Article Text

Abstract
Objectives There are no epidemiological studies comparing the prevalence of skin diseases between civilian and military populations. We sought to determine and compare the prevalence of skin conditions between civilian and military populations.
Methods A total of 3382 male patients (1148 military and 2234 civilian) were retrospectively and consecutively evaluated at Merzifon Military Hospital in the central Black Sea Region of Turkey.
Results The most frequent dermatological condition was tinea pedis (15.8%) followed by acne vulgaris, allergic contact dermatitis and alopecia areata in the military population (15.7%, 7.7% and 5.4%, respectively). Acne vulgaris, xerosis cutis and allergic contact dermatitis were the most common diagnoses in the civilian group (19.4%, 14.1% and 9.1%, respectively). The prevalence of tinea pedis, alopecia areata, pityriasis versicolor, ingrown nail (unguis incarnatus) and callus were statistically significantly higher in the military group (15.8% vs 4.4%, p<0.001; 5.4% vs 1.7%, p<0.05; 3.5% vs 0.7%, p<0.001; 3.3% vs 0.3%, p<0.001 and 4.6% vs 0.9%, p<0.001; respectively). Xerosis cutis was found to be significantly higher in the civilian group (14.1% vs 5.8%, p<0.001). Superficial fungal disease was the most prevalent disorder as in the previous literature.
Conclusions Preventive measures should be taken to improve the health of troops and reduce the prevalence of the common disorders such as tinea pedis, alopecia areata and callus. Troops should wear boots only when necessary in base camps. Clothing which reduces ventilation is not recommended. Depression and anxiety should be recognised and treated in soldiers with alopecia areata, as a solely dermatological approach without psychological support may reduce treatment success.
- DERMATOLOGY
- EPIDEMIOLOGY
- OCCUPATIONAL & INDUSTRIAL MEDICINE
Statistics from Altmetric.com
Key messages
Fungal infections and alopecia areata were statistically significantly more prevalent in the military than civilian groups.
Preventive measures should be taken to improve health of troops and reduce the prevalence of common disorders such as tinea pedis, alopecia areata and callus.
Multidisciplinary approach is required to reduce skin disorders.
Introduction
Epidemiological studies of skin diseases provide us with data regarding prevalence and demographic differences in affected groups. Epidemiological data are significant for investigating disease trends and planning healthcare programmes. Skin diseases are common in military populations and are responsible for 25% of all medical consultations by military personnel on deployments.1 ,2 There are 41 military hospitals in Turkey attached to the General Staff and a 2012 feasibility report regarding these hospitals opened them to civilians, although most military personnel were unsure whether they fulfilled the expectations of civilian patients or not. In 2013, a total of 300 000 civilian patients benefited from the military hospitals. The medical literature lacks reports comparing diagnoses between civilian and military patients evaluated in the same health institution. The aim of the present study was to determine the prevalence of skin diseases in a sample of civilian and military male patients at the Merzifon Military Hospital in the central Black Sea Region of Turkey.
Methods
The clinical and demographic data of all male patients presenting to our dermatology clinic in a 6-month period were evaluated retrospectively. Subsequent consultations of the same patient with the same diagnosis were excluded. Analysis of variance and Pearson's χ2 were used to measure expected and observed frequencies in the statistical analyses. p values of <0.05 were accepted as indicating statistical significance.
Results
A total of 3382 male patients were seen in clinic in the 6-month period as new presentations; 1148 were military with conscripts making up 43.9% and 2234 were civilian. There was no significant difference between the mean ages of the civilian (26.69±17 years) and military (26.04±8.36 years) patients (p=0.218).
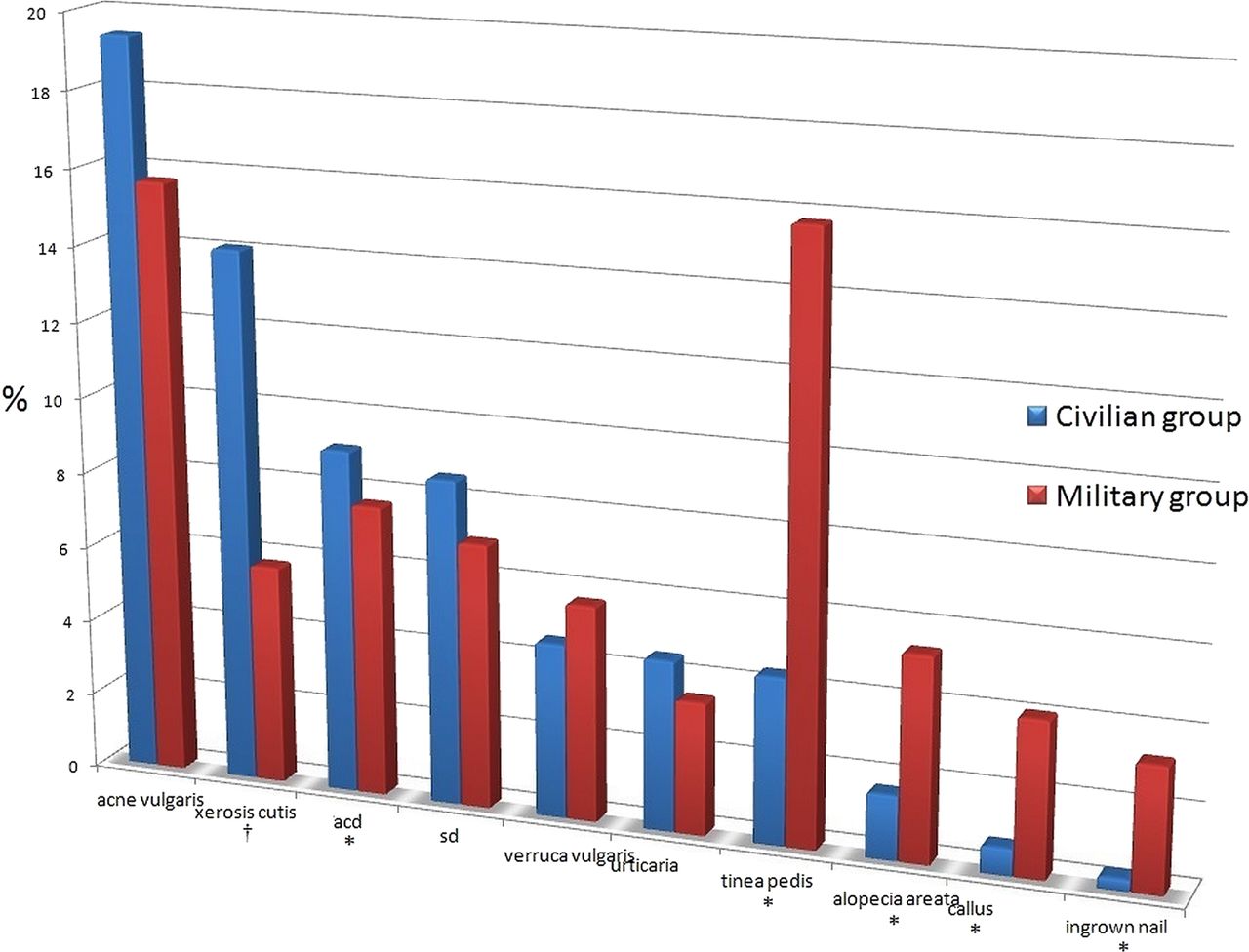
Tinea pedis was the most common skin disease in the military group (n=181, 15.8%), followed by acne vulgaris (15.7%) and allergic contact dermatitis (7.7%). The most frequent diagnosis in the civilian group was acne vulgaris followed by xerosis cutis and allergic contact dermatitis (19.4%, 14.1% and 9.1%, respectively) (Figure 1). The prevalence of tinea pedis, alopecia areata, pityriasis versicolor, ingrown nail (unguis incarnatus) and callus were statistically significantly higher in the military group (15.8% vs 4.4%, p<0.001; 5.4% vs 1.7%, p<0.05; 3.5% vs 0.7%, p<0.001; 3.3% vs 0.3%, p<0.001 and 4.6% vs 0.9%, p<0.001; respectively). Xerosis cutis was found to be significantly higher in the civilian group (14.1% vs 5.8%, p<0.001) (Table 1).
The distribution of dermatological diagnoses in civil and military groups
{kind=link}
Comparison of 10 most common diagnoses in both groups. *statistically commoner in military group, †statistically commoner in civilian group. SD, seborrheic dermatitis; ACD, allergic contact dermatitis.
Discussion
Only a limited number of studies provide data concerning the epidemiology of common skin diseases with the exception of skin cancer. Acne vulgaris was the most prevalent diagnosis (19.4%) in our civilian group and the second frequent disease in the military group (15.7%). Ertam et al3 reported that acne vulgaris was the most common disease with a higher prevalence (40.1%) in a Turkish patient group of which the mean age was 21.14±2.52 years. Plunkett et al4 also reported that acne was one of the most common diseases in an adult study population and the prevalence of the disease had a clear decrease with age from 42% in the age group of 20–29 years to 1.4% in the age group of 60–69 years. We hypothesised that xerosis cutis was the only diagnosis that was statistically commoner in the civilian group since this condition might be a neglected diagnosis in the military personnel.
Military personnel are prone to trauma due to the friction between the skin and their uniforms and skin diseases have been of major significance in military history. In World War I, 40.88/1000 men in British Army and 126.13/1000 men in French Army were admitted to hospitals for dermatological conditions.5 During World War II, 20% of all medical consultations were reported as being dermatological.6
Merzifon is a district of Amasya province of Turkey located in the central Black Sea region. Merzifon has Mediterranean climate with hot summers and cold and rainy winters. Exposure to high temperature and humidity, wetness and excessive sunlight can cause dermatological conditions varying from minor skin problems to debilitating diseases in military personnel.
Military personnel are most likely to be exposed to predisposing factors for dermatophyte infections including high ambient humidity and poorly ventilated footwear with insufficient aeration.7 Superficial fungal infections can produce severe outbreaks among military personnel in tropical climates. According to the US Army Medical Department's official history of medicine during the World War II, only 6% of soldiers evaluated in dermatology clinics were diagnosed with superficial fungal infections in Virginia with temperate climate although the incidence was higher (22%) in the Mediterranean theatre of war.8 Fungal infections were found to be the major dermatological conditions in the East Timor deployment of Australian troops with fungal skin infections occurring in more than 50% of deployed troops.7 Djeridane et al9 reported the prevalence of tinea pedis to be 18.3% among Algerian military personnel and higher than that in the Algerian general population (15%), and other studies10 like ours confirm tinea pedis to be the most frequent dermatological diagnosis. Fungal infection was determined as the major dermatological disorder (28%) in military conscripts in Singapore.11
Viral infections can cause outbreaks on military deployments.12 In tropical and sub-tropical climate, oral herpes infections and genital warts can relapse frequently.1 We found no difference in the prevalence of viral infections between both groups.
Selvaag reported that allergic and irritant contact dermatitis, acne vulgaris and sexually transmitted disease were the most prevalent skin diseases in military personnel (34.2%, 15.3% and 10.3%, respectively).13 Similarly, eczematous dermatitis was the most common disorder with a frequency of 17% in a deployed dermatology clinic in Iraq.14
In this study, pityriasis versicolor was more common in military personnel than in the civilian group (3.5% vs 0.7%, p<0.001); the prevalence of pityriasis versicolor was 2.1% in Italian sailors, 68% of whom were not aware of their disease or even their skin lesions. No association was found between pityriasis versicolor and sporting activities or marching.15 Alopecia areata was the diagnosis in 5.4% of military personnel, which was significantly higher than in civilians: the rate was 2.1% in a military study from Saigon, Vietnam, in 1967.8
Since fungal infections are the most common disorders causing disability among troops, preventive measures should be taken. Troops should wear socks and boots only when required in base camps in such Mediterranean climates. Shower thong and mesh socks are recommended. Dry cotton mesh socks should be included in resupply. Wearing underclothes while on operations may reduce ventilation of the skin. Troops should be discouraged from wearing underclothes.16 Environmental interventions such as routine disinfection of communal showers and reduction of communal laundering of socks should be planned.7 ,17 Frequent air drying and powdering of the feet with tolnaftate or foot powder including 83% talc, 10% starch and 3% salicylic acid may be effective preventive measures.7
Alopecia areata may be a result of psychological conditions such as alexithymia, anxiety and depression. Emotional problems should be investigated and treated in soldiers with alopecia areata and a multidisciplinary approach is required to reduce such skin disorders. A solely dermatological approach without physiological support may reduce treatment success. On retrospective analysis, 24% of the military personnel with alopecia areata were referred to a psychiatry clinic and 16% of these were initiated on anti-depressant therapy.
Our study has one limitation that we evaluated the patients retrospectively. A prospective approach to associations, possible causes and risk factors should be focused on in further studies.
Conclusions
Physicians should be aware that since military personnel face different environmental conditions from civilian people, certain disorders such as tinea pedis, callus and ingrown nail affect them more frequently. A multidisciplinary approach, preventive interventions and educational programmes can reduce loss of labour and health spending on the military personnel.
Acknowledgments
We would like to thank Ibrahim Kahyalar, Mustafa Gürkan, Özkan Özkul and Hüseyin Küpeli for the data entry for the statistical analysis and Dr. Emrullah Solmazgül for the assistance.
References
Footnotes
Contributors EŞ: planning; MS: data collecting; SDŞ: analysis. All the authors are responsible for the overall content.
Funding None.
Competing interests None.
Patient consent Obtained.
Ethics approval Gulhane Military Medical Academy Ethics Committee, Ankara, Turkey.
Provenance and peer review Not commissioned; externally peer reviewed.