Article Text

Abstract
To assess the associations of acceleration force indicators (aircraft type and flight hours) with cervical and lumbar pain and radiological degeneration among fighter pilots. The PubMed, Embase, Scopus and Web of Science databases were searched until October 2013. Twenty-seven studies were included in the review and 20 in the meta-analysis. There were no differences in the prevalence of neck pain (pooled OR=1.07, 95% CI 0.87 to 1.33), cervical disc degeneration (OR=1.26, CI 0.81 to 1.96), low back pain (OR=0.80, CI 0.47 to 1.38) or lumbar disc degeneration (OR=0.87, CI 0.67 to 1.13) between fighter pilots and helicopter or transport/cargo pilots. Moreover, the prevalence of cervical (OR=1.14, CI 0.61 to 2.16) or lumbar (OR=1.05, CI 0.49 to 2.26) disc degeneration did not differ between fighter pilots and non-flying personnel. Most studies did not control their estimates for age and other potential confounders. Among high-performance aircraft pilots, exposure to the highest G-forces was associated with a higher prevalence of neck pain compared with exposure to lower G-forces (pooled OR=3.12, CI 2.08 to 4.67). The studies on the association between flight hours and neck pain reported inconsistent findings. Moreover, looking back over the shoulder (check six) was the most common posture associated with neck pain. Fighter pilots exposed to high G-forces may be at a greater risk for neck pain than those exposed to low G-forces. This finding should be confirmed with better control for confounding. Awkward neck posture may be an important factor in neck pain among fighter pilots.
Statistics from Altmetric.com
Introduction
Cervical and lumbar spine disorders are common conditions in fighter pilots. One out of two fighter pilots reports neck pain and one out of three reports low back pain.1 In addition, nearly 15–50% of fighter pilots show cervical2 and 10–50% lumbar disc degeneration radiologically.3 ,4
Fighter pilots are exposed to high accelerations during flight. Air combat engagements with currently used fighter aircraft consist of multiple, frequently repetitive excursions to high Gz levels (Gz is a gravitational force that is applied to the vertical axis of the body). Peak levels usually range from +7 to +9 Gz, and approximately 20% of the flying time is spent with Gz loading above +2 Gz.5 Fighter pilots have reported a higher prevalence of neck and low back pain as well as multisite pain than transport or cargo pilots.1 High G-forces have been suggested as an underlying factor.1
A fighter cockpit is a compromise between limited space, the placement of controls and ejection seat requirements. The position of the backrest of an ejection seat more upright than recommended may stress the low back structures.6 Moreover, the cervical spine of fighter pilots is especially susceptible to injuries. High G-forces, frequent turning and tilting of the head and neck as well as the weights of the helmet and oxygen equipment increase the stresses on the cervical vertebrae, especially during neck rotations and extensions.7
To date, a single meta-analysis on the association between exposure to acceleration forces and radiologically confirmed cervical disc degeneration has been conducted and published in a report.2 That meta-analysis comprised seven studies and showed a significantly higher prevalence of cervical disc degeneration in fighter pilots compared with other pilots or non-flying personnel. We are not aware of any other meta-analyses on the role of occupational physical factors in cervical or lumbar pain or degeneration among fighter pilots. Our aim was to carry out a systematic review to assess the possible associations of acceleration forces with cervical and lumbar pain and degeneration among fighter pilots and to estimate the magnitude of these associations with meta-analyses.
Methods
Search strategy
We conducted comprehensive literature searches in the PubMed, Embase, Scopus and Web of Science databases until October 2013 using the following predefined keywords: (Gravitation OR gravity OR gravit* OR G-force OR pilots OR helicopter OR military OR jet OR fighter OR flight OR flying) AND (spine OR spinal OR neck OR back OR disc OR cervical OR lumbar OR degeneration).
We used both MeSH terms and text words in PubMed, and we used Emtree terms and text words in Embase. We checked the reference lists of included articles for additional studies.
Selection of the studies
We included cross-sectional, case–control and cohort studies that assessed the associations of exposure to G-force with neck or low back pain or cervical or lumbar disc degeneration. We included studies published in English only. To be eligible for a meta-analysis, the studies had to report quantitative data on the associations of occupational factors with cervical or lumbar disorders. RSh assessed the titles, abstracts and full texts of the studies and evaluated the studies for inclusion.
Not only case reports, reviews, guidelines, editorials, and letters are excluded, but also studies on lifetime neck or low back pain (one study) and studies with a sample size less than 10 participants (four studies). The results did not change after including those five excluded studies.
Quality assessment
The quality of each included study was assessed by two authors using the modified Effective Public Health Practice Project tool for observational studies.8 RSh assessed all studies and the second assessments were carried out by other coauthors. Discrepancies were solved by discussion in the group. The following five main domains were assessed: selection bias, performance bias, detection bias, confounding and attrition bias (see Web table 1).
G-forces
We classified aircrafts as fighters, transport/cargo and helicopters. Fighters included aircraft types F-16, F-15, F-5, F/A-18, A-7 and A-4 as having the capacity to induce exposure to high G-forces on pilots (high manoeuvrability, higher G-developing rate and capability to sustain G-forces above 4 Gz). Other jets named in the studies were classified as having low G capacity, and they were combined with helicopters and transport/cargo aircrafts.
Meta-analysis
We estimated crude or age-specific ORs with 95% CIs for the studies that reported the prevalence of cervical or lumbar pain or degeneration in fighter pilots vs. helicopter or transport/cargo pilots, or in fighter pilots vs. non-flying personnel. We calculated Woolf CIs for the estimated ORs.9 We used a fixed model to estimate the overall OR for combining subgroups of a single study, e.g., combining the estimates for different age groups. We used a random model to combine the estimates of a single study on different outcomes, e.g., different signs of disc degeneration.
For a study10 that reported the mean flight hours in participants with or without cervical or lumbar disorder, we calculated the standardised mean difference by dividing the difference between the two means by their pooled SD. We then converted the standardised mean difference into OR.11
We used a random-effects meta-analysis to combine the estimates of different studies and assessed the presence of heterogeneity across studies by the I2 statistics.12 The I2 statistic shows the total variation across studies, which is not due to chance. I2 statistic less than 25% indicates small inconsistency and more than 50% indicates large inconsistency between studies.12 The influence of each individual study on the summary OR and heterogeneity was examined by repeating the meta-analysis leaving one study out at a time.
Publication bias was assessed by a funnel plot and Egger's regression test.13 ,14 The assumption of publication bias is that studies with significant results are more likely to be published than studies with non-significant results. In the presence of publication bias, studies with significant results are more likely to be included in a meta-analysis. In this review, most of the included studies reported non-significant results and the pooled estimates were close to unity. Thus, we assessed publication bias for meta-analyses with positive findings only. We used Stata, V.13 (Stata Corp, College Station, Texas, USA) for meta-analysis.
Results
Our searches initially identified 9879 abstracts (see Web figure 1). RSh screened the full text of all relevant reports. Fifty-seven relevant studies were identified. Of those, we excluded 30 studies conducted on pilots other than fighter pilots, and we finally included 27 studies in the review (see Web tables 2–4). Of these 27 studies, 20 were included in the meta-analyses of neck pain, low back pain or radiologically defined cervical or lumbar disc degeneration.
Our quality assessment showed that most of the included studies did not control for potential confounders and 9 of the 27 studies had strong selection bias (see Web tables 2–4).
Cervical pain and degeneration
Type of aircraft
We used aircraft type to compare fighter pilots with helicopter or transport/cargo pilots and to study the effects of different G-levels. A pooled estimate of four studies on the association between aircraft type and neck pain did not differ from unity (pooled OR=1.07, 95% CI 0.87 to 1.33, I2=0%; figure 1).
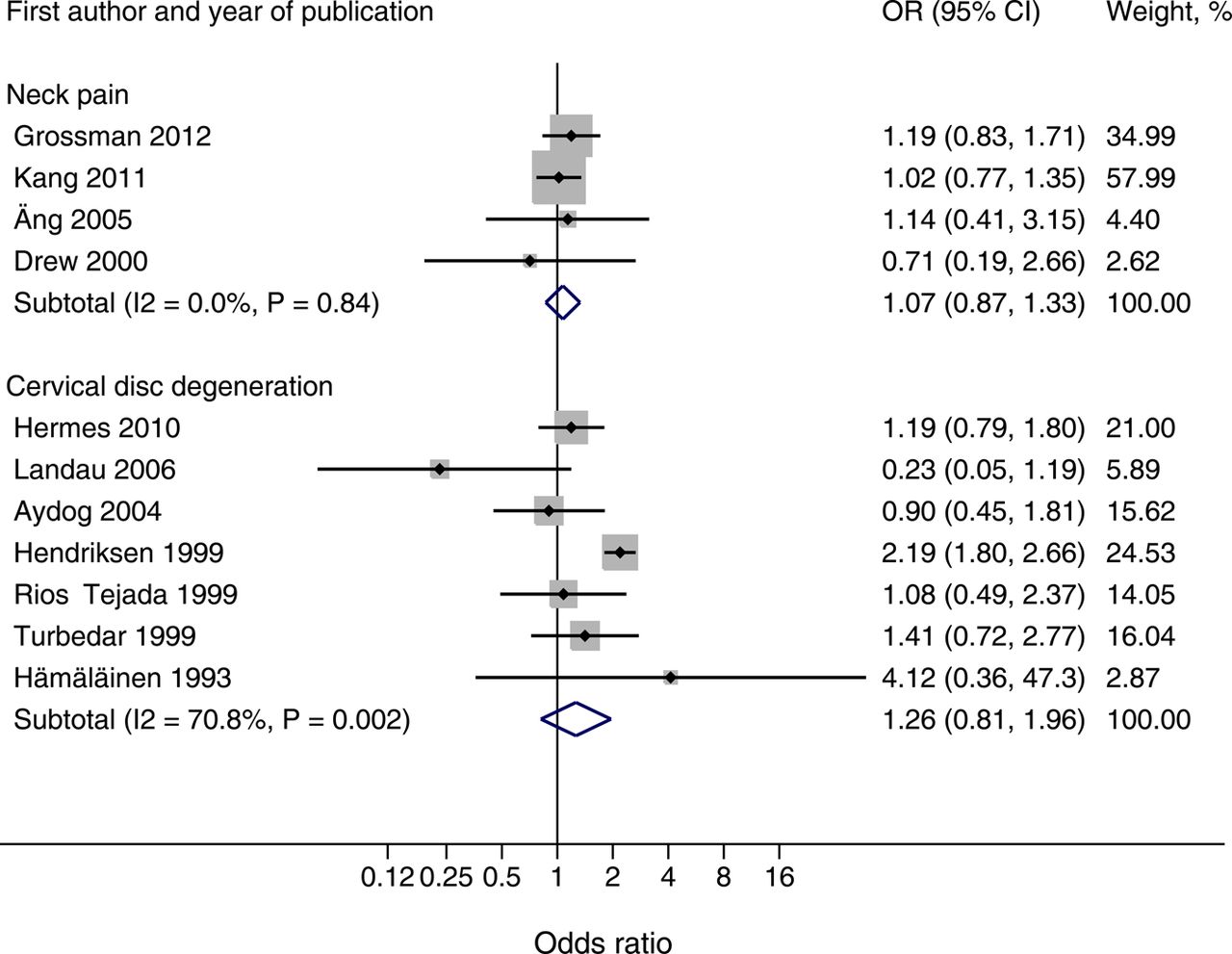
Pooled ORs of neck pain and cervical disc degeneration (radiologically) in fighter pilots compared with helicopter or transport/cargo pilots. The size of the grey shaded area indicates the weight of each study. Horizontal lines show the 95% CIs.
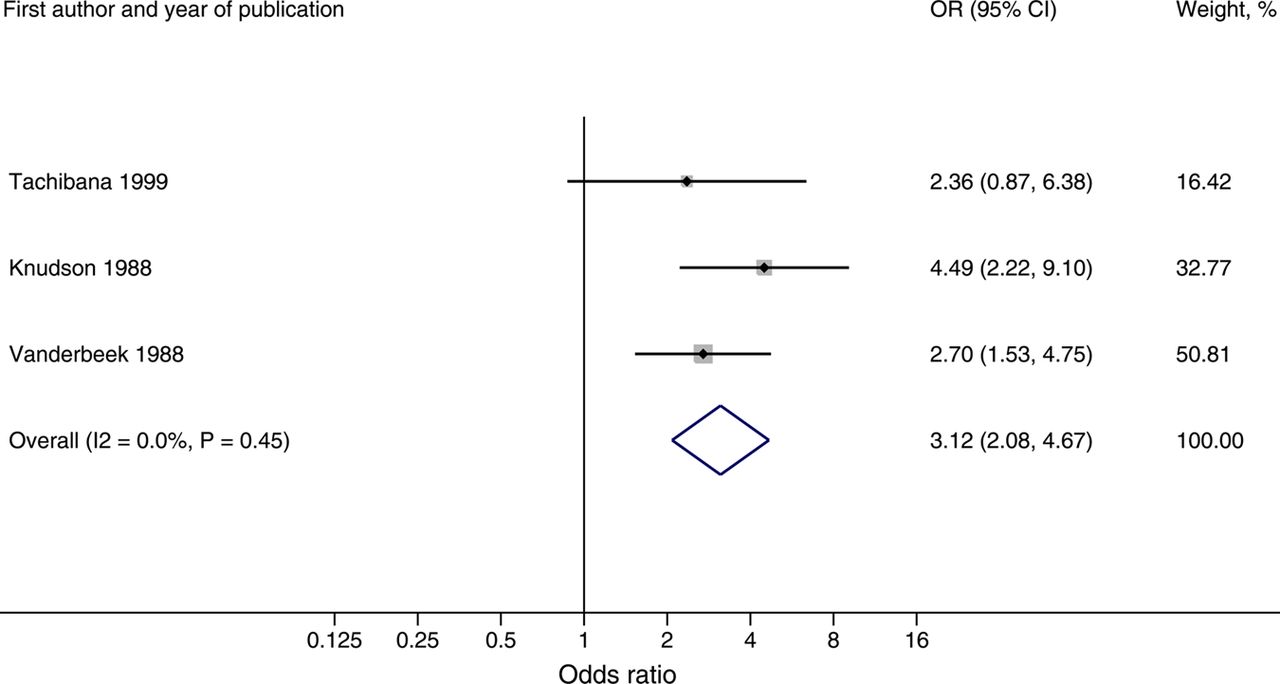
A meta-analysis of three studies15–17 comparing neck pain between two high G-performance aircraft F-16 and F-15 pilots showed no difference (pooled OR=1.19, 95% CI 0.85 to 1.67, I2=0%). However, three studies16 ,18 ,19 compared F-16/F-15 with F-5,16 F/A-18 with A-7/A-418 and F-15 with F-1.19 Neck pain was more common in F/A-18, F-15 and F-16 pilots than in pilots flying the less G-capable aircrafts (including F-5 aircraft). A meta-analysis of these three studies showed a threefold (pooled OR=3.12, 95% CI 2.08 to 4.67, I2=0%) increased risk of neck pain for the highest G exposure (figure 2 and see Web table 2).

Pooled OR of neck pain for exposure to high vs. low G-forces. The size of the grey shaded area indicates the weight of each study. Horizontal lines show the 95% CIs.
A meta-analysis of seven studies on cervical disc degeneration confirmed by imaging (figure 1) showed no difference between fighter pilots and helicopter or transport/cargo pilots (pooled OR=1.26, 95% CI 0.81 to 1.96, I2=70.8%). Of these studies, the largest one reported a significant association between aircraft type and cervical disc degeneration that disappeared after adjustment for age.20
Moreover, there was no difference in cervical disc degeneration confirmed by imagery between fighter pilots and non-flying personnel in the meta-analysis of four studies (pooled OR=1.14, 95% CI 0.61 to 2.16, I2=24.3%; figure 3).

Pooled ORs of cervical and lumbar disc degeneration (radiologically) in fighter pilots compared with non-flying personnel. The size of the grey shaded area indicates the weight of each study. Horizontal lines show the 95% CIs.
Cumulative flight hours
The pooled estimate of four studies10 ,15 ,21 ,22 that reported quantitative data on the association between flight hours and neck pain was 1.54 (95% CI 0.99 to 2.39; figure 4). In all, seven studies10 ,15 ,21–25 explored the association between flight hours and neck pain. Four studies21–24 (two included in the meta-analysis) found no association, but three10 ,15 ,25 did (two included in the meta-analysis). Of the latter group, one study25 (not included in the meta-analysis) did not control for any confounder. In the remaining two studies10 ,15 (both included in the meta-analysis), the association between the number of flight hours and neck pain remained significant after controlling for some confounders. The pooled estimate of the two studies that controlled for some confounders was 1.95 (95% CI 0.77 to 4.91).

Pooled ORs of neck pain for high vs. low flying hours in fighter pilots. The size of the grey shaded area indicates the weight of each study. Horizontal lines show the 95% CIs.
A single study26 found an association between the total flight hours and cervical disc degeneration in high-performance aircraft pilots (OR=2.80, 95% CI 1.21 to 6.51 for ≥2000 h vs. <1000). However, the association disappeared after adjustment for age (OR=1.10, 95% CI 0.41 to 2.93 for ≥2000 h vs <1000).26
Posture
Looking back over the shoulder (checking six)16–18 ,21 was the most common posture that caused neck pain. Moreover, posterior seat (rear of a double seat) was related to the higher severity of neck pain.15
Flight environment
Severe neck pain was reported to be more common in a training environment than in an operational environment.16
Lumbar pain and degeneration
Type of aircraft
A meta-analysis of four studies on low back pain (pooled OR=0.80, 95% CI 0.47 to 1.38, I2=68.1%) and four studies on lumbar disc degeneration confirmed by imaging (pooled OR=0.87, 95% CI 0.67 to 1.13, I2=0.9%) did not show a difference between fighter pilots and helicopter or transport/cargo pilots (figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Pooled ORs of low back pain and lumbar disc degeneration (radiologically) in fighter pilots compared with helicopter or transport/cargo pilots. The size of the grey shaded area indicates the weight of each study. Horizontal lines show the 95% CIs.
Moreover, there was no difference in the prevalence of lumbar disc degeneration between fighter pilots and non-flying personnel in the meta-analysis of two studies (pooled OR=1.05, 95% CI 0.49 to 2.26, I2=0%; figure 3).
Cumulative flight hours
One study27 found no association between the number of high G-force flight hours and low back pain during the preceding 12 months among fighter pilots. However, another study reported an association between flight hours and lumbar disc degeneration.26 This association disappeared after adjustment for age.26
Spinal pain and degeneration
Type of aircraft
Two studies1 ,24 showed no difference in spinal pain between fighter pilots and helicopter or transport/cargo pilots. However, pilots exposed to high G-forces more frequently sought medical care than pilots exposed to low G-forces (OR=2.92, 95% CI 1.08 to 7.87).17 This study, however, did not control for potential confounders.
Furthermore, a single study28 showed a higher prevalence of spinal pain in fighter pilots compared with non-flying aircrew (OR=7.20, 95% CI 3.83 to 13.50). However, this study did not control for age and other confounders. Further, another study29 showed a lower prevalence of spinal disorders in fighter pilots or weapon system officers compared with non-flying air traffic personnel (OR=0.47, 95% CI 0.27 to 0.83).
Cumulative flight hours
A single study28 reported a direct correlation between total flight hours and spinal pain, whereas another study24 did not.
Posture
Checking six was the most common posture associated with pain, followed by forward trunk bending.30
Heterogeneity and publication bias
There was a high level of heterogeneity in the meta-analysis of studies on cervical disc degeneration and low back pain. In the study by Hendriksen and Holewijn,20 the association between aircraft type and cervical disc degeneration disappeared after adjustment for age, but the adjusted estimate was not reported. After excluding this study, the pooled OR of cervical disc degeneration reduced from 1.26 to 1.10 (95% CI 0.79 to 1.53) and I2 reduced from 70.8% to 14.6%. In the meta-analysis of studies on low back pain, pooled OR increased from 0.80 to 1.06 (95% CI 0.77 to 1.47) and I2 dropped from 68.1% to 0% after excluding the study by Froom et al.31
There was no evidence of publication bias either in the meta-analysis of the association between flying hours and neck pain (p value for Egger's test 0.59) or in the meta-analysis of the association between high G-forces and neck pain (p value for Egger's test 0.94).
Discussion
This systematic review and meta-analysis showed no differences in the prevalence of cervical or lumbar pain or radiological degeneration between fighter pilots and helicopter or transport/cargo pilots, or non-flying personnel. Among high-performance aircraft pilots, exposure to high G-forces was associated with neck pain.
We found no association between exposure to G-forces and cervical disc degeneration. The findings of our meta-analysis differ from those in the aforementioned previous report.2 Of the seven studies included in their meta-analysis, we included six in our meta-analysis. In their report, the study by Ziyan and collaborators that reported a strong association has not been published.2 From another study by Rios-Tejada et al32 only one radiological outcome (disc protrusion)—showing a positive association—was included in their meta-analysis and the other two outcomes (osteophytes, disc height change)—showing reverse or no association—were not considered. Furthermore, we included four new studies3 ,4 ,26 ,33 showing no association between G-forces and cervical disc degeneration.
The current review suggests that exposure to G-forces is associated with neck pain in high-performance aircraft pilots. This finding is noteworthy, since two groups of fighter pilots, i.e., groups with similar characteristics and selection mechanisms, were compared. One of the included studies15 suggested that the cumulative G exposure has more effect on neck pain than the peak G exposure. Exposure to high G-forces may involve acute peaks or be cumulative, and the effects of these different types may differ. Since the other included studies did not differentiate between acute and cumulative G-force exposures, it was not possible to investigate this question further in our meta-analysis.
Looking back over the shoulder (‘check six’) was the most common posture that caused neck pain. Check six, i.e., looking directly behind the aircraft, requires maximal neck rotation, often accompanied by extension and lateral bending.34 This posture is closest to the end range in any plane of movement of the cervical spine.35 With the head posture close to the end range, high levels of neck muscle activation and cocontraction have been discovered under high G exposure.36
An awkward neck posture may be the most important underlying factor causing neck pain in fighter pilots. The position of the neck may have more influence on neck muscle activity than the increased load due to head-worn equipment.37 Over a long period, concomitant exposure to G-forces can aggravate the consequences of poor posture.
The studies included in the current review had several limitations. Most of the included studies that used non-flying personnel as a control group did not recruit a representative sample of age-matched and sex-matched controls from other occupations but used volunteers instead. In general, volunteers are healthier than the general population.38 Furthermore, exposures imposed on the neck were in most studies characterised only roughly with aircraft type. The sample size was small in the majority of included studies. Many of the included studies were conducted among a selected group of pilots without reporting the total number of pilots out of which the samples were drawn. Furthermore, most of the studies reported estimates that were not controlled for potential confounders. Age is a major determinant for both neck and low back pain39 ,40 as well as for cervical and lumbar disc degeneration.2 ,3 Moreover, total flight hours increase simultaneously with a pilot's career with his/her age. In one study,26 where age was considered, the association between total flight hours and cervical or lumbar disc degeneration disappeared after adjustment for age. However, pilots flying more agile aircraft have shown an early development of degenerative changes.41
The risk of cervical and lumbar pain or degeneration in fighter pilots should be contrasted with that in a comparable group (e.g., combat specialty personnel with little or no professional aircraft experience) at least with a similar age and sex. Previous studies compared the prevalence or incidence of cervical and lumbar pain or degeneration in fighter pilots with that in other pilots or non-flying air force personnel. Helicopter or transport pilots may be exposed to other occupational risk factors, such as vibration. Comparing fighter pilots with such groups may dilute the adverse effects of their occupational risk factors. A pilot who suffers from a spinal disease may become a non-flying air force officer or shift from a fighter to less loading transport aircrafts. Finally, fighter pilots may under-report their neck or low back pain in order to keep their job and flying status.
We found an association between high G-forces and neck pain. In principle, exposure to high G-forces should be reduced to prevent neck pain. Since this is not feasible for operational reasons, other measures to reduce physical stress to the cervical region should be relied on, for instance, the use of a lighter helmet and avoidance of awkward neck postures during high G-forces when possible. Additionally, frequent muscle endurance training may reduce the risk of in-flight neck pain.17 ,42 ,43
Conclusions
Our findings showed no differences in the prevalence of cervical and lumbar pain or radiological disc degeneration between fighter pilots and helicopter or transport/cargo pilots, or non-flying personnel. Fighter pilots exposed to high G-forces may be at a greater risk for neck pain than fighter pilots exposed to low G-forces. Overall, better characterisation of exposures and the use of similar outcomes and larger sample sizes in future studies would give more insight into neck problems in fighter pilots. Moreover, future studies should better control for confounding.
Acknowledgments
The authors thank chief flight surgeon Tuomo Leino for his help in classifying the capacity of aircrafts in inducing exposure to G-forces on pilots.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors RSh was involved in literature searches, quality assessment and meta-analysis, and assessed all studies. EV-J, HF, KK, MS and TV performed the second assessments. All the authors were involved in the writing, revision and review of the manuscript.
-
Funding This work was supported by the State Treasury of Finland (grant number VK/582/00).
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.