Article Text

Abstract
Introduction Body armour is a type of equipment worn by military personnel that aims to prevent or reduce the damage caused by ballistic projectiles to structures within the thorax and abdomen. Such injuries remain the leading cause of potentially survivable deaths on the modern battlefield. Recent developments in computer modelling in conjunction with a programme to procure the next generation of UK military body armour has provided the impetus to re-evaluate the optimal anatomical coverage provided by military body armour against high energy projectiles.
Methods A systematic review of the literature was undertaken to identify those anatomical structures within the thorax and abdomen that if damaged were highly likely to result in death or significant long-term morbidity. These structures were superimposed upon two designs of ceramic plate used within representative body armour systems using a computerised representation of human anatomy.
Results and conclusions Those structures requiring essential medical coverage by a plate were demonstrated to be the heart, great vessels, liver and spleen. For the 50th centile male anthropometric model used in this study, the front and rear plates from the Enhanced Combat Body Armour system only provide limited coverage, but do fulfil their original requirement. The plates from the current Mark 4a OSPREY system cover all of the structures identified in this study as requiring coverage except for the abdominal sections of the aorta and inferior vena cava. Further work on sizing of plates is recommended due to its potential to optimise essential medical coverage.
- FORENSIC MEDICINE
- TRAUMA MANAGEMENT
Statistics from Altmetric.com
Key messages
Body armour acts to prevent or reduce the damage caused by ballistic projectiles to structures within the thorax and abdomen.
Those structures within the thorax and abdomen requiring essential medical coverage by a ceramic plate are heart, great vessels, liver and spleen.
Current front and rear plates in the UK OSPREY body armour system cover most of these structures.
Further work on sizing of plates is recommended due to its potential to optimise essential medical coverage.
Introduction
Historical development of body armour worn by UK forces
Body armour is a type of equipment worn by military personnel that aims to prevent or reduce the damage caused by ballistic projectiles to structures within the thorax and abdomen. Such injuries remain the leading cause of potentially survivable deaths on the modern battlefield.1–7 Bleeding from projectiles penetrating the thoracic cavity in particular is difficult to treat as it is not amenable to compression by applying direct pressure.1 Although modern haemostatic dressings and the early use of blood products can potentially delay the time to death or significant complications8–11 the only way of definitively stopping ongoing intrathoracic bleeding remains surgery.12 However not every soldier sustaining a chest wound dies from it, demonstrating variable vulnerability of the structures within the thorax and abdomen.
The first fielded designs of body armour of the modern era covered the thorax and abdomen with a single type of material to provide protection against fragmenting munitions. However, it was recognised in the 1970s that some anatomical structures are more susceptible to damage than others and that it may be possible to add additional layers to the person to provide some degree of protection against more challenging threats, such as high energy rifle bullets. To reflect this modern body armour can now be thought of as comprising two components, ‘soft armour’ and ‘hard armour’, each of which fulfils a different role. The ‘soft armour’ component covers the whole of the thorax and abdomen and is designed to stop explosively propelled fragments. Soft armour usually contains a woven fabric, thus is relatively flexible, with early incarnations using ballistic nylon and more recently para-aramids such as Kevlar or Twaron.13 ‘Hard armour’ is to designed to defeat high energy bullets and has successively been fulfilled by various designs of rigid ceramic/composite plates2 ,13–19 (Figures 1⇓–3).
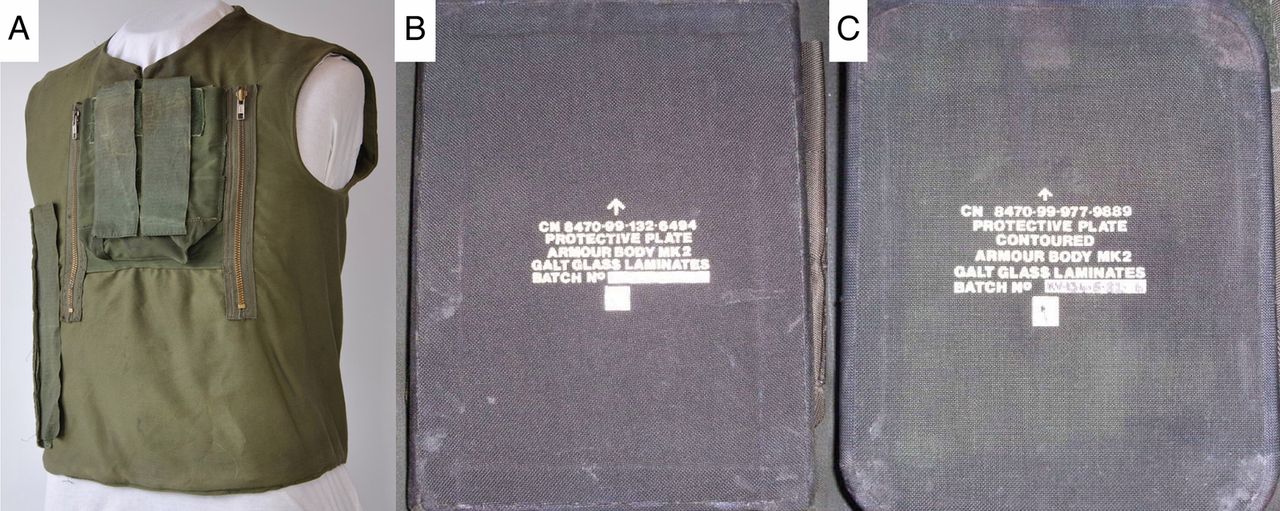
Improved Northern Ireland Body Armour (INIBA) system contains a carrier (A) soft armour worn in conjunction with hard plates—original rectangular front and rear INIBA plates (B) and later replaced by contoured plates (C).

Enhanced Combat Body Armour (ECBA) system contains a carrier (A) soft armour (B) worn in conjunction with front and rear ECBA plates (C) held in external pockets.

The Mark 4a OSPREY body armour system (A) used the new front and rear plates (B). The option for the plates from the Enhanced Combat Body Armour system to be used as side plates (C) or alternatives to the main protective plates and a filler (D) which is the soft armour designed to stop fragmentation.
The original systems, used in the Improved Northern Ireland Body Armour vest (Figure 1) and more recently the Enhanced Combat Body Armour (ECBA) system (Figure 2), incorporated front and rear plates. The exact coverage provided by these earliest plates was not defined in strict anatomical terms at the time, but has subsequently been inferred to be the heart and mediastinum. This coverage was developed upon a balance of understanding between the weight that could be carried, the prevalent threat and that medical attention in the conflict at the time (Northern Ireland) was approximately 20 min away.
The plates used in the OSPREY system (Figure 3) were introduced in 2006 during the Iraq conflict when the threat was redefined and the original assumptions were revisited with the figure for time to medical care recognised to be 1–2 h. This resulted in a design that encompassed the spleen and liver in addition to the existing heart and mediastinum that had been covered by ECBA.
Defining coverage
Historically, protective equipment was designed to prevent death, but there is an increasing recognition that prevention of those injuries causing significant long-term morbidity is also required.20 For example ballistic eyewear has been worn for many years, but more recently pelvic protection was introduced due to the long- term morbidity from genital injuries.2 ,21 However any protective system will be a compromise, between the degree of protection and the encumbrance or ‘burden’ on the wearer. A programme to procure the body armour worn by UK military personnel in the future is currently underway and part of this programme is a desire to optimise the anatomical coverage of the armour, which can subsequently be modified by factors such as tactical considerations on the ground, weight restrictions and equipment integration. Such an approach has recently been successfully undertaken for comparisons of coverage provided by combat helmets,22 face, eye and neck protection.23
The exact medical requirements for body armour have never been openly stated, making objective comparisons between designs more difficult; Box 1 provides suggested definitions to allow comparison. The ‘essential’ and ‘desirable’ medical coverage provided by a particular piece of body armour are medical judgments and should be independent of the ballistic protective material used. Essential medical coverage can be thought of crudely as the minimum coverage that should be provided to all soldiers, although this will realistically be subject to a degree of modification by human factors, considerations such as equipment integration and interoperability. Essential medical coverage is currently provided by ‘hard armour’ in the form of ceramic plates. Generally the remaining coverage (ie, desirable) is fulfilled by ‘soft armour’ in the form of a para-aramid fragmentation vest, although ‘plate carriers’ with reduced desirable coverage exist. The boundaries of the soft armour will be determined by the requirement for mobility and acceptable thermal burden.
Suggested definitions of essential and desirable medical thoracoabdominal body armour coverage
Essential medical coverage
▸ Those anatomical structures that if damaged would likely lead to death prior to definitive surgical intervention being available, for example, bleeding from the thorax that cannot be compressed and requires surgical access (thoracotomy) to arrest it. In current operations it is recommended that structures are chosen based upon a period of up to 60 min from injury to surgery.
Desirable medical coverage
▸ Those anatomical structures potentially responsible for mortality not fitting the requirement for essential coverage as well as those causing morbidity necessitating lifelong medical treatment or that result in significant disability. This includes physical disability as well as psychological disability, for example, damage to the lower parts of the spinal cord (lumbar or sacral parts) may result in significant loss of function in one or both limbs.
Computerised representations of anatomical coverage provided by body armour
Our ability to compare the potential medical effectiveness of different designs of armour has significantly evolved since the introduction of the first type of ‘modern’ body armour to US forces in Korea.14 ,24–28 Initially, work was undertaken using medical opinion and simple shot line models on representations of the human body organs with no representation in the models for the severity of injury. These original models were simplistic with the organ geometry constructed from shapes such as spheres and cubes that were determined from anatomical atlases. To construct the shape of the heart or liver, for example, required digitisation into multiple cylinders (Figure 4).29

Early shot line model (the VULCAN vulnerability analysis package) being used to evaluate armour plates with simplistic representations of the heart and liver from the late 1980s. This model was also used in selecting the OSPREY plate in 2005.
The benefit of models based on simplified geometry was that they were fast to set-up and run, enabling multiple configurations to be conducted quickly. Technology has moved on considerably and it is now possible using complex anatomical geometries to accurately define the positions and also the shapes of the organs using shell elements, rather than simple shapes. One set of injury model platforms now use the commercially procured Zygote model (Zygote), which was originally generated from CT scans.2 The scans provided three-dimensional coordinates describing the outline and geometry of all anatomical structures within the human body, down to the fidelity of the smallest named vessels and nerves. The coordinates were then meshed together to provide a three-dimensional construct by a team at the UK Defence Science and Technology Laboratory (Dstl). This Zygote model is believed to be representative of the skin surface anthropometric measurements of a 50th centile man within the UK military based upon currently available information.2 Body armour designs can be laser scanned and superimposed onto those anatomical structures identified as requiring protection, or conceptual designs can be placed on the body from computer aided drawing files.
The aim of the research in this paper was to re-examine the techniques used to consider the coverage of modern UK body armour protective plate systems to protect the wearer from high velocity rifle bullets and to ascertain if any new evidence or tools exist to refine the medical requirements definition for future body armour.
Method
A review of the medical literature was undertaken in order to ascertain those structures within the thorax and abdomen likely to lead to death or significant long-term morbidity. Using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) methodology,30 PubMed, ProQuest, Web of Science and Google Scholar were searched. Four limited-access sources (Ministry of Defence online library, the Barrington digital library at Cranfield University, the Dstl Athena online library and the proceedings of the Personal Armour Systems Symposia conferences) were also interrogated. This study considered just the use of thoracoabdominal body armour so the following keywords were used: “body armour”, “plate”, “death”, “mortality”, “morbidity”, “complications”, “ceramic”, “coverage”, “ballistic”, “thorax”, “abdomen” and “military”. Structures were identified that if damaged were highly likely to lead to death within 60 min8 (essential medical coverage) or would cause death after that period or result in significant long-term morbidity (desirable medical coverage). A time period of 60 min from time of injury to arrival at either a Role 2 surgical facility or Role 3 field hospital was chosen as this is the target that the UK Ministry of Defence8 and the US Department of Defense strive to meet.10 Strictly defining the time to surgery and not just ‘time to medical care’ as used in the past is important as surgery is the only means of arresting haemorrhage; fluid resuscitation, compression and novel haemostatic agents merely buy time. Structures within the pelvis (such as the iliac arteries) were specifically excluded. Finally the front and rear plates used in ECBA and OSPREY body armour systems were superimposed over those structures identified from the systematic review as requiring full medical coverage.
Results
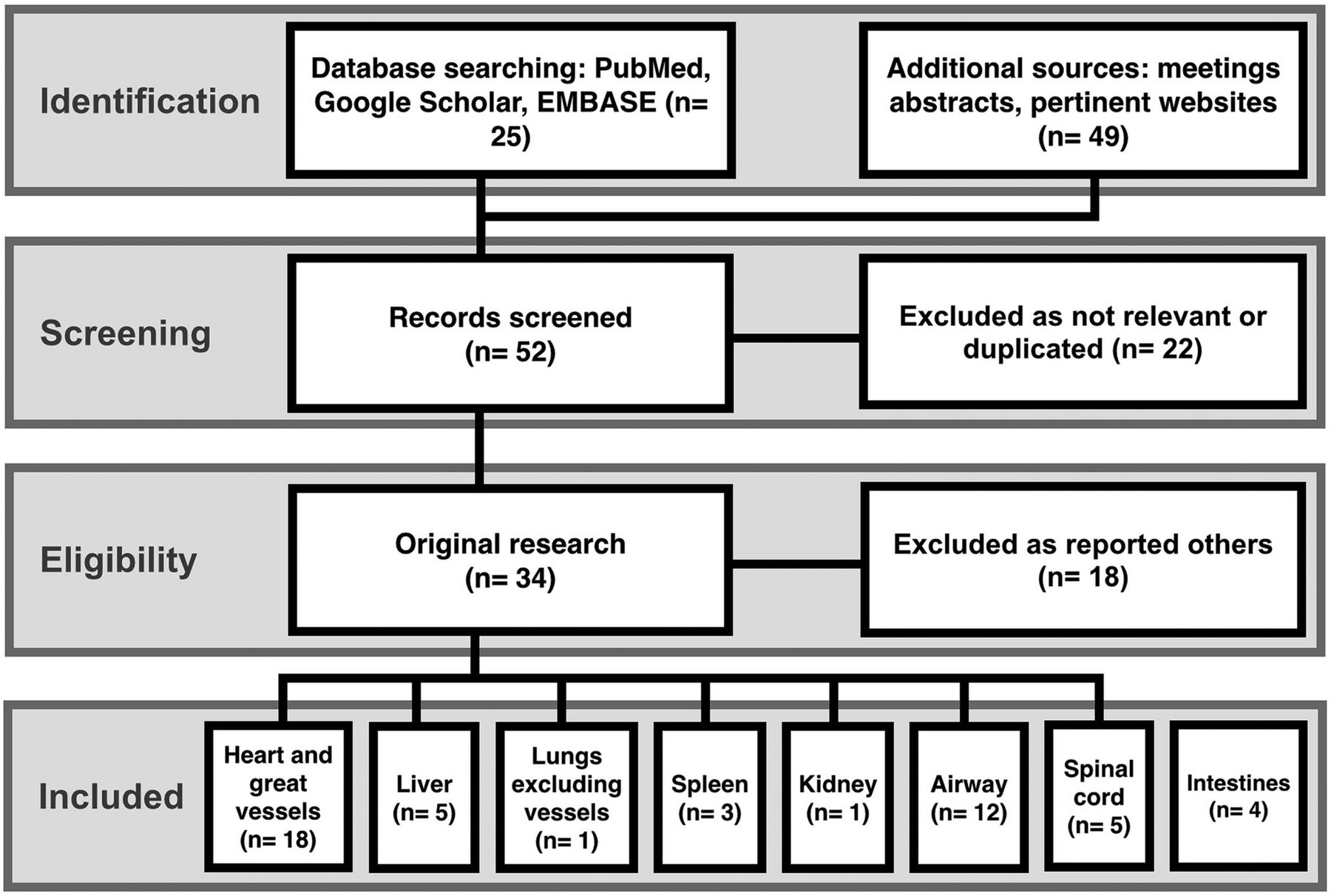
In total, 34 of the 90 sources identified provided pertinent evidence for the outcomes of penetrating missile injury to structures within the thorax and abdomen (Figure 5). A summary of the findings is demonstrated in Table 1.1 ,3–7 ,16 ,31–57
Evidence found from this review necessitating coverage requirements of individual anatomical structures by ballistic plates

Results of the literature review undertaken using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) methodology.
The individual structures comprising the ‘great vessels’ were as according to the Gray’s anatomy definition: superior and inferior vena cavae, pulmonary arteries and veins and the aorta.58 After the bifurcation of the aorta these vessels are considered to be within the pelvis and were therefore excluded. Traumatic injuries to the heart, pulmonary vessels as well as the superior and inferior vena cavae are associated with mortality rates of between 23% and 75%.59–66 Patients with abdominal aortic injuries from gunshot wounds are three times more likely to survive than those with thoracic aortic injuries but the quoted mortality rate of 34% warrants inclusion.67 ,68
A low incidence of military splenic injury was found (3% of intrathoracic injuries), with none of those publications describing their outcome. The low incidence of military splenic injury likely reflects that body armour is routinely worn now by UK soldiers on all modern operations36–38 and is likely to mask the true risk of splenic injury were it not worn. Civilian papers describing comparable ballistic projectile penetration of the spleen demonstrated high mortality (14–67%) and therefore necessitating essential coverage.49 ,50 An open access Home Office report was identified that described the anatomical structures requiring coverage for police ballistic armour which included the heart, liver, lungs, kidneys and spleen,69 although the authors did not provide reasons why these particular structures were chosen.
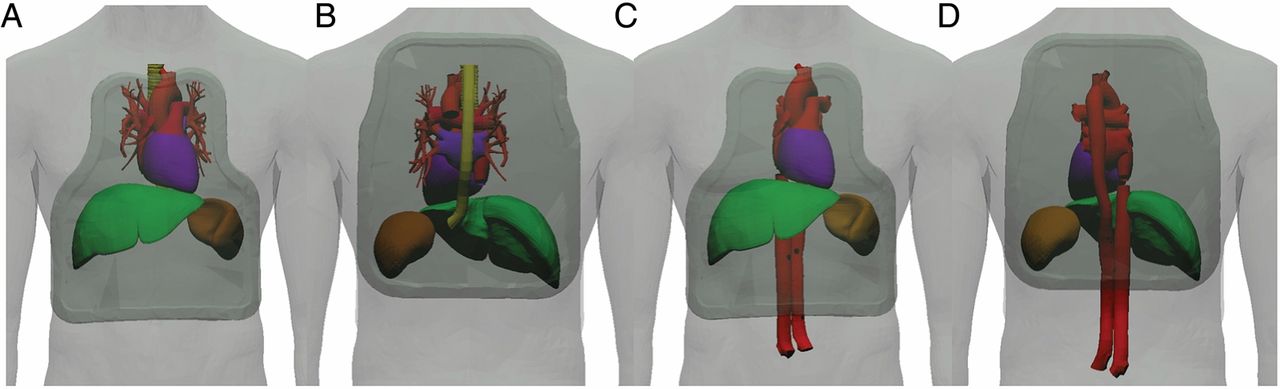
The front and rear plates used in the ECBA body armour system were superimposed over those structures identified from the systematic review above as requiring essential medical coverage: heart, great vessels, liver and spleen. Almost complete coverage of the heart and immediately surrounding vessels from front and rear horizontal shot lines is demonstrated (Figure 6). Protection of the liver and spleen is limited with the ECBA plates (Table 2), reflecting their original requirement. Superimposition of the OSPREY plates used in the current Mark 4a OSPREY body armour system over the anatomical structures requiring essential coverage demonstrates complete coverage of all these structures (Figure 7) in the front and rear directions, with the exception of the abdominal components of the aorta and inferior vena cava.
Essential medical coverage of anatomical structures within the thorax and abdomen by different plates when viewed in the front and rear in a horizontal plane
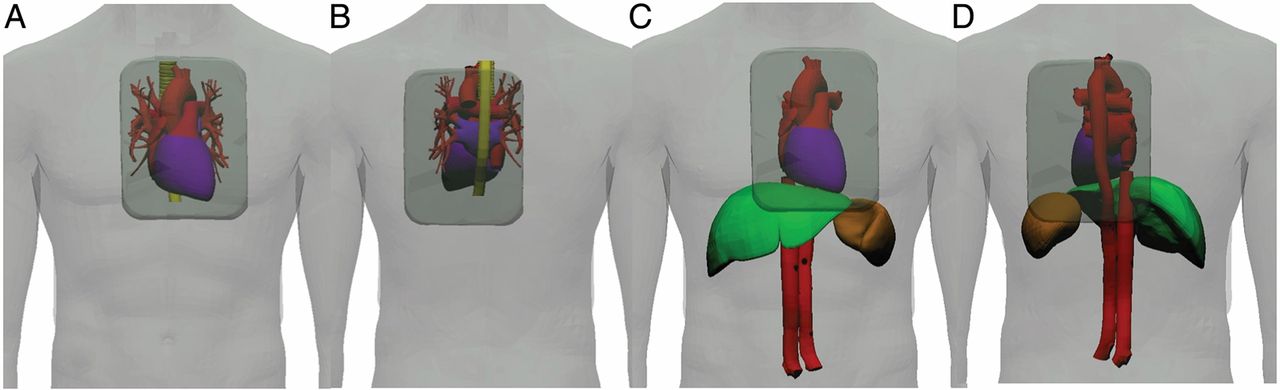
Plates within the Enhanced Combat Body Armour (ECBA) system superimposed upon original coverage requirements in front (A) and rear (B) horizontal planes. Coverage requirements derived from this review in front (C) and rear (D) horizontal planes.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Plates within the Mark 4 OSPREY body armour system superimposed upon original coverage requirements in front (A) and rear (B) horizontal planes. Coverage requirements derived from this review in front (C) and rear (D) horizontal planes.
Discussion
This review has identified those structures within the thorax and abdomen likely to cause death before 60 min and therefore requiring essential medical coverage, are the heart, great vessels, liver and spleen. This value was derived from current guidelines produced by the UK and USA for the ‘gold standard’ maximum time interval between notification of injury and arrival of the casualty at the Role 2 medical facility. Although this timeline is achievable in Afghanistan where well established evacuation protocols existed,9 it is recognised that timelines in future conflicts may be significantly longer, especially in early operations.18 Therefore the structures necessitating essential coverage may alter should a timeline of 60 min be unfeasible. Such decisions should also be reviewed in light of postmortem and casualty data interpretation when that becomes available as has been undertaken in previous conflicts such as Iraq and Afghanistan.3–7 ,13 ,23 ,70 The spinal cord, intestines, lungs and kidneys cause significant morbidity and should be covered wherever possible (desired medical coverage); in the context of current body armour systems this will be by soft armour.
Using the geometries within the current Zygote model; the front and rear ECBA plates alone do not cover all the structures now recognised to be important, but exactly fulfils the original requirement to provide coverage to the heart and those vessels immediately around it. The front and rear OSPREY plates cover the structures that this current review has demonstrated to be important with the exception of the abdominal sections of the aorta and inferior vena cava. It is important to stress the importance of these assessments having been undertaken on a representation of a male UK soldier in a horizontal plane. Although a horizontal plane would likely be representative of most bullet trajectories with a patient in the standing position, it may not represent other trajectories such as when in a firing prone position or from ricochets. Such a concept is the premise of the Coverage of Armour Tool (COAT), that enables objective comparisons between armour designs in terms of percentage coverage from different shot lines.70
Body armour designs in COAT are superimposed over those anatomical structures within the Zygote deemed to necessitate protection. Currently the Zygote is believed to be a good approximation of the external skin surface geometry of a 50th centile male soldier based upon the limited relevant military anthropometric information available. However further assessments are required to ascertain whether this is correct as well as to scale the geometry of internal anatomical structures. This will enable construction of multiple geometries scaled to different anthropometric sizes of UK soldiers such the 5th and 95th centiles. These should additionally provide evidence to support the trialling of a number of different plate sizes, which can be fitted to an individual’s height or bone anthropometric landmarks on the skin surface. The CT scans on which Zygote are based are taken with the subject at full inspiration, moving the liver and spleen to their most inferior positions, so that their positions in Zygote could be considered to be extreme.
COAT enables objective comparisons between armour designs in terms of percentage coverage from different shot lines but does not provide any indication of potential injury. High energy bullets for example generally result in high-energy transfer, causing irreversible tissue damage at some distance away from the projectile path.47 ,71 The next step to this work therefore needs to address models that enable the visualisation of the coverage of armour and incorporate injury prediction. Such an approach is currently being developed in the Dstl Personal Vulnerability Simulation tool and includes cavitation dimensions based on gelatine.72
Conclusions
A systematic review of the literature has demonstrated that those anatomical structures within the thorax and abdomen predicted to be responsible for death within 60 min and thereby requiring essential coverage are the heart, great vessels, liver and spleen. For the geometrical model used in this study the front and rear plates from the ECBA body armour provide limited coverage of these structures, but do fulfil their original requirement. The plates from the current Mark 4a OSPREY body armour cover all the above structures except for the abdominal sections of the aorta and inferior vena cava. Further work on sizing of plates is recommended due to its potential to optimise coverage.
Acknowledgments
The authors thank the following colleagues for their advice and identifying any information not previously available: Dr Leslie Payne (Ballistic Archives), Dr Mark Dorn (Frazer-Nash Consultancy Limited) and Dr Debra Carr (Cranfield University).
References
Footnotes
Contributors Planning: JB, RF, EAL; conduct: JB, RF; reporting: JB, RF, EAL, JC, AEH, PM.
Funding The authors can confirm that no funding was provided for conducting this research. Permission to publish has been granted by Defence Equipment and Support (DE&S) and the Defence Scientific and Technology Laboratory (Dstl). Crown copyright 2014. Published with the permission of the Defence Science and Technology Laboratory of behalf of the Controller HMSO.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.