Article Text

Abstract
Atrial fibrillation (AF) is the most common sustained atrial arrhythmia, and increases an individual's risk of morbidity and mortality from cardiovascular and thromboembolic events. In this article, we review the pathophysiology and clinical presentations of AF and describe appropriate investigations and management likely to be appropriate for a military population, in line with current National Institute for Health and Care Excellence and European Society of Cardiology guidelines. The implications for the individual's Medical Employment Standard in the UK Armed Forces, with specific reference to specific military occupational activities such as aviation, diving and driving occupationally, are also reviewed.
- OCCUPATIONAL & INDUSTRIAL MEDICINE
- AVIATION MEDICINE
Statistics from Altmetric.com
Key messages
Atrial fibrillation is the most common sustained arrhythmia seen in the Armed Forces, and its incidence increases with age.
The optimal management plan should be individually tailored, but catheter ablation will often play a role in maintaining sinus rhythm.
All personnel will be medically downgraded for assessment and management; some specialist groups will remain restricted despite cardioversion.
Introduction
A 38-year-old Royal Marine Sergeant presents to the medical centre with fatigue, breathlessness and palpitations since waking from sleep 2 days before. He is, otherwise, healthy, and has been a keen footballer and triathlete for 20 years. The night before his symptoms appeared, he was intoxicated with alcohol at a formal dinner. He admits to normally drinking 30 units of alcohol weekly. On examination, his BP is 124/80 mm Hg, and his pulse is fast and irregular. An ECG shows atrial fibrillation (AF) with a ventricular response of 120–140 bpm.
Atrial fibrillation (AF) is the most common sustained cardiac arrhythmia,1 with an estimated prevalence of 36.5 million individuals worldwide.2 In Western adults aged <55 years, the prevalence is estimated at 0.1%,3 and is associated with thromboembolic disease and exacerbations of heart failure.4 In the general population, the risk of death in individuals with AF is increased twofold as a result of underlying disease or complications related to the arrhythmia. Within military populations, morbidity and mortality from AF may be less common; however, from an occupational standpoint, the diagnosis may be career-limiting as there are specific standards of medical fitness required to work within different military occupations. Indeed, there are discharges on medical grounds within the UK Armed Forces every year as a result of this diagnosis5 as AF and its treatments impact military employment.
Few publications examine the impact of AF in a young, fit population such as the UK Armed Forces. This article reviews the clinical presentations of AF, and comments on the occupational and lifestyle implications for military personnel. It also describes investigations and management likely to be appropriate for the military population, in line with current National Institute for Health and Care Excellence (NICE) and European Society of Cardiology guidelines. The implications of the individual's Medical Employment Standard (MES) in the UK Armed Forces, with specific reference to military occupational activities such as aviation, diving and driving occupationally such as fork-lift trucks or Driver and Vehicle Licensing Agency Class 2 licensed vehicles such as large goods vehicles, are also reviewed.
Pathophysiology
AF is a pathological cardiac rhythm caused by competing sources of electrical activation in the atria of the heart. These result in disordered atrial activity where the atria ‘fibrillate’ rather than contract in a coordinated and uniform manner.6 In the normal heart, electrical activation is initiated at the sinoatrial node within the right atrium, activation then spreads to the right and left atria and results in atrial contraction (atrial systole), which corresponds to the P wave on the surface ECG. Conduction progresses slowly through the atrioventricular node located in the interatrial septum before it passes through to the ventricular myocardium, to trigger ventricular systole corresponding to the QRS complex on the ECG.
To develop AF, there must be a trigger to initiate the rhythm and a substrate to maintain it. Triggers include stimulation from the sympathetic or parasympathetic nervous system, bradycardia or tachycardia, accessory atrial–ventricular pathways, acute atrial stretch (eg, due to acute mitral regurgitation), and ectopic foci within the tissue surrounding the pulmonary veins.7 These result in competitive impulse initiations, arising in areas of the atria other than the sinoatrial (SA) node or altered transmission of the action potential across parts of the atrial tissue. As a consequence, individual muscle fibres contract in response to the multiple stimuli at a high frequency.6 Not all of these impulses will be transmitted to the ventricle; hence, on the ECG, the P waves are absent, and QRS complexes occur at irregular intervals (Figure 1).

ECG showing atrial fibrillation.
In individuals without structural heart disease, AF will commonly manifest as self-terminating paroxysms, resulting in paroxysmal AF (PAF) (Table 1).8 ,9 A substrate is needed for AF to persist, although this may not be specifically identifiable in clinical practice.
Both parasympathetic and sympathetic nervous system activation can cause AF. In small studies of human subjects, and in animal models, alterations in vagal tone have been linked to the development of PAF in otherwise healthy subjects.10 ,11 It is thought that chronic increases in vagal tone, as seen in endurance athletes, contribute to the development of AF in this group.12
An important substrate associated with AF is atrial fibrosis,13 which may be mediated by chronic activation of the rennin–angiotensin–aldosterone system found in congestive heart failure, ischaemic heart disease, hypertension and structural heart disease.1 However, atrial fibrosis has also been found at biopsy in healthy individuals diagnosed with ‘lone AF’ (AF without any apparent underlying structural heart disease).9 ,10 Another key factor in the development of AF is stretch of the atrial myocardium caused by increased haemodynamic load; for example, left atrial stretch caused by mitral regurgitation.7 ,8 During the first few minutes of AF, the atria begin remodelling, which creates a substrate for further AF. In a normal heart, stretch of the atrial myocardium may stimulate remodelling within 30 min. Thus, ‘AF begets AF’, and without treatment, the patient will progress from PAF to persistent AF (Table 1). Eventually, the remodelling becomes irreversible, and the patient has permanent AF, which cannot be terminated by cardioversion.1 ,9
UK Armed Forces population
The UK Armed Forces are predominantly young, with only 0.14% aged >55,14 and common risk factors for AF among the general population (hypertension, coronary artery or structural heart disease and diabetes) are relatively uncommon.1 ,15 Thirteen per cent of US service personnel have been shown to have hypertension16; a rate that is likely to be similar in the UK Armed Forces. Diabetes is uncommon in the UK Armed Forces, as it often results in medical discharge. It is difficult to quantify the incidence of coronary heart disease and structural heart disease in serving UK Armed Forces personnel, but recent data show that ischaemic heart disease is the most frequent individual cause of death due to disease in the UK Armed Forces (3.9 per 100 000 per year).5 Due to screening at entry and the young age of the military population in general, valvular heart disease is likely to only be associated with AF in a minority of cases. Hyperthyroidism commonly triggers AF, which can be the first indication of the underlying disease; appropriate management of the thyroid disease is key to managing the arrhythmia.
Structural abnormalities, cardiomyopathies and abnormalities of conduction such as Brugada syndrome, Wolff–Parkinson–White syndrome and long-QT syndromes can predispose younger patients to develop AF.17 While these are uncommon, the onset of AF may be the trigger for the diagnosis of these important conditions. Medical officers should consider the possibility of structural and electrical heart abnormalities in a young service person presenting with AF.
Lifestyle factors, such as a high body mass index (often with sleep apnoea) and chronic alcohol intake (>4.5 units/day) may also contribute to the development of AF.18 A recent study of currently serving personnel found that levels of obesity were low in those aged <25, but increased significantly in those >35, with a prevalence of ∼25%.19 Alcohol intake within the UK Armed Forces is consistently reported as higher than that in comparable civilian groups, with higher rates of heavy episodic or ‘binge’ drinking.20 ,21 Illicit drug use (eg, cocaine) is associated with AF though this is likely to be less of a problem in the military compared with that of the general population.
An occupational hazard?
Participation in regular exercise is both an occupational and cultural expectation in the UK Armed Forces, and many military personnel participate in endurance sports both within military teams and outside of work. Lone AF is more common in veteran endurance athletes, and it is hypothesised that this is due to endurance exercise inducing atrial fibrosis.22 However, merely participating in endurance exercise for many years may cause other anatomical (eg, left ventricular hypertrophy) and physiological changes in the heart that act as a substrate for AF, echocardiography demonstrates dilatation of cardiac chambers, including the atria, and is associated with increased vagal tone and bradycardia.12 Additionally, there is evidence that intense physical training can lead to chronic systemic inflammation while a chronically elevated C-reactive protein (CRP) is predictive of AF.23 Overall, 40% of athletes presenting with AF will be diagnosed with a specific underlying substrate for AF such as an accessory pathway, cardiomyopathy or myocarditis.24
Flight, even within commercial aircraft, alters the physiology of both pilots and passengers. Like their civilian equivalents, military multiengine transport aircraft, such as the Airbus A330 Voyager aircraft, are pressurised to an equivalent altitude of 6000–8000 ft (1524–2438 m), with a corresponding decrease in the partial pressure of oxygen.25 This results in a degree of mild hypoxia, accompanied by an increase in RR, BP and HR; physiological responses that are usually of no consequence in a healthy population.26 In patients with AF however, these have the potential to result in decompensation during a pre-existing cardiac arrhythmia, and may precipitate arrhythmias in susceptible subjects. Hypoxia may trigger or exacerbate AF, and some drug therapies (particularly beta blockers) may prevent cardiovascular compensatory mechanisms from occurring.
Exposure to acceleration (+Gz), both in a centrifuge and when performing +Gz manoeuvres in air combat manoeuvring, is well recognised to induce a variety of cardiac arrhythmias. While these are most commonly benign, more dangerous arrhythmias such as ventricular tachycardia and AF have been reported.27–29 Military aviation may, therefore, trigger AF in an individual with predisposing factors. This may result in distraction or incapacitation, which may have significant consequences if they occur during key stages of flight.
Military diving
Military diving is physically and physiologically demanding, involving depths of up to 60 m. Once underwater, divers face additional tasks such as explosive detonation, surveillance and construction.30 ,31 Cold water immersion is known to induce bradycardia in healthy individuals,32 and in extremely cold environments, arrhythmias, including AF, can be precipitated even in healthy individuals.33 Subjects known to have AF may develop ventricular tachycardias when diving34; hence, a career in military diving creates physiological conditions that may favour the development of AF in predisposed individuals. Diving in those with known AF may expose them to more malignant arrhythmias, and is, therefore, an exclusion criterion for diving. ECG screening for military aircrew and divers is performed at selection and with increasing frequency with age.
Presentation and investigation
The medical officer (MO) seeks telephone advice from a cardiologist who advises the initiation of bisoprolol 2.5 mg daily. This is subsequently increased to 5 mg on review by the MO the next day. A cardiology outpatient appointment is arranged, and the marine is downgraded by the MO to Medically Non-Deployable (MND), temporary (Medical Employment Standard (MES) A4L4M3/4E3) to modify employment and ensure availability for clinical management. The full blood count, CRP, urea and electrolytes, liver function and thyroid function tests are all normal. In outpatients, a transthoracic echocardiogram demonstrates a structurally and functionally normal heart, and a 24 h ambulatory ECG demonstrates AF with a ventricular rate of 52–90 bpm throughout the recording.
AF may be asymptomatic or present only as fatigue.9 ,18 Palpitations are a common and often distracting feature; other symptoms of AF result from a reduced cardiac output and include dizziness, chest pain, reduced exercise tolerance and dyspnoea. Diagnosis is confirmed by detecting the typical 12-lead ECG characteristics of absent P-waves and irregular QRS complexes characteristic of AF (Figure 1). PAF may be difficult to confirm if the patient has returned to sinus rhythm (SR) when examination and ECG are performed. Those suspected of having PAF should undergo 24 h ambulatory ECG monitoring if symptoms occur on a daily or almost daily basis (Figure 2). An ‘event recorder’ ECG should be requested for those with symptomatic episodes >24 h apart. If the trigger for AF is clearly identified from the history, for example, exercise, then these conditions may be reproduced to help trigger the arrhythmia.
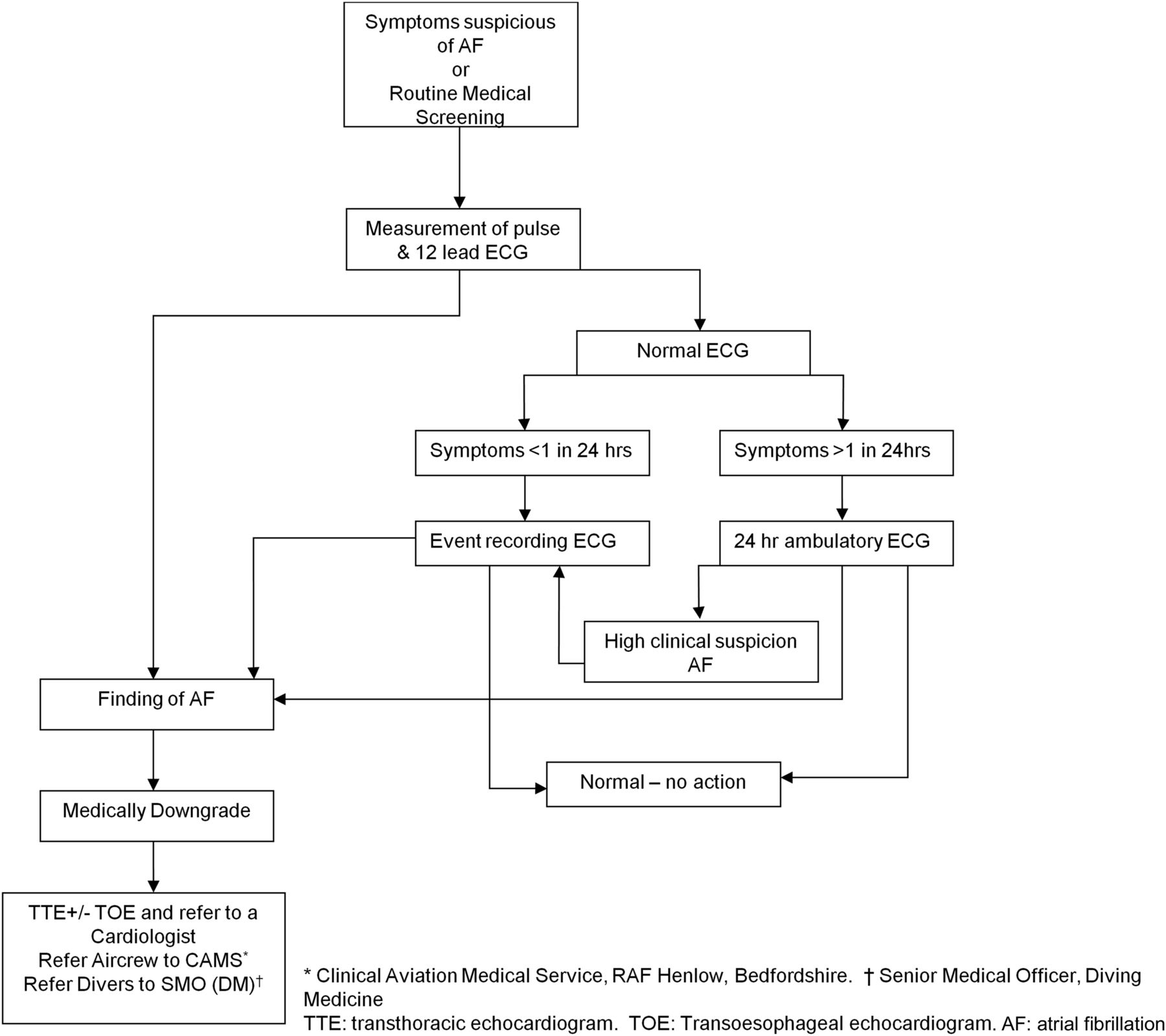
Pathway for UK Armed Forces personnel suspected to have AF.
On confirming AF, NICE guidelines state that transthoracic echocardiogram (TTE) should be performed on patients who are appropriate for cardioversion, suspected of having underlying structural heart disease or in need of a TTE to plan long-term management or anticoagulation.9 In the younger military population, all personnel diagnosed with AF will need a TTE to exclude structural heart disease. A structurally normal heart is a requirement for return to a less restrictive MES in most military occupations (Figures 2 and 3).35–37

{kind=link}
{kind=link}
{kind=link}
Management pathway for UK Armed Forces personnel diagnosed with AF.
Management
AF may be rhythm or rate controlled. While this should always be determined on a case-by-case basis, in general, patients with de novo AF, without underlying cardiovascular disease, should be considered for pharmacological or electrical cardioversion to attempt to return them to SR. Patients who have underlying cardiovascular disease, and those who have been in AF for a significant time, may be considered for rate control. All patients should be considered for anticoagulation9 ,38 using the CHA2DS2-VASc scoring system. This scoring system calculates the likelihood of thromboembolic events in patients with AF based on age, gender and comorbidities.39
Current NICE guidelines state that electrical, rather than pharmacological, Direct Current cardioversion (DCCV) should be offered to patients with AF persisting >48 h. After 48 h of AF, anticoagulation cover should be given for at least 3 weeks prior to DCCV, unless guided by transoesophageal echocardiography (TOE) at the time of the procedure. In those patients with AF refractory to initial attempts at DCCV or who revert to AF soon after, amiodarone may be used to increase the chances of successful cardioversion and subsequent maintenance of SR. Due to the side-effect profile of amiodarone, long-term administration should be carefully considered in the military population, and catheter ablation is likely to be the preferred alternative in such cases. For those with a high likelihood of AF recurrence, long-term drug treatment may be considered necessary in order to maintain SR. In this instance, standard beta blockers should be the first choice, unless there are specific contraindications to their use.
In those with infrequent PAF, with a structurally normal heart, a ‘pill in the pocket’ approach may be appropriate, using agents such as flecainide and a beta blocker.9 This requires patients to have a clear onset of symptoms, and to be able to take the medication within a relatively short time of the onset of AF. Antiarrhythmic drugs, such as flecainide, are contraindicated in patients with ischaemic or structural heart disease.
Personnel who cannot be successfully cardioverted or maintained in SR, those who have refractory symptoms despite medical therapy or those with left ventricular impairment due to AF should be considered for catheter ablation.9 ,40 Catheter ablation identifies and targets foci for AF arising within the ostia of the pulmonary veins, and isolates these from the atrium using radiofrequency ablation though cryotherapy, ultrasound or laser ablation may also be used. Radiofrequency energy applied directly to the myocardium generates heat and causes necrosis and scarring of the affected tissue. Cryoablation, where extreme cold is used instead of heat, is also effective.37 Scarring electrically isolates the four pulmonary veins from the atria, preventing the transmission of competitive electrical activation that triggers AF. Generally accepted success rates for AF ablation are 50%–70% after a first procedure and 80%–90% after a second.41
Although potentially curative, catheter ablation carries small, but significant, risks of thromboembolism and stroke, cardiac tamponade and death, and its use for purely occupational reasons should not be undertaken lightly, and should be discussed fully with the patient. In those with symptoms refractory to medical therapy or when left ventricular dysfunction results from AF, ablation remains an entirely appropriate treatment option.
When a rate-control strategy is deemed to be appropriate, first-line agents for AF are rate-limiting calcium channel blockers (such as diltiazem or verapamil) or beta blockers; these may also be appropriate for military personnel. Consideration should be given to the use of only approved drugs in those in specialist groups, such as aircrew, only where this does not result in substandard treatment. A combination of two agents (eg, beta blocker and diltiazem) may be used for resistant symptoms. Digoxin monotherapy is reserved for sedentary patients, and would be rarely indicated in the military population.
The risk of distraction and incapacitation due to AF is incompatible with an unrestricted MES. It is likely that military personnel will be subject to significant occupational restrictions if they are not cardioverted,35 and some of these restrictions may persist in specific groups even when SR is restored. Cardioversion should be achieved according to normal guidelines.
A ‘pill in the pocket’ approach may be a useful treatment strategy among military personnel with a low AF burden. For deployments or detachments to appropriately risk-assessed roles, personnel would not require resupply of medication as they can deploy with a plentiful supply for their likely needs, placing little dependence on the logistic chain. Consideration must be given to the potential need for access to medical care, should pharmacological cardioversion not be achieved.
Anticoagulation
Potentially, the most harmful consequence of AF is the formation of thrombus in the left atrial appendage (LAA) of the heart. The LAA is a finger-like outward projection of the left atrium, and when made non-contractile due to AF, abnormal pooling of blood can occur here, with subsequent thrombus formation and embolisation, which may result in an embolic stroke. Patients presenting with AF of >48 h duration should be anticoagulated for at least 3 weeks prior to cardioversion to minimise the risk of embolic stroke at the point that SR is restored. Alternatively, the patient may undergo TOE-guided cardioversion to exclude thrombus in the LAA if more rapid cardioversion is required due to haemodynamic compromise or LV dysfunction. Although TOE is a safe procedure in skilled hands, it does carry risks of aspiration pneumonia, dental trauma and a small risk (approximately 1:1000 cases) of oesophageal perforation; hence, TOE-guided cardioversion should only be undertaken when clinically indicated.
Those who are managed with a rate-control strategy should be considered for anticoagulation according to their risk of stroke, using the CHA2DS2-VASc scoring system (see Table 2),39 which should be balanced against bleeding risk. Bleeding risk may be assessed using the HAS-BLED scoring system, which estimates the risk of major bleeding based on age, comorbidities, alcohol and drug use and concurrent.42 Anticoagulation in this cohort may be with warfarin or with one of the licensed novel oral anticoagulants (NOACs), such as rivaroxaban, dabigatran or apixaban.
Patients anticoagulated with warfarin require regular international normalise ratio (INR) monitoring to ensure that they are within the therapeutic range, while NOACs do not require level monitoring and have short half lives, but are not easily reversible should the need arise, whereas warfarin is more easily reversed when required.
Occupational impact
Individuals should always be treated with optimal therapy on medical, and not purely occupational, grounds. This must particularly be borne in mind when specific treatments carry significant procedural risks. As a minimum, personnel with AF should be made unfit service outside base areas (peacetime access to civilian or military hospital) in the first instance. Aircrew and air traffic controllers must be made unfit flying/controlling duties, and referred for specialist assessment at the Clinical Aviation Medicine Service.
Service personnel with a single episode of AF, with a structurally normal heart and no evidence of ischaemia, may return to an unrestricted MES after a period of 2 years in SR, without medication. Following AF ablation, personnel must be in SR for 2 years (with no structural heart disease) in order to regain an unrestricted MES.34 Aircrew and air traffic controllers will not regain an unrestricted MES, regardless of the outcome of AF treatment, but may be permitted to fly in a multicrew environment or control with a proximity controller. Table 3 shows the likely restrictions on MES according to type of AF and military role.
Occupational consequences of treatments for AF
The medical treatment of AF contributes to a restricted MES being awarded, and this especially applies to anticoagulation. The bleeding risk as well as the need for monitoring makes warfarin incompatible with service outside base areas (usually MND, E3 (UK only)); warfarin is incompatible with flying duties. No specific guidance is yet available on the use of NOACs in the UK military setting. The inability to reverse them as well as the associated bleeding risk makes it unlikely that personnel on NOACs would be fit for service outside base areas, except on low-risk short deployments/detachments following a thorough risk assessment. They are highly unlikely to be compatible with flying. Management with rate-limiting drugs may affect an individual's tolerance to cold, exertion and +Gz.
Rate or rhythm controlled AF, including the intermittent treatment of PAF, will require a continuing restriction of MES to base areas and deployability at either Medically Limited Deployability or MND.
Following 3 weeks of continuous therapeutic anticoagulation, an elective direct current (DC) cardioversion successfully returns him to sinus rhythm. His MO gives him lifestyle advice, and, in particular, he stops binge drinking. He is followed up by his Single Service Occupational Medicine board, but occupationally, he remains non-deployable. After 2 years of monitoring, during which he has no further AF episodes, he is medically upgraded to medically fully deployable (MFD) with an L2 MES marker. As this monitoring period exceeded the 18 months allowed for temporary gradings (12 months in the Army), the Medical Board advised the Employment Board of the likelihood of upgrading.
Conclusion
AF is a common arrhythmia with the potential to be distracting and incapacitating. Although AF is associated with increasing age, it may still be seen within the UK Armed Forces where the occupational consequences may be highly significant. Full assessment of these patients is mandated, in order to look for potential underlying causes and to help plan optimal treatment. Restoration of SR will be the aim in almost all personnel, and catheter ablation may be appropriate in order to achieve this. When long-term medication is required, this needs to be considered in the context of an individual's branch or trade. A restricted MES will be required in all personnel for initial assessment and management, particularly with anticoagulation, and restrictions may not be removed until SR has been restored for a significant period. Aircrew and air traffic controllers will remain restricted, despite successful cardioversion. Specialist divers will continue to be assessed on a case-by-case basis.
Acknowledgments
With thanks to Dr Foster Crawford, Institute of Naval Medicine, Portsmouth.
References
Footnotes
Contributors AHH: first author, responsible for overall content, drafting and revision of content, and submission. ATC: critical review of content, editing style and content for cardiological accuracy. JD’A: specialist military cardiology and occupational advice and review of content. MR: specialist military occupational advice and review of content. AJC: senior author and atrial fibrillation expert, review of content.
Competing interests None declared.
Provenance and peer review Commissioned; internally peer reviewed.