Article Text

Abstract
Cardiovascular diseasesi are the most common cause of loss of flying licence globally, and cardiac arrhythmia is the main disqualifier in a substantial proportion of aircrew. Aircrewii often operate within a demanding physiological environment, that potentially includes exposure to sustained acceleration (usually resulting in a positive gravitational force, from head to feet (+Gz)) in high performance aircraft. Aeromedical assessment is complicated further when trying to discriminate between benign and potentially significant rhythm abnormalities in aircrew, many of whom are young and fit, have a resultant high vagal tone, and among whom underlying cardiac disease has a low prevalence. In cases where a significant underlying aetiology is plausible, extensive investigation is often required and where appropriate should include review by an electrophysiologist. The decision regarding restriction of flying activity will be dependent on several factors including the underlying arrhythmia, associated pathology, risk of incapacitation and/or distraction, the type of aircraft operated, and the specific flight or mission criticality of the role performed by the individual aircrew.
- electrophysiology
- catheter ablation
- cardiac arrhythmias and resuscitation science
- ecg/electrocardiogram
- health care delivery
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- electrophysiology
- catheter ablation
- cardiac arrhythmias and resuscitation science
- ecg/electrocardiogram
- health care delivery
Introduction
Cardiovascular diseases are the most common cause of loss of flying licence globally, and cardiac arrhythmia is the main disqualifier in a substantial proportion of aircrew.1 Frequent ventricular ectopic (VE) beats (or premature ventricular contractions (PVC)), non-sustained ventricular tachycardia (NSVT), and atrial fibrillation (AF) are the most common arrhythmias seen in aircrew.2
Aircrew often operate within a demanding physiological environment, that potentially includes exposure to sustained acceleration (usually resulting in a positive gravitational force, from head to feet (+Gz)) in high performance aircraft. As described in Coumel’s triangle of arrhythmogenesis, clinical arrhythmias are the result of three factors: the anatomic or electrophysiological substrate, the trigger factor, and the modulation factors, of which the most common is the autonomic nervous system.3 4 It has been known for many decades that exposure to +Gz leads to an elongation of the heart5; additionally, this exposure leads to rapid stimulation/inhibition of the sympathetic and parasympathetic systems, and so this is a highly arrhythmogenic environment for aircrew, especially those with pre-existing susceptibility. Benign dysrhythmias such as sinus arrhythmia, low degree atrioventricular (AV) block, and premature atrial or ventricular beats are commonly observed as a physiological response to acceleration during centrifuge training.6 More rarely,+Gz is associated with more significant arrhythmias such as AF or recurrent NSVT. This is often in relation to cardiac abnormalities found during subsequent investigation of aircrew, in whom +Gz has precipitated these events, that may have flight safety implications.6 Particularly worrisome complications of arrhythmias in aircrew are incapacitation secondary to pre-syncope or syncope, or distraction due to symptoms such as palpitations or dizziness that may interfere with aircrew duties and negatively impact flight safety.
Aeromedical assessment is complicated further when trying to discriminate between benign and potentially significant rhythm abnormalities in aircrew, many of whom are young and fit, have a resultant high vagal tone, and among whom underlying cardiac disease has a low prevalence.
As with all individuals, arrhythmia and conduction disturbances in aircrew may be caused by underlying structural heart disease, or endocrine or other non-cardiac organic disorders. Therefore, when investigating arrhythmias in aircrew, a thorough cardiac and general medical assessment is mandatory. For aircrew with confirmed arrhythmia, assessment of both the conduction abnormality and antiarrhythmic therapy (which may have aeromedically relevant side-effects) is critical as both may have implications for flight safety.
Close liaison with subspecialty electrophysiologist expertise is recommended to ensure all potential options are explored as this is a rapidly changing field. Increasingly, aircrew are recommended to undergo, or have already undergone, catheter ablation or device implantation, and both short- and long-term outcome data must be considered when determining aircrew licensing.7–9
This paper describes an approach to electrophysiological screening, further investigation, and risk stratification of electrical abnormalities and arrhythmias in aircrew. Risk stratification for aeromedical disposition depends on the presenting arrhythmia, associated pathology, risk of incapacitation and/or distraction, and specific aircrew duties.
Approach to screening in aircrew
First level investigation
Assessment of aircrew with suspected arrhythmias, or changing resting ECG patterns, should include a thorough medical history including family history, alcohol, caffeine and supplement intake, a physical examination, and a 12-lead ECG. Symptoms such as palpitations (regular or irregular), dizziness, syncope or presyncope should lead to suspicion of an arrhythmic aetiology.
Many abnormal ECG findings may be acceptable in young, fit individuals with high vagal tone, whereas others mandate further investigation and may lead to restriction, or withdrawal, of flying privileges. A more detailed summary of ECG abnormalities and their relevance and consequences for aeromedical investigation are presented in table 1. In those where there may be flight safety consequences, further investigation is mandated.
Recommendations for ECG findings in aircrew
Second level investigation
Further investigation should include Holter monitoring (24 hours to 7 days), echocardiography and exercise ECG, as well as laboratory investigations. Haematological and biochemical samples should include a blood count, electrolytes, and thyroid hormone assessment. Other investigations may be required (ie, urinary catecholamines, etc). When undertaking Holter assessment, the longer the monitoring duration, the more likely it is to reveal abnormal results. If episodic, telemetric ECG monitoring and/or external/implantable event/loop recorders may be appropriate. In certain scenarios, in-flight Holter monitoring may be required (figure 1). While the sensitivity and specificity of exercise ECG for the detection of coronary artery disease (CAD) is low, it provides useful information about cardiovascular fitness, stress induced arrhythmias, QT interval changes with exercise or exercise induced bundle branch blocks. If hypertension is suspected, ambulatory blood pressure measurement should be included.

Spectrum of ambulatory patient monitoring systems. From left to right, the duration of monitoring increases leading to an increase of the diagnostic yield.
Third level investigation/treatment
In a minority of cases invasive electrophysiologic (EP) testing and/or treatment may be required. If invasive EP testing reveals a target for catheter ablation, it is often performed immediately. In certain arrhythmias, genetic testing may be indicated.
In some instances, specialist pharmacological testing may be indicated to confirm or refute a diagnosis—that is, adenosine with an accessory pathway with antegrade conduction, or ajmaline in the case of suspected Brugada syndrome.
In aircrew flying in high-performance aircraft, human centrifuge testing to assess the response of arrhythmias to sustained acceleration may be useful. If underlying structural disease or CAD is suspected, stress echocardiography, cardiovascular CT, cardiac MRI or invasive coronary angiography may be indicated (table 2).10–14
Recommendations for investigation of arrhythmias
Syncope
Syncope is caused by transient global cerebral hypoperfusion and is defined as a transient, self-limiting loss of consciousness, with rapid onset and spontaneous complete recovery after a short time period. Pre-syncope occurs when there are symptoms of cerebral hypoperfusion without a loss of consciousness. The aetiology of loss of consciousness is diverse and may be caused by neurogenic reflexes, cardiovascular disease or arrhythmias, neurologic or psychiatric conditions, medications, and a variety of metabolic disorders. Vagally-mediated syncopal attacks are common and if isolated can be considered benign, but recurrent or unprovoked syncope requires careful evaluation.
Careful aeromedical evaluation is necessary to elucidate the cause of syncope and to determine the risk of recurrence. Neurogenic syncope refers to a reflex response causing vasodilatation and/or bradycardia, rarely tachycardia, leading to systemic hypotension and cerebral hypoperfusion. Types of neurogenic syncope include neurocardiogenic (vasovagal) syncope, carotid sinus syncope and situational syncope . The overall recurrence rate of vasovagal syncope may be as high as 30%.15 In aircrew, a thorough investigation with ECG, echocardiogram, exercise ECG and, in some cases, tilt table and an implantable loop recorder (ILR) is often required if more than one syncopal episode has occurred. International guidelines regard ILR implantation as a class IA indication in the early phase of evaluation in patients with recurrent syncope of uncertain origin, or in high risk patients in whom a comprehensive evaluation was not successful in identifying an underlying cause.16
In an aviation context, a syncopal attack may lead to sudden incapacitation and loss of aircraft control,17 while pre-syncope that causes distraction or incapacitation may also be potentially catastrophic.
A single episode of loss of consciousness, if associated with a clear precipitant, and likely neurocardiogenic (vasovagal) origin, should not lead to aircrew being restricted in their flying duties—for example, if associated with venepuncture or prolonged standing, without incontinence, and followed by complete and rapid recovery. Additionally, a syncopal episode associated with a physiologic loss of consciousness because of reduced partial pressure of oxygen (PaO2) (eg, during hypoxia training) or a G induced loss of consciousness (GLOC) in the centrifuge, may also be deemed to be benign, if isolated. In other cases, if a clear precipitant is identified and the risk of recurrence is low and/or the underlying condition or triggering factor can be adequately controlled, return to restricted flying duties may be possible after a period of observation (table 3). Recurrent episodes of loss or disturbances of consciousness, orthostatic or symptomatic hypotension, or recurrent vasodepressor syncope are all disqualifying for aircrew duties.
Recommendations for syncope
Rhythm and conduction disturbances
Bradyarrhythmias and conduction disturbances
Sinus node dysfunction
Sinus bradycardia and sinus arrhythmia are common findings in active people; these findings often normalise during exercise and are usually asymptomatic. Individuals who maintain cardiovascular fitness also often have increased vagal tone,18 19 and may have a higher incidence of junctional rhythm, and increased heart rate variability. These findings, in isolation, are compatible with all aircrew duties, including in single seat, high performance aircraft.
In contrast, aircrew with syncope or presyncope caused by sinus bradycardia, sinus arrest or sino-atrial block should be grounded. In asymptomatic individuals, sino-atrial arrest >3 s during the daytime and >4 s at night should also lead to temporary withdrawal of aircrew privileges (table 4).20 Such individuals require further investigation to confirm or exclude underlying cardiac disease.
Recommendations for bradyarrhythmias and conduction disturbances
Atrioventricular conduction disturbance
First degree AV block in asymptomatic aircrew can be regarded as a normal variant up to 300 ms. It is a common finding in young athletes.21 If the PR interval exceeds 300 ms as a new finding, further investigation is recommended. During exercise ECG (and after atropine) a significant shortening of the PR interval should be observed. Following such investigations, most aircrew can remain flying.
In aircrew, the most common type of second degree heart block is Mobitz type I (Wenckebach). In most cases this is an incidental finding in asymptomatic individuals, and further examination is usually not required.22 23 As with first degree heart block, further investigation is only required in those with symptoms, diurnal occurrence of Mobitz type I or in those aged over 40 years at first presentation. Most aircrew with Mobitz type I may be returned to unrestricted duties.
In contrast to Mobitz type I, Mobitz type II is rarely seen in aircrew24; it is more commonly related to infra-Hisian block, located below the AV node, and carries a risk of progression to third degree (complete) AV block.25 Aircrew with Mobitz type II and complete AV block must be investigated for underlying structural heart disease and, although often asymptomatic, aircrew are unfit for flying because of the risk of sudden cardiac death (SCD), syncope, bradycardia-related haemodynamic symptoms, and heart failure. In most cases pacemaker therapy is indicated. A review by an electrophysiologist is recommended.
Individuals with implanted pacemakers are initially unfit for aircrew duties. A return to aircrew duties may be possible if individuals are not pacemaker dependent, have bipolar lead systems, and have regular pacemaker follow-up.26 The possibility of pacemaker failure and the risk of electromagnetic interference, even if considered low in modern pacemaker systems,27 are also important factors, and aircrew are usually restricted to low performance aircraft that do not routinely employ equipment that use high electro-magnetic frequencies (EMF). EMF sources are common in many military aircraft and other radar systems and should always be considered by occupational physicians before return to military and aircrew duties.
In some instances, discrimination between second degree AV block Mobitz type I and II can be challenging on the ECG, and in aircrew invasive EP testing with measurement of the H-V interval may be helpful.
Right bundle branch block
Incomplete right bundle branch block (RBBB) is a very common finding in aircrew and is seen in 2–3% of routine aircrew ECGs.28 In isolation, it can be regarded as a normal variant and further investigation is not required. Individuals with complete RBBB (which is found in <1% of aircrew ECGs28), should undergo further investigation for structural heart disease, despite it being a normal variant in a proportion of the normal population. Investigation in aircrew should include an echocardiogram, an exercise ECG, and consideration of Holter monitoring. If underlying disease can be excluded, aircrew can be considered fit to continue all duties. In aircrew aged >40 years, coronary artery assessment may also be considered. Flying restriction and follow-up is usually not necessary.
Left bundle branch block
Left bundle branch block (LBBB) is more commonly associated with underlying structural heart disease than RBBB and its incidence increases with age. It is not a common finding in aircrew and has been reported in 0.01–0.1% of healthy military aircrew compared with 0.2–0.7% of various civilian populations.29 30 The prognosis of isolated LBBB in young men is generally benign,31 and the risk of progressive conduction system disease for newly diagnosed LBBB has not been shown to be increased in otherwise apparently healthy young males.32 However, LBBB can be a marker of advanced CAD,33 longstanding hypertension, aortic valve disease or cardiomyopathy, and therefore requires investigation in all aircrew.
Aircrew found to have new LBBB are unfit for aircrew duties pending a thorough cardiological evaluation including echocardiography, an exercise ECG, and coronary angiography (invasive or CT based). Under age 40, a CT coronary angiogram should be considered, and over age 40 it is recommended. Holter monitoring may be useful. Many patients with LBBB have underlying left ventricular hypertrophy.34 A cardiac MRI should be considered, especially if under the age of 40 years.
If underlying heart disease can be excluded, return to unrestricted flying duties may be acceptable; however, many civil and military licensing authorities mandate an observation period and close follow-up with further (often annual) echocardiography, exercise ECG, and Holter monitoring. This is primarily to monitor for the possible development of cardiomyopathy and reducing left ventricular function. Aircrew with exercise induced LBBB should be treated similarly to aircrew with LBBB on a resting ECG. However, coronary assessment is recommended in all aircrew with exercise induced LBBB.
Left anterior and left posterior fascicular block
Left anterior fascicular block (LAFB) is seen in 1–2% of individuals without structural heart disease, while left posterior fascicular block (LPFB) is far less common. Both carry no appreciable risk of progression to higher degrees of block.35 However, LAFB may be associated with myocardial ischaemia and if newly acquired over age 40, underlying CAD should be excluded with CT coronary angiography. Under 40 years, if investigated, an echocardiogram is usually sufficient. LPFB is often associated with RBBB and may be associated with CAD or cardiomyopathy. Investigation with echocardiography, Holter and exercise ECG is recommended, and if over age 40 at presentation CT coronary angiography should be considered. If there are no underlying cardiac abnormalities, unrestricted flying is possible without follow-up investigation, in both types of hemiblock.
Ectopy, tachyarrhythmias, ventricular pre-excitation, and channelopathies
Ectopy
Atrial and ventricular ectopy is frequently discovered on routine aircrew ECGs. For aeromedical purposes, two or more atrial or ventricular ectopic beats on a standard ECG should lead to further assessment with a Holter monitor. On Holter monitoring in aircrew, atrial and ventricular ectopy is quantified as the percentage of total beats and is often graded as rare (≤0.1%), occasional (>0.1% to 1.0%), frequent (>1.0% to 10%), and very frequent (>10%).36
Atrial ectopy
Atrial ectopy (or premature atrial contractions (PACs)) is usually benign and does not require further investigation or restrictions for aircrew, as long as they are not frequent or associated with haemodynamic symptoms.
Atrial ectopy is of aeromedical concern if associated with symptoms, and if numerous, underlying heart disease should be excluded. At higher PAC burden, there is also a concern regarding the potential development of AF. In patients with structurally normal hearts, the data in this area are contradictory. One small database of frequent atrial ectopy was not predictive of tachyarrhythmia in 430 US aircrew (US Air Force (USAF) Aeromedical Consultation Service database), while another, small, non-aircrew study (where frequent PACs were defined as >100 PACs/24 hours), demonstrated that patients with frequent PACs were significantly more likely to develop AF (HR 3.22, 95% CI 1.9 to 5.5; P<0.001), and more composite major adverse cardio- and cerebrovascular events (MACCE), including ischaemic stroke, heart failure and death (HR 1.95, 95% CI 1.37 to 3.50; P=0.001) at 6 years follow-up.37 This latter study demonstrates that a comparatively low burden of PACs may significantly increase the risk of AF and adverse cardiovascular events in the long term. Therefore, aircrew with >1% of PAC on Holter monitoring should be considered for further investigation and regular follow-up with echocardiogram, Holter and exercise ECG; above 5% PAC on Holter assessment, further investigation is recommended, and may result in restriction of aircrew duties (table 5).
Recommendations on atrial ectopy
Supraventricular tachycardia
Supraventricular tachycardia (SVT) is defined as a run of narrow complex tachycardia and may be asymptomatic or associated with palpitations. It may last for seconds to days; however, sustained SVT is defined as having a duration of >30 s.38 The aetiology of SVT include AV nodal re-entrant tachycardia (AVNRT) caused by a dual AV nodal pathway (approximately 60%), AV re-entrant tachycardia (AVRT) caused by an accessory pathway (30%), and atrial tachycardias caused by foci or small re-entrant circuits in the right or left atrium (10%).39
While AVNRT and AVRT often occur in otherwise healthy subjects, atrial tachycardias are often associated with structural heart disease, hypertension, etc, and require investigation in aircrew to exclude an underlying aetiology. Tachycardias usually start suddenly and are usually symptomatic, with distracting symptoms such as palpitations, nausea, dizziness, or haemodynamic symptoms like syncope or presyncope, all being of significant concern in an aircrew population. As a result, all tachyarrhythmias are initially disqualifying for aircrew and require further investigation and management. In cases of suspected SVT, information about alcohol, caffeine or supplement intake is important, because these agents may be provocative.
Little data exist in aircrew populations; however, in a review of 430 US military aircrew evaluated for SVT over a median 8 years follow-up, 42 (10%) had haemodynamically relevant symptoms including syncope, presyncope, light-headedness, chest discomfort, dyspnoea or visual changes, with an additional 21 (5%) experiencing recurrent sustained SVT (defined as >10 min, without haemodynamic symptoms).40 Mean follow-up in this study was 11.4±9.0 years, and median follow-up was 7.9 years with a range from 1 to 35 years. Individuals with asymptomatic SVT often remained symptom-free for many years; however, of those presenting with one or more episodes of sustained SVT, recurrence was 1–2% per annum.41
Individuals with sustained SVT are usually unfit for aircrew duties. If asymptomatic, and in those with non-sustained SVT, a return to aircrew duties may be possible, although with restrictions in many cases. Aircrew with very short runs of asymptomatic SVT may be able to continue unrestricted flying but should be assessed on a case-by-case basis.
Antiarrhythmic drug therapy for SVT is unreliable and often associated with side effects that are incompatible with flying duties. As a result, the therapy of choice for symptomatic SVT is often invasive EP testing and catheter ablation. For most SVT, ablation has a success rate >90% and adverse event rate <3%.42 Ablation success rates for AVNRT and accessory pathways may be as high as 95%. Depending on the aircraft type and role of aircrew, many can return to previous duties. However, depending on the estimated recurrence rate, many aircrew who fly high-performance aircraft, or on single seat platforms, may be restricted, even after clinically successful ablation.
Asymptomatic pre-excitation
Pre-excitation on a 12-lead ECG is caused by an accessory pathway (AP) with antegrade conduction bypassing the AV node, either partially or completely. Usually the ECG shows a shortened PR interval <120 ms and a delta wave. The length of the PR interval depends on the location of the accessory pathway and the conduction properties of the accessory pathway and AV node. In contrast to simple pre-excitation on the ECG, Wolff-Parkinson-White (WPW) syndrome requires evidence of tachyarrhythmia or symptoms of palpitations for diagnosis.
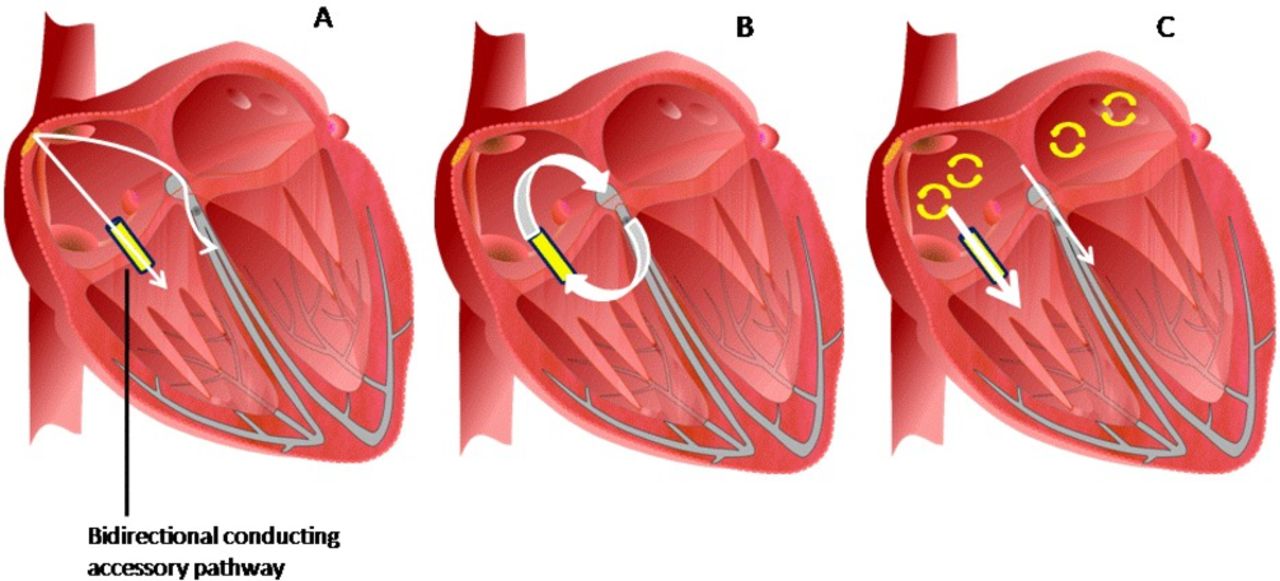
Individuals with fast conduction over the accessory pathway, multiple pathways43 or retrograde conduction over the accessory pathway can be regarded as high-risk individuals (figure 2). Fast antegrade conduction over the accessory pathway may lead to ventricular fibrillation (VF) and SCD in cases of AF, while retrograde conduction over the accessory pathway may allow for AV re-entrant tachycardia.44 Fast antegrade conduction can be determined by observing an RR interval <250ms during AF.43

{kind=link}
{kind=link}
Risks possibly associated with an accessory pathway. (A) During sinus rhythm there is conduction via the atrioventricular (AV) node and accessory pathway. The delta wave in the ECG represents the ventricular pre-excitation caused by the conduction via the accessory pathway. The size of the delta wave and the PR interval depend on the location of the accessory pathway and the conduction properties of the AV node and accessory pathway. (B) A retrograde conduction of the accessory pathway bears the risk of an orthodromic AV re-entrant tachycardia with antegrade conduction via the AV node and retrograde conduction via the accessory pathway. (C) During atrial fibrillation there is a risk of a fast conduction via the accessory pathway to the ventricles depending on the conduction properties of the accessory pathway. As most accessory pathways have no decremental conduction in contrast to the AV node, the conduction via the accessory pathway can be much faster than via the AV node. This can lead to ventricular fibrillation and sudden cardiac death.
In previous aircrew studies, pre-excitation was identified in 0.25–1% of healthy subjects, but only a very small proportion (<2%) of these aircrew had any documented arrhythmia.45 46 In the latter study, with follow-up for over two decades, 15% of patients with pre-excitation developed new symptoms including new tachyarrhythmias, with one case of SCD. As the incidence of AF increases with age, the risk of WPW also increases due to the risk of fast antegrade conduction via the accessory pathway.
In a recently published study from the USAF ECG library, 638 aircrew with pre-excitation (0.3% of all aircrew) were identified over a 68 year period.47 Aircrew who developed high risk features (defined as symptoms, arrhythmia or ablation of a high-risk pathway) were compared with those who remained asymptomatic. Sixty-four of 638 individuals (10%) progressed to the combined endpoint of SCD, arrhythmia and/or ablation of a high-risk pathway with average follow-up of 10.5 years. There were two SCDs (0.3%). Annual risk of possible sudden incapacitation was 0.95% and of SCD 0.03%. Interestingly, those that progressed were significantly younger at presentation.
Ablation for pre-excitation/WPW syndrome is deemed curative in almost 100% of cases, and has a very low risk of complications, particularly for accessory pathways located further from the AV node. For these reasons, all aircrew with pre-excitation documented in a 12 lead ECG should be referred to an electrophysiologist for invasive EP testing and consideration for catheter ablation (table 6).44
Recommendations for supraventricular tachycardia
Atrial fibrillation
AF is the most common type of cardiac arrhythmia seen in aircrew. A study of UK aircrew found asymptomatic AF in 0.3% of all aircrew during routine ECG screening,48 many of whom were returned to flying in a limited capacity.49
Idiopathic AF (without an underlying aetiology) may rarely occur as a single episode, is often paroxysmal (PAF) (≤7 days) but may be persistent (>7 days) or permanent (no attempts/failed attempts to restore sinus rhythm).50 In most cases, AF encountered in the military aircrew population is paroxysmal, idiopathic and converts either spontaneously or by medical intervention within 24 hours. A single episode occasionally has a clearly identifiable cause, such as acute alcohol excess (so-called ‘holiday heart syndrome’) or supplement use.
Aeromedical concerns include palpitations, dizziness, shortness of breath, presyncope, syncope, exercise intolerance, and haemodynamic instability. The loss of atrial contribution to cardiac output, loss of atrioventricular synchrony, and the rapid ventricular response during an episode may impair cardiac performance, especially during exertion, and can be acutely distracting or incapacitating. For these reasons aircrew diagnosed with AF are initially to be made unfit for aircrew duties. Investigations are required to confirm or exclude underlying causes (echocardiography, laboratory tests, chest X-ray, and a risk-factor dependent examination to exclude CAD).
The investigation and management of AF in aircrew requires a comprehensive and integrated approach as it may have a cardiac or non-cardiac aetiology. AF can be associated with valvular heart disease, CAD, cardiomyopathies, hypertension, hyperthyroidism, and respiratory diseases. Other potential causative or trigger factors include electrolyte disorders, sepsis, smoking, alcohol or caffeine excess, drug intake (including metabolic supplements), excessive physical activity, fatigue, and exhaustion. In cases where there is a clear causative aetiology for AF, the underlying disease guides treatment.
AF should be managed in accordance with international guidelines.50 51 w1
Supplemental material
Given the adverse side effect profile of these agents, AF catheter ablation is increasingly recommended as a first line intervention in aircrew, as with the general population.51 Isolation of the pulmonary vein ostia within the left atrium may be achieved by radiofrequency, cryotherapy or laser-based procedures. In PAF success rates >80% can be achieved, with cryo-balloon ablation non-inferior compared with radiofrequency ablation.52 53 Unlike PAF, the long-term success rate in patients with persistent AF is only 40–60% after a single ablation,54 and in many cases a second or third intervention is necessary.
When assessing aircrew that have undergone AF ablation, the observation period to determine the success of the procedure should last at least 6 months; this includes an initial ‘blanking period’ of 3 months, during which the ablation itself may cause arrhythmias regardless of the ablation success, and an additional observation time of at least 3 further months.
As with non-aircrew, anticoagulation should be determined by the CHA2DS2VASc score. Most aircrew have a CHA2DS2VASc score of 0 and do not need anticoagulation. If anticoagulation is needed, it can be done with vitamin K antagonists or direct oral anticoagulants (DOACS). For military aircrew, permanent anticoagulation is often, but not universally, disqualifying; however, civil regulations are usually less restrictive.
Return to aircrew duties requires a detailed cardiovascular assessment and consideration of the aircrew role (table 7). Return to unrestricted flying is usually only possible after a single episode of AF without underlying disease, but with an identified trigger factor. In all other cases, restricted flying in low-performance aircraft may be possible after a minimum observation period of 3–6 months depending on flying duties, with extensive investigation to confirm stable sinus rhythm or rate control at rest and during effort (long-duration Holter monitoring, exercise ECG). In both paroxysmal AF and persistent AF, recurrences may occur years after ablation therapy, and as a result, most licensing authorities do not allow a return to single seat flying operations or high-performance flying. In severe situations that require surgical ablation, mostly performed as a concomitant procedure to coronary bypass or valve surgery,55 or a left atrial appendage exclusion with internal devices because of contraindication to anticoagulation, aircrew are likely to be unfit for flying.
Recommendations for atrial fibrillation
Atrial flutter
Atrial flutter may coexist with AF or occur in isolation. In most cases atrial flutter is caused by similar underlying pathology to those causing AF with similar aeromedical concerns. An additional concern in atrial flutter is the potential for 1:1 AV conduction resulting in extreme tachycardia and acute incapacitation. Aircrew with atrial flutter require thorough cardiac and non-cardiac evaluation (table 8).
Recommendations for atrial flutter
Typical atrial flutter is a right atrial macro-re-entrant tachycardia with the re-entrant circuit passing through the cavo-tricuspid isthmus. Antiarrhythmic medication is usually only moderately effective and not appropriate for aircrew. Catheter ablation is usually the first line therapy, ablating a line to block the isthmus pathway, and has success rates >90% with up to 2 years follow-up.56 Some studies suggest a moderate rate of subsequent AF, following flutter ablation,57 and recurrence can sometimes occur years after the ablation, with the highest incidence in those with atypical flutter (non-isthmus-dependent) and associated structural heart disease.
Due to the arrhythmogenic +Gz environment, single seat and flying high performance aircraft are not generally recommended following flutter ablation. In selected cases, consideration of a diagnostic EP study to reconfirm bidirectional isthmus block would be recommended if considering a more lenient approach.
Ventricular ectopy/premature ventricular complexes (VE/PVCs)
VE/PVCs are a common finding in aircrew and have been reported on 12-lead ECG in about 0.8% of aircrew compared with 2.0–7.0% of civilian populations.58 Aeromedical concerns related to VE/PVCs include haemodynamic compromise, particularly during +Gz, and possible underlying heart disease.
An additional concern is the development of tachycardia-related cardiomyopathy following recent evidence that large numbers of PVCs (>10% burden) can cause cardiomyopathy and should be treated by antiarrhythmic drugs or catheter ablation.59
For aircrew with two or more PVCs or complex ectopy on a routine ECG, further assessment with a 24 hour Holter monitor, echocardiography and exercise ECG is recommended. Suppression of ectopy with exercise is reassuring. In aircrew assessment with exercise ECG, if the number of PVCs exceeds 10% in a 30 s period during exercise, further investigation with echocardiogram and Holter is also recommended.
The ectopy burden on the 24 hour Holter determines the requirement for further specialist work-up. If the VE burden exceeds 1% further investigation should be considered; if >2%, or complex forms are prevalent, further investigation is recommended to exclude cardiomyopathy. Recent evidence suggests that cardiac MRI may be particularly useful in this scenario.60 If aircrew with frequent ectopy burden are under the age of 40 years at presentation, a CT coronary angiogram should be considered; if over age 40, it is recommended.
Aircrew may often be able to continue to fly in a restricted (dual-pilot) role during evaluation. If the VE burden is <2%, with no complex forms and no evidence of sustained ventricular tachycardia (VT) or complex ectopy, no further testing is usually required, and the results are usually aeromedically acceptable. In aircrew with higher ectopy burden (>5%), yearly follow-up with exercise ECG, echocardiography and Holter is recommended for the early detection of tachycardia related cardiomyopathy. Most aircrew can continue to fly in an unrestricted capacity. In those with a VE burden >7.5% many licensing authorities would consider restricting aircrew to multicrew and low performance aircraft; however, there is no consensus on an upper limit of ectopy that requires disqualification, although if >10% and not suppressed by exercise, many licensing authorities would consider additional restrictions (table 9).
Recommendations for ventricular ectopy
VE ablation has emerged as a state of the art treatment that many believe can effectively cure VE, or at least reduce VE burden significantly, as the origin of aberrant ventricular electrical activity is usually well localised.61It should be considered in symptomatic patients, PVC-induced ventricular tachyarrhythmia or PVC-mediated cardiomyopathy.62While it may be possible to return aircrew to multi-crew, low performance flying, further long-term evidence is required before unrestricted aircrew privileges can be considered.
Accelerated idioventricular rhythm
In AV node dysfunction, idioventricular escape rhythms (IVR) may be seen, usually with a heart rate between 30 and 40 beats per min (bpm), and IVR is defined by the presence of three or more monomorphic ventricular beats. If the heart rate of an IVR exceeds the heart rate of sinus rhythm, this is known as an accelerated idioventricular rhythm (AIVR).
AIVR may be a benign arrhythmia, usually seen in the young,63 64 but can manifest in several different clinical scenarios.65 AIVR occurs due to an increased vagal and decreased sympathetic tone66 and is commonly observed in athletes and athletic aircrew. However, AIVR may also be associated with underlying cardiac disease, including cardiomyopathy67 68 and ischaemic heart disease.69 It is also seen in pregnancy.70
If AIVR is detected in aircrew, underlying disease should therefore be ruled out. Investigation may include the usual gamut of echocardiography, exercise ECG and Holter monitoring, while cardiac MRI may be appropriate in some cases. If no underlying aetiology is found, therapeutic intervention and flying restrictions are not indicated.
Non-sustained and sustained ventricular tachycardia
VT is defined as three or more consecutive premature ventricular contractions at a heart rate of more than 100 bpm. Non-sustained ventricular tachycardia (NSVT) is usually defined as VT with a duration <30 s. VT can be divided into idiopathic or secondary to conditions such as structural, coronary or heart muscle disease, or ion channelopathies. Determining if NSVT is idiopathic can be challenging; however, the presence of frequent VE during recovery directly after exercise appears to be even more predictive of an increased risk of death than frequent VE during exercise.71
From an aeromedical perspective, NSVT for nearly 30 s would potentially be catastrophic and as a result the threshold for defining (significant) VT in aviation cardiology is stricter than civilian guidelines. In a 30 year review of 193 aviators evaluated by the USAF for non-sustained VT, the maximum predicted event rate for idiopathic non-sustained VT was 0.3% per year.72 The longest VT duration was 11 beats or less in 98% of the cohort and the number of VT runs per evaluation was four runs in 90% of the cohort, establishing these two limits as thresholds used by many air forces.
Aeromedical concerns include the presence of haemodynamic symptoms such as pre-syncope or syncope and chest pain, and the risk of acute incapacitation or SCD and distraction in the critical phases of flight. Aircrew with significant underlying structural or cardiac disease or symptoms are unfit for aircrew duties.
Idiopathic VT usually originates from one of the outflow tracts, more commonly the right ventricular outflow tract (RVOT) than the left (LVOT). RVOT tachycardias have a typical morphology with inferior axis and LBBB. The usual treatment options for symptomatic NSVT, such as β-blockers and calcium channel blockers, are incompatible with many flying roles, and the fact that RVOT tachycardia is amenable to ablation, with high success rates, means that ablation should be considered as a first-line therapy.73 74 Even in LVOT tachycardia, where ablation is usually considered only if antiarrhythmic drug therapy is not effective or not tolerated because of side effects, ablation should be considered first line for aircrew. After successful catheter ablation and a period of observation, return to aircrew duties may be considered (table 10). After a certain arrhythmia-free period, return to unrestricted flying may be possible after a case-by-case decision.
Recommendations for broad complex arrhythmias
Individuals with primary or secondary VF are permanently unfit for aircrew duties.
Inherited arrhythmogenic conditions (channelopathies)
Aircrew with inherited arrhythmogenic disorders, including long QT syndrome (LQTS) or Brugada syndrome (BrS), are usually unfit for flying (table 11).75 Channelopathies are usually caused by transmembrane ion channel or protein mutations involved in intracellular calcium handling.
Recommendations for channelopathies
Channelopathies are rare, but LQTS and BrS cases predominate in the aviation medicine literature.75–77 Risk stratification should be performed in specialist centres using international guidelines78 and can be very challenging.79 Crucial factors include medical and family history and genetic testing. High risk patients usually need implantable cardioverter-defibrillator (ICD) implantation to prevent SCD and are permanently unfit for flying. While ICDs may prevent SCD they do not necessarily prevent the arrhythmia and any shock delivered would be potentially distracting or incapacitating. However, after careful risk stratification, restricted flying might be possible in asymptomatic, lower risk individuals, on a case-by-case basis.
Brugada syndrome
BrS is diagnosed in the presence of typical ECG changes. There are three recognised BrS morphology types, with type 1 being associated with the highest risk of arrhythmia and SCD. Type 1 BrS has classic changes in lead V1 and V2 (ST-segment elevation with type 1 morphology ≥2 mm in ≥1 lead among the right precordial leads (V1, V2 positioned in the second, third or fourth intercostal space78) that may occur spontaneously, or after provocative drug test with class I antiarrhythmic drugs such as ajmaline or flecainide. The highest risk patients may present with typical ECG changes and have survived cardiac arrest or syncope. Symptomatic patients are usually treated with an ICD and are unfit for flying.
In asymptomatic individuals spontaneous type 1 BrS ECG is associated with the highest likelihood of clinical sequelae. Other predictors for an increased risk are male gender, family history of SCD, and spontaneous AF. There is controversy about the value of an EP study for inducibility of ventricular arrhythmia. Brugada patients should avoid certain drugs (brugadadrugs.org) and excessive alcohol consumption, and they should reduce fever immediately, for example, with paracetamol. New risk markers like a fragmented QRS complex and a ventricular effective refractory period <200 ms are under investigation.
For aeromedical assessment differentiation between Brugada syndrome and Brugada pattern is important. Patients with Brugada type 1 syndrome may develop ventricular arrhythmia at a rate of 7.7% per year; patients with asymptomatic Brugada type 1 pattern have a rate of 2.3% events per year.80 Pilots that have Brugada type 2 syndrome (saddleback ECG findings) and a history of VF or syncope have 1.39% calculated events per year.81 However, Brugada type 2 ECG pattern without symptoms have <0.5% events per year, with an equally low event rate for individuals with Brugada type 3 pattern. As ECG morphology can change, at least three serial ECGs should be done not less than 24 hours apart. All individuals with type 2 pattern should be challenged with sodium channel blockers. Genetic testing for mutations in the SCN5A gene are of limited use, because there are more than 80 known mutations of this gene, and not all these gene carriers are at significant risk for clinical disease.75
Meanwhile, the arrhythmogenic substrate of Brugada syndrome could be localised at the anterior RVOT epicardium.82 83 Catheter ablation of this epicardial substrate is now possible in many patients with symptomatic Brugada syndrome, preventing spontaneous VT/VF episodes and leading to normalisation of the Brugada pattern. It is hoped that this new therapeutic option may ‘cure’ the subset of patients with symptomatic Brugada syndrome and without overlapping syndrome—that is, combined Brugada syndrome and early repolarization syndromes, without the need for ICD implantation. To test this hypothesis the prospective, multicentre, randomised, non-blinded BRAVE study (Ablation in Brugada Syndrome for the Prevention of VF Episodes) was recently established.
In summary, individuals with symptoms are usually treated by ICD implantation or increasingly catheter ablation and should be grounded. Aircrew with Brugada type 2 or 3 ECG pattern without symptoms, with a negative family history and a negative drug challenge, may be assessed fit for flying with limitations76 and regular follow-up is mandatory. All individuals with spontaneous type 1 ECG, type 1 ECG after challenge with sodium channel blockers, a history of ventricular arrhythmias, syncope, or survived cardiac arrest, and a positive family history should be assessed as unfit for flying.
Long QT syndrome
LQTS can be diagnosed in the absence of a secondary cause for QT prolongation, in particular drugs and ionic disorders, and/or in the presence of an unequivocally pathogenic mutation in one of the LQTS genes. Additionally, the presence of a QT interval corrected for heart rate (using Bazett’s formula or Hodges’ formula) of QTc ≥500 ms in repeated 12-lead ECGs, and in the absence of a secondary cause for QT prolongation, is diagnostic for LQTS. Finally, LQTS can be diagnosed using a clinical risk score that incorporates specific ECG findings, clinical findings, and family history.78 84
LQTS risk in asymptomatic patients depends on the types of genetic mutations and degree of mutation dysfunction. If measuring just the QT interval, patients with a QTc >500 ms can be regarded as high risk, and those with a QTc >600 ms as very high risk. The presence of overt T-wave alternans, especially despite avoidance of drugs with QT prolongation and β-blocker treatment, is a direct sign of electrical instability and calls for preventive measures.78
Among genotyped patients, LQT1 males, who are asymptomatic at a young age, are at low risk of becoming symptomatic later in life, while females, especially LQT2 females, remain at risk even after age 40.
In aircrew, further investigation should be recommended above a QTc cut-off of 470 ms. Symptomatic individuals are unfit for flying. For asymptomatic aircrew, a case-by-case decision should consider all criteria for the aeromedical assessment, including the age of diagnosis, the type of LQTS (mutation identified, expected circumstances and triggers of arrhythmias, possible medical treatment), the duration and stability of QTc (Holter monitoring), and the type of aircraft and aircrew.
Conclusion/summary
Electrical abnormalities are a common finding in aircrew. In a young fit population, many abnormal ECG findings may be considered benign and associated with high vagal tone. However, in those cases where a significant underlying aetiology is plausible, extensive investigation is often required and, where appropriate, should include review by an electrophysiologist. The decision regarding restriction of flying activity will be dependent on several factors including the underlying arrhythmia, associated pathology, risk of incapacitation and/or distraction, the type of aircraft operated, and the specific flight or mission criticality of the role performed by the individual aircrew (online supplementary table 12).
References
Footnotes
↵ i Preamble: Evidence-based cardiovascular risk assessment in aircrew poses significant challenges in the aviation environment as data to support decision making at the low level of tolerable risk in aviation is rarely available from the published literature. As a result, there are discrepancies between aviation authorities’ recommendations in different countries, and even between licensing organisations within single countries. The North Atlantic Treaty Organization (NATO) HFM-251 Occupational Cardiology in Military Aircrew working group comprises full-time aviation medicine and aviation cardiology experts who advise both their military and civil aviation organisations including, but not limited to, the US Federal Aviation Authority (FAA), the UK Civil Aviation Authority (CAA), the European Aviation Safety Agency (EASA) and the US National Aeronautics Space Administration (NASA). The recommendations of this group are as a result of a 3 year working group that considered best clinical cardiovascular practice guidelines within the context of aviation medicine and risk principles. This work was conducted independently of existing national and transnational regulators, both military and civilian, but considered all available policies, in an attempt to determine best evidence-based practice in this field. The recommendations presented in this document, and associated manuscripts, are based on expert consensus opinion of the NATO group. This body of work has been produced to develop the evidence base for military aviation cardiology and to continue to update the relevant civilian aviation cardiology advice following the 1998 European Cardiology Society aviation cardiology meeting.
↵ ii Aircrew: Aircrew are defined somewhat differently in civil and military aviation. NATO and the International Civil Aviation Organization (ICAO) delegates the definition of aircrew to national authorities. In the civilian sector aircrew are often categorised as flight crew (pilots)/technical crew members and cabin crew, with separate regulation for air traffic controllers (ATCO). The military define aircrew more broadly as “persons having duties concerned with the flying or operation of the air system, or with passengers or cargo when in flight”. From a risk perspective, professional (commercial) pilots have a higher attributable risk than private pilots and non-pilot aircrew. Controllers are considered to have an attributable risk equivalent to professional pilots. From a cardiovascular perspective, aircrew whose flying role includes repetitive exposure to high acceleration forces (Gz) comprise a subgroup who, due to the unique physiological stressors of this flight environment, often require specific aeromedical recommendations. A more detailed description of aircrew is available in table 1 of the accompanying introductory paper on aviation cardiology [ref Intro paper].
Contributors All authors were part of the NATO aviation cardiology WG and all contributed to the design and writing of this article.
Funding Produced with support from NATO CSO and HFM-251 Partner Nations.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Commissioned; externally peer reviewed.