Article Text

Abstract
Introduction Defining the minimum anatomical structural coverage required to protect from ballistic threats is necessary to enable objective comparisons between body armour designs. Current protection for the axilla and arm is in the form of brassards, but no evidence exists to justify the coverage that should be provided by them.
Method A systematic review was undertaken to ascertain which anatomical components within the arm or axilla would be highly likely to lead to either death within 60 min or would cause significant long-term morbidity.
Results Haemorrhage from vascular damage to the axillary or brachial vessels was demonstrated to be the principal cause of mortality from arm trauma on combat operations. Peripheral nerve injuries are the primary cause of long-term morbidity and functional disability following upper extremity arterial trauma.
Discussion Haemorrhage is managed through direct pressure and the application of a tourniquet. It is therefore recommended that the minimum coverage should be the most proximal extent to which a tourniquet can be applied. Superimposition of OSPREY brassards over these identified anatomical structures demonstrates that current coverage provided by the brassards could potentially be reduced.
- TRAUMA MANAGEMENT
- VASCULAR MEDICINE
Statistics from Altmetric.com
Key messages
Defining the minimum anatomical structural coverage required to protect from ballistic threats is necessary to enable objective comparisons between body armour designs.
Haemorrhage from vascular damage to the axillary or brachial vessels was demonstrated to be the principal cause of mortality from arm trauma on combat operations.
Peripheral nerve injuries are the primary cause of long-term morbidity and functional disability following upper extremity arterial trauma.
The minimum coverage of arm protection inferiorly should be the most proximal extent to which a tourniquet can be applied.
The coverage provided by current arm protection used by UK forces could potentially be reduced in size thereby improving heat dissipation and comfort.
Introduction
Body armour is a type of personal protective equipment designed to protect soldiers from injury on the modern battlefield. Since its original inception in its most modern form in the 1950s,1 body armour design and development have been an iterative process. Individual components have been designed to respond to particular evolving threats, with recent examples being the Pelvic Protection System2 and the Patrol Collar.3 The resultant armour often has elements that have been developed separately and when worn as a complete system may not therefore be optimised in terms of integration and interoperability; an additional consequence is that it can result in overlaps or lack of coverage.
The aim of the VIRTUS project is to procure the personal protective equipment that will be worn by the UK armed forces in future conflict. It will be a fully integrated system and based upon objective evidence for which anatomical structures require protection. As such, a prospective review of which anatomical components within each body area that require protection is being undertaken, with multidisciplinary consensus groups having already agreed on areas of coverage for both neck3 and head4 protection.
Damage to vascular structures within the arm and axilla from ballistic projectiles is responsible for a significant mortality on modern combat operations.5–8 Arresting such junctional bleeding can be challenging due to difficulties in both providing direct compression as well as surgical access (Figure 1). The re-emergence of tourniquets in providing immediate haemostasis has been associated with significantly reduced mortality8 ,9 but their use is limited by how proximal they can be placed.10 For vascular injuries closer to the trunk, packing novel haemostats into the wound, followed by direct pressure from a first field dressing, remains the extent of currently available care in the prehospital setting. The only method of definitely controlling bleeding for these wounds is surgical.11 Such access, usually through a thoracotomy requires highly specialised medical knowledge and has a poor success rate in the prehospital setting.5 Therefore, in order to reduce the mortality, primary prevention or mitigation of axillary vascular injuries is required.
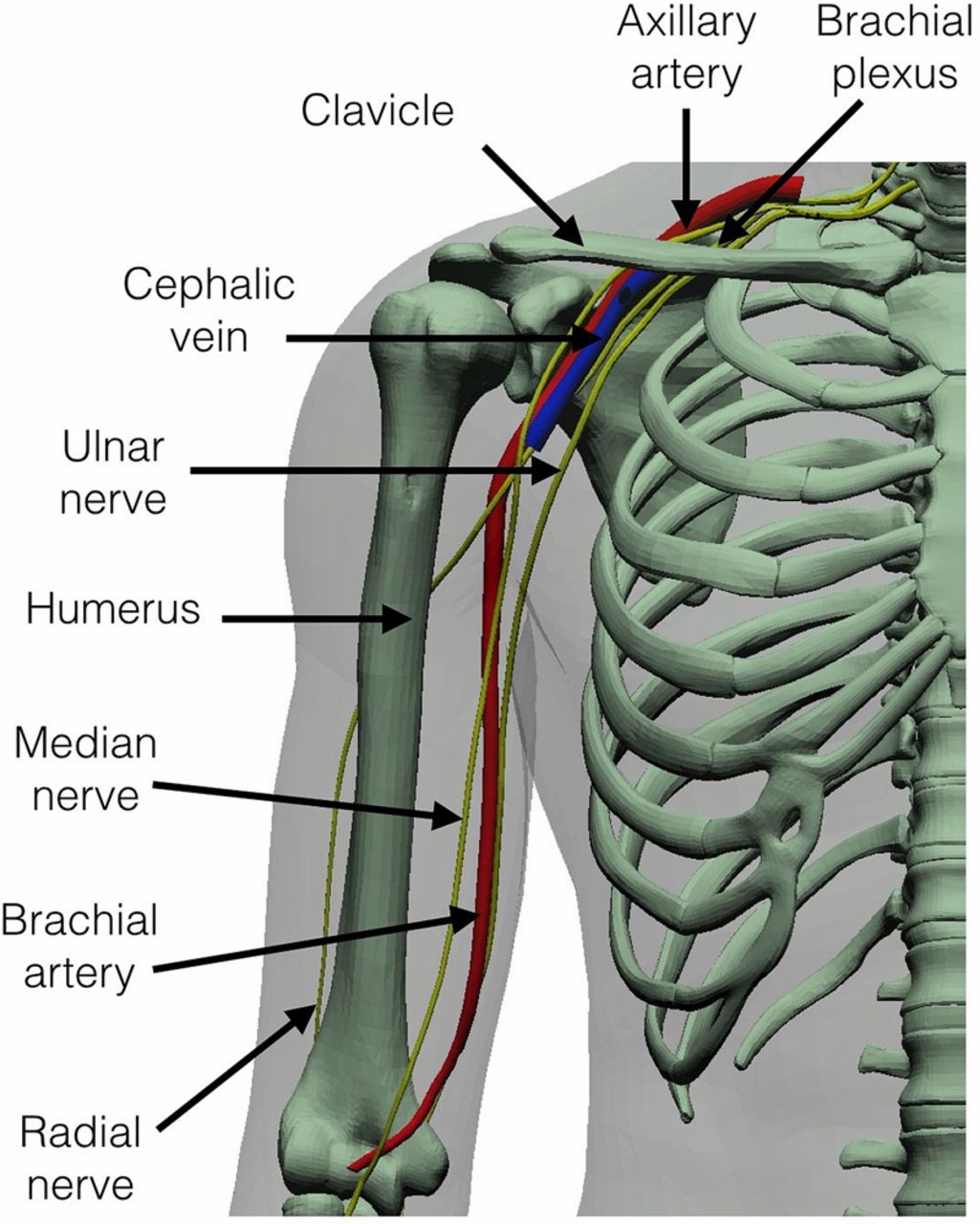
Potentially vulnerable structures within the arm and axilla shown within a three-dimensional representation of human anatomy.
Existing ballistic protection designed to prevent arm and axilla injuries
The OSPREY body armour system, introduced into service in 2006, was the first UK body armour system that included specific protection of the arm and axilla against explosively propelled fragments (Figure 2). All generations of OSPREY have since used the same design of detachable protection that can be secured to the body armour vest. The brassards are designed to be used in conjunction with an additional shoulder guard that is attached to the rear. It is believed that the wearing of OSPREY brassards by UK soldiers deployed in Afghanistan was disliked due to the perceived thermal burden on the wearers and the perceived reduction in agility; but little evidence exists as to their true uptake. A 3.5-month review of all UK soldiers treated in Camp Bastion in 201212 demonstrated that none of 38 were wearing their brassards at the time of their injury, although their use may have been limited by the role that the soldier was performing at the time of injury.

A close up of Mark 4 OSPREY system to demonstrate the coverage provided by the brassard (A) and shoulder guard (B) from the front and rear.
The KESTREL body armour system is the only other body armour system issued to UK forces that has included arm protection, with the exception of specialist Explosive Ordnance Disposal suits. KESTREL was only issued for a limited period (2006–2007), specifically to provide increased protection in static positions such as sentry duty or top cover.1 Both versions of KESTREL (Marks 1 and 2) incorporated a single fixed piece of soft body armour covering the thorax, arms and neck (Figure 3).

The Mark 2 Kestrel body armour demonstrating the fixed arm and neck collar portions.
Arm protection has been available to US forces since the interceptor system was introduced in the 1990s.1 The US Army and Air Force replaced interceptor with the Improved Outer Tactical Vest (IOTV) in 2007, which in all its iterations have included a detachable Deltoid and Axilla Protector (DAP) on each side (Figure 4). This is similar to the brassard component of OSPREY but without the additional shoulder guards. The US Marine Corps in comparison replaced interceptor with the modular tactical vest in 2006 (and in 2013 the improved modular tactical vest). In an attempt to reduce the burden on the dismounted soldier, one of the alterations was to not include arm protection. Greer et al12 interviewed 48 US soldiers with upper arm injuries sustained in Iraq about the DAPs issued with their interceptor body armour, only two of 48 stated that they had been issued with DAPs, one of whom stated that it was not worn at the time of injury due to discomfort. No other information has been described in the literature about arm protection used by other nations. When compared on anatomical mannequins, the coverage provided by the UK OSPREY and the US IOTV arm protection is similar, reaching to just above the elbow, but the anatomical requirements for the coverage provided by the arm protection components in any military body armour have never been anatomically described.

Deltoid axilla protectors used in (A) interceptor outer tactical vest, (B) Mark 1 Improved Outer Tactical Vest, (C) Mark 3 Improved Outer Tactical Vest.
Protection against projectiles injuring the forearm (Figure 5) is available through commercial products and have been used by the UK in some prototypes that have undergone ergonomics testing. The ulnar aspect of the forearm is, for example, the closest part of the upper limb to any ground-based energised projectiles. However, at the time of publication, no forearm protection has been issued to military forces to the best of our knowledge.

(A) Forearm injury due to discrete energised fragments, (B) such an injury could potentially be prevented with ballistic protective material.
The advantage of defining minimum protection is that it does not specify the design of armour required to protect it nor the material within it. For example, the practicalities of being able to move the arms means that for the foreseeable future the requirement will be fulfilled by soft armour which is flexible and cannot in most cases defeat a high velocity bullet. The aim of this review was to identify objective evidence to determine which anatomical structures within the axilla and arm require protection from ballistic projectiles in order to define the minimum coverage required.
Method
A systematic review was undertaken using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses methodology13 to identify published evidence for the outcome of damage to the anatomical structures within the arm and axilla. Four scientific databases (PubMed, ProQuest, Web of Science and Google Scholar) were searched as well as four limited-access sources (the Ministry of Defence (MOD) online library, the Barrington digital library at Cranfield University, the Defence Scientific and Technology Laboratory (Dstl) Athena online library and the proceedings of the Personal Armour Systems Symposia conferences) using the search terms: military, trauma, brachial plexus, arm, axilla, junctional, artery, vein, nerve and protection. Structures were identified that if damaged were highly likely to lead to either death within 60 min or would cause significant long-term morbidity. A time period of 60 min from time of injury to arrival at a role 2 surgical facility was chosen as this reflects the target that both the UK MOD14 and the US Department of Defense strive for.15
Results
Haemorrhage from vascular damage to the axillary or brachial vessels (Figure 1) was demonstrated to be the principal cause of mortality from arm trauma on combat operations5–9 ,16–20 (Table 1). The incidence of vascular injury to the arm increases the further away from the torso the injury occurs. A 7-year review (2002–2009) of 1570 military vascular injuries in US forces that found axillary vessel damage in 2%, brachial in 11% and distal extremity in 19%.17 Overall, 9%–19% of upper extremity vascular injuries result in amputation, with the incidence of amputation again increasing the further away from the torso the injury occurs.19 ,21 ,22 Long-term functional outcomes from upper extremity amputations are even worse than lower extremity amputations,23–25 with only 8% of patients returning to full military duties.23 ,25 This was reportedly due to the increased difficulty with the use of upper extremity prosthetics when compared with those used in the lower limbs.26–28
Evidence found from this review supporting coverage requirements of individual anatomical structures within the arm or axilla by ballistic protection
Nerve injury is the primary cause of long-term morbidity including functional disability following upper extremity trauma25 ,29–40 (Table 1). Nerve repair is difficult, with outcomes notably worse the closer to the torso that the nerve is injured.33 The most common complications from upper extremity nerve damage include motor weakness, neuropathic pain, sensory deficit, limb contracture and muscle atrophy.31 Chronic pain is common25 ,41 and can be difficult to manage even with modern pain-modulating medications.42–46 No specific evidence was identified that axillary nerve or musculocutaneous nerve damage from ballistic projectiles was associated with significant long-term morbidity, despite recognition that those nerves have an important role in arm function. Coverage of peripheral nerves within the arm and forearm would reduce morbidity, with protection closest to the torso of greatest importance in terms of outcome; however, no evidence was identified to say where any protection should start or end. No evidence was found that ulnar neurovascular structures were injured more commonly than radial ones, despite the ulnar surface of the forearm probably being closer to the site of ground-based explosive events.
Discussion
Haemorrhage is the principal cause of mortality from arm trauma on combat operations.5–9 ,16 Arresting such haemorrhage, in addition to direct pressure, is primarily through the use of combat tourniquets. It is therefore recommended that the coverage provided by ballistic arm protection should extend to at least the most proximal extent to which a tourniquet can be applied. In most individuals, a tourniquet can be applied as distal as the lower border of the pectoralis major muscle anteriorly. As the tourniquet is tightened it is likely to slip until it is perpendicular to the humeral shaft at that level, which approximates laterally to the deltoid insertion (Figure 6). In addition, with the arm by the side, the neurovascular bundle can be seen to be relatively well protected, particularly if the shoulder is internally rotated which it is when carrying a rifle. As such, protection to the axilla may only be required if the arm will be elevated, exposing the axilla. Avoiding bulking, and potentially uncomfortable material in the axilla may improve acceptability, but this would be dependent on the threat assessment at the time. Limited evidence was found to justify coverage of anatomical structures further along the arm (ie, the forearm) and we would currently not recommend its requirement. However, further analysis should determine whether forearm coverage is required for specific roles such as defensive close combat or public order.

(A) Tourniquet placed as far up the arm as possible, (B) limit of ideal protection therefore equates to the lower border of this tourniquet demonstrated on Zygote.
The Zygote (Zygote Inc) is a commercially procured model originally derived from three-dimensional coordinates describing the outline and geometry of all anatomical structures within the human body. The coordinates were generated from CT and MR scans11 and meshed together to provide a three-dimensional shell. The model is believed to be representative of the external anthropometric sizes of a 50th percentile male within the UK military, although research is currently underway to confirm how well it represents internal anatomical geometries. Zygote acts as the structure underpinning injury analysis programmes such as the Coverage of Armour Tool and other vulnerability models. The OSPREY vest, brassard and shoulder guard were fitted to an exact physical replica of the Zygote model, and the soft armour ballistic protective material components were recreated in the model. The armour components were superimposed over those structures requiring protection , that is, axillary vessels, brachial artery and the radial, ulnar and median nerves. These structures were trimmed off at the lower border of the tourniquet when applied as far up the arm as possible (ie, level with the deltoid insertion). This demonstrated that the OSPREY brassards provide more coverage than just the structures identified as requiring coverage and as such could be reduced (Figure 7). Coverage to a level along the arm equivalent to the bottom edge of the shoulder guard part of OSPREY is sufficient to cover these structures. Such a reduction in coverage may provide significant ergonomic advantage and a potential reduction in thermal burden.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Zygote with tourniquet superimposed, (B) anatomical structures trimmed to lower border of this tourniquet (dashed line). This is just above the level of the shoulder guard (1) and far higher than the lower border of the brassard (2).
Conclusions
Axilla and arm protection should be considered as an item of ballistic protective material designed to prevent the penetration of explosively propelled fragmentation into those anatomical structures responsible for exsanguination not amenable to compression by a tourniquet in the prehospital setting. These structures are the axillary vessels, brachial artery and the median, ulnar and radial nerves. Superimposition of the current OSPREY brassards over these structures demonstrated that their area of coverage could almost be halved while also maintaining the minimum essential coverage.
Permission to publish has been granted by Defence Equipment and Support and the Dstl.
References
Footnotes
Contributors Planning: JB; conduct: JB, RF and EAL; reporting: JB, RF, EAL and JC.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.