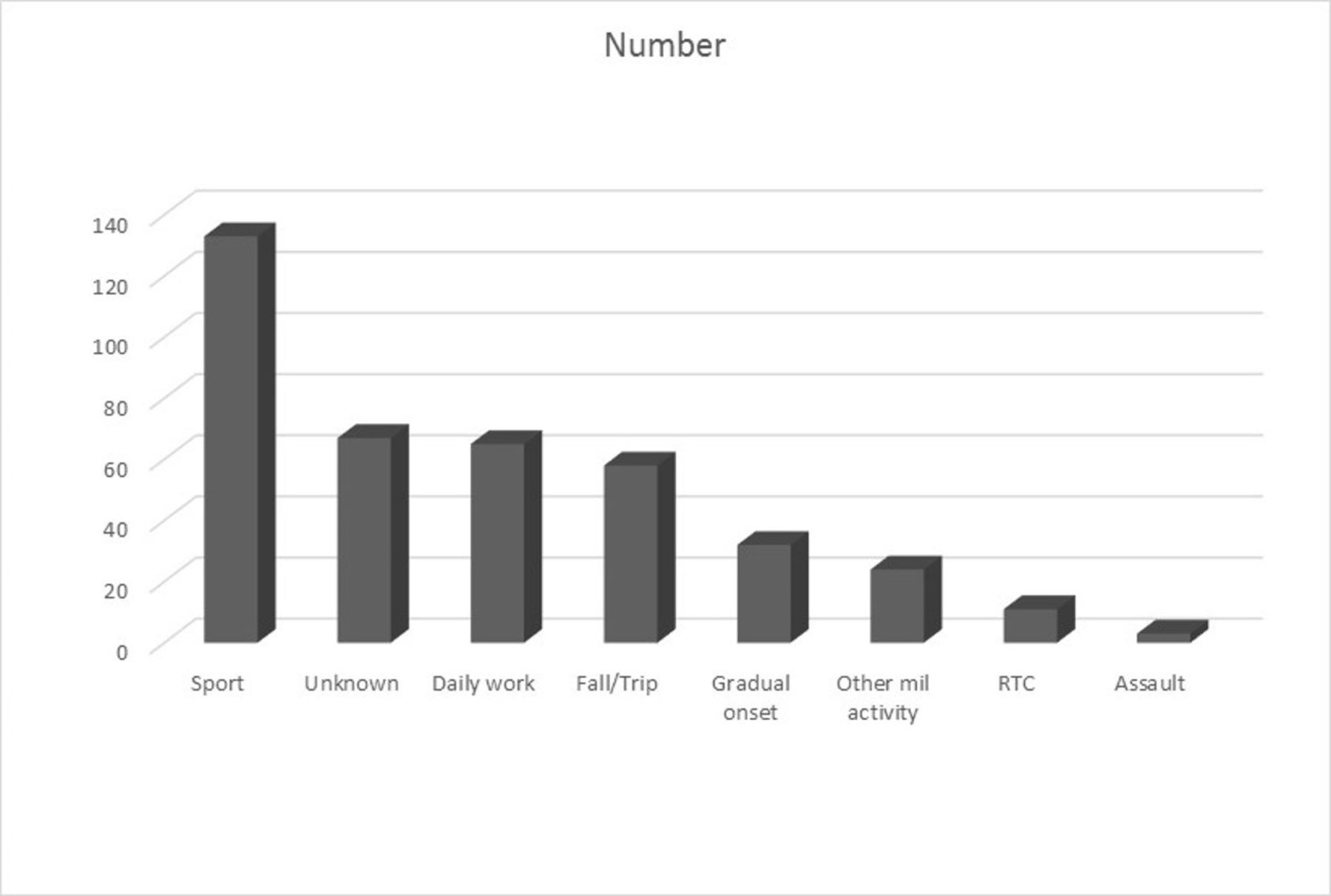
The most common identifiable cause of injury was sports or physical training. Figure 1 indicates the breakdown of injury presentations by causation.

{kind=link}
Injury presentations by causation.
Injury presentations
Table 3 shows the top five injury presentations: LBP (n=67), soft tissue UL injuries (n=40), disorders of the patella (n=39), traumatic knee injuries (n=34) and lower limb soft tissue injuries (n=31). Of these, 47.3% (n=186) were repeat injuries.
Presentations by common pathology
Timelines
The average wait for PCRF assessment was 8.3 working days, with 75.6% (n=297) being seen within the directed KPI of 10 working days. The average care pathway duration was 117.1 days. The average number of treatments per individual was 8.7 physiotherapy sessions (including hydrotherapy sessions) with a range from 0 to 127. Thirty individuals remained under PCRF care at 2 years. Of these individuals, 17.8% (n=70) were referred for hydrotherapy; 44% (n=173) received ERI interventions; 14.2% (n=56) required concurrent District Community Mental Health (DCMH) intervention; 28.5% (n=112) were referred to the specialist multidisciplinary injury assessment clinic (MIAC), and of these, 74.1% (N=83) were compliant with DDR best practice timelines. Only 2.9% (n=11) of individuals were referred to the Defence Medical Rehabilitation Centre (DMRC) at Headley Court.
Specific pathology
Table 4 outlines a breakdown of specific outcomes, duration and injury repetition by common pathology. Notable data is highlighted in bold.
Breakdown of specific outcomes by pathology
Outcomes
Of the total individuals, 58.3% (n=229) were occupationally fully fit (P2 MES) at 18 months. When including a P3 MES, this rose to 71.2% (n=280) of individuals returning to a potentially employable role. Of the total individuals, 7.6% (n=30) remained under active care (after 18 months to 2 years) and, in view of the long timelines, would be unlikely to return to full fitness. Reassuringly, 74.1% of care pathway timelines complied with BPGs. Based purely on FAA, 72% (n=283) were deemed fit for their primary role (FAA 1 or 2) on discharge, which almost exactly matches the relative MES of P2 or P3. Of all data, 15.3% were lost through administrative discharge, such as through DNA (or did not attend). As a result, effective return to duty rates directly following treatment ranged from 72% to 87.3%.
Gender-specific Outcomes
Table 5 indicates further specific outcome data broken down by gender.
Outcome data by gender
Discussion
As expected, the population investigated was almost entirely RN and RM in composition. The average age at 35.1 years was higher than would be expected in an equivalent army population (at 30 years), which could influence injury incidence.12 15 In this study, rank did not appear to affect presentation rates, with the proportion of presentations by rank approximately matching the overall RN population proportions. Women, however, were significantly over-represented at 18.1% of presentations compared with an actual RN population of 9.3%. These figures are likely to be higher as HMS Drake has a significant population of RM personnel and submariners, which have a few to no female personnel assigned. Female personnel also had a higher rate of concurrent DCMH attendance at 26.8% compared with 15.9% in male personnel. Furthermore, P2 rates at 2 years were significantly worse at 46.4% compared with 60.7% of men. These statistics appear to support the evidence of higher susceptibility to injury among female military personnel,12 14 16 but could also indicate their increased willingness to attend primary care facilities as needed.
Sport or physical training was the most common cause of injury followed by ‘unknown’. Closer scrutiny of the latter suggested much of this category comprised overuse injuries, which did not have a specific causation category. This could be indicative of ineffective or overloaded training regimes and deserves future investigation as it could offer a significant potential area for injury prevention strategies. Within this study, no specific measure of physical fitness was recorded; however, there has been much recent high-profile scrutiny regarding degrading RN fitness levels and rising obesity rates. Considering the close relationship between physical fitness and injury occurrence this could also be a key driver for future work in injury prevention.
Of the total injuries, 47.3% were a repeat of a previous injury, matching previous evidence that this is a significant predictor of further injury. These data were collected from the DMICP medical history, but no further detail was taken (such as time since previous injury episode or evidence of prior PCRF treatment). This could indicate individuals are either undergoing insufficient rehabilitation prior to upgrade or have not been sufficiently functionally tested prior to returning to work.
Overall injury timelines appeared satisfactory with a 74.1% adherence to BPGs. One hundred per cent adherence is not practically achievable due to the fluid nature of recovery pathways as patients may well appear to be progressing well then relapse. Equally, if an individual is not downgraded, it is not unusual for individuals to be deployed for periods, which takes them past the recommended timeline for further investigation. Although this study indicated a wait of 8.3 days for initial assessment with a 75.6% compliance rate with KPIs, it is felt this serves to highlight a DMICP data error; there is no option for recording the first appointment offered compared with when the individual attended. As a result, individuals can breach the KPI despite there being no waiting list at the PCRF (as is currently the case). The average care pathway duration was 117.1 days, with each individual requiring an average of 8.7 physiotherapy sessions. In view of the almost 50% reinjury rate, this may be insufficient, with individuals requiring longer in rehabilitation. Thirty individuals remained under PCRF care at 18 months and generally represented longer term surgical patients such as Anterior Cruciate Ligament (ACL) reconstructions. Relatively few patients were referred for hydrotherapy (17.8%) and ERI (44%). On review of the study period, it coincided with a time of high staff turnover, which may have led to staff retaining their patients in physiotherapy as opposed to moving them through to the ERI environment. Of the total patients, 14.2% (n=56) required concurrent DCMH intervention, which could indicate a possible relationship between mental health and pain presentations; however, care must be taken not to extrapolate this based off the simple data collected within this study. No investigation was made into the relationship between requirement for DCMH intervention and relative outcome and MES. Although 28.5% (n=112) were referred to MIAC, only 2.9% (N=11) individuals were referred to DMRC.
In line with previous studies, LBP was the most common presentation and was associated with a relatively poor outcome (56.7% attaining P2) and with the highest reinjury rates (71.6%). As may be expected, traumatic knee injuries had the worst return to full fitness (44.8%), required the most treatments (on average 11.2) and had long care pathway durations. It would be useful to examine this group in more detail as these include ACL reconstructions, which currently are regularly completed under the funded Fast Track scheme. Patellar tendinopathy also had particularly poor return to P2 rates (53.8%), which emphasises the challenge of treating this condition. Conversely, ankle injuries had good longerterm outcomes, with 80% at P2 MES at 2 years.
Summary
The PCRF was generally compliant with best practice direction with a minimum of 71.2% returning to an employable MES at 2 years. LBP has once again been highlighted as a significant problem in the military population. Reinjury rates have been highlighted as a significant issue within the Drake population, as has specific issues regarding injury occurrence, recovery and DCMH attendance in the female population.
Limitations
A key drawback of this study is that it is limited solely to the HMS Drake population; it is not yet possible to extrapolate these results across the defence population. It is highly likely that different services and trades have different injury profiles. Furthermore, this study highlighted the significant challenge of extracting meaningful data from within DMICP due to the problem of inaccurate data entry, injury coding and unreliability of electronic searches. This study had to be performed manually, which is highly time-consuming and subject to human error and bias. Ideally, DMICP should be able to perform such data analysis automatically and reliably.
Future work
It is necessary to repeat this study for the 2017 population to determine if these results represent true trends. In addition to the existing demographics, it should also include a physical fitness measure to attempt to determine if this has a relationship to injury occurrence and recovery. It would also be useful to examine reinjuries in further depth, particularly as to whether previous rehabilitation had been completed and to what level prior to reinjury. This would provide a gauge of the effectiveness of the rehabilitation process. It would also be more useful to use the Medical Deployment Standard as opposed to the P grade as a measure of effective employment, as this would more accurately reflect operational deployability. It is also necessary to expand this study into different service establishments to attain a true appreciation of the actual defence injury profile.
From this study, further work is already under way, focussing on both the specific RM and female populations to identify if these are higher risk populations to identify injury prevention strategies. The PCRF has also designed and instigated a trial functional assessment test to attempt to determine if individuals are fit to return to duty and will compare this against reinjury occurrence. Finally, closer scrutiny should be given to the relationship between PCRF attendance, concurrent DCMH involvement and outcome.
Data availability statement
Data may be obtained from a third party and are not publicly available.
Ethics statements
Patient consent for publication
Acknowledgments
The author wishes to thank the line management within Defence Primary Health Care (South West) for allowing the time to conduct and produce this study.
References
Footnotes
Contributors The author was the sole contributor to the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests The author is employed in the study location.
Provenance and peer review Not commissioned; externally peer reviewed.