Article Text

Statistics from Altmetric.com
The UK Government entrusts the Ministry of Defence (MoD) to ‘efficiently protect our people, project our global influence, promote our prosperity, and maintain a strategic base and integrated global support network’.1 2 Defence Engagement (DE), now enshrined as a core MoD task,3 describes the means by which we use assets, short of bombs and bayonets, to achieve those aims. DE has been practised for years, but has previously been regarded as secondary to the main role of Defence.4 In the past, ‘hard power’ (the ability to coerce and force) took primacy over ‘soft power’ (the ability to attract and co-opt others). Today, these are seen as synergistic, and described as ‘smart power’.5
Fragile states may be threatened by internal or cross-border conflict or insurgency, and further challenged by poverty, corruption, widening inequality, poor basic infrastructure, limited access to education and healthcare, environmental concerns, and crime. Further destabilisation can be caused by local or regional events, such as infectious disease outbreaks or natural disasters. External humanitarian aid alone is not sufficient and may even exacerbate problems to the point of prolonging conflict.6 Through engagement, the UK can offer support to solve systemic government-wide problems, support local providers to strengthen leadership and build capacity to deliver priority services. DE can help with service needs analysis, design, planning, management, delivery, monitoring and evaluation.2 7
International Security Forces (ISF) with robust logistic chains and integrated force protection can operate where other actors cannot. This was exemplified by the Defence Medical Services’ (DMS) role during Op GRITROCK, the UK response to the West African Ebola crisis. The DMS was described as ‘the only part of the UK health sector that is trained, equipped, manned and available to rapidly deploy and operate a complete medical unit as part of an international response to a health crisis’.8
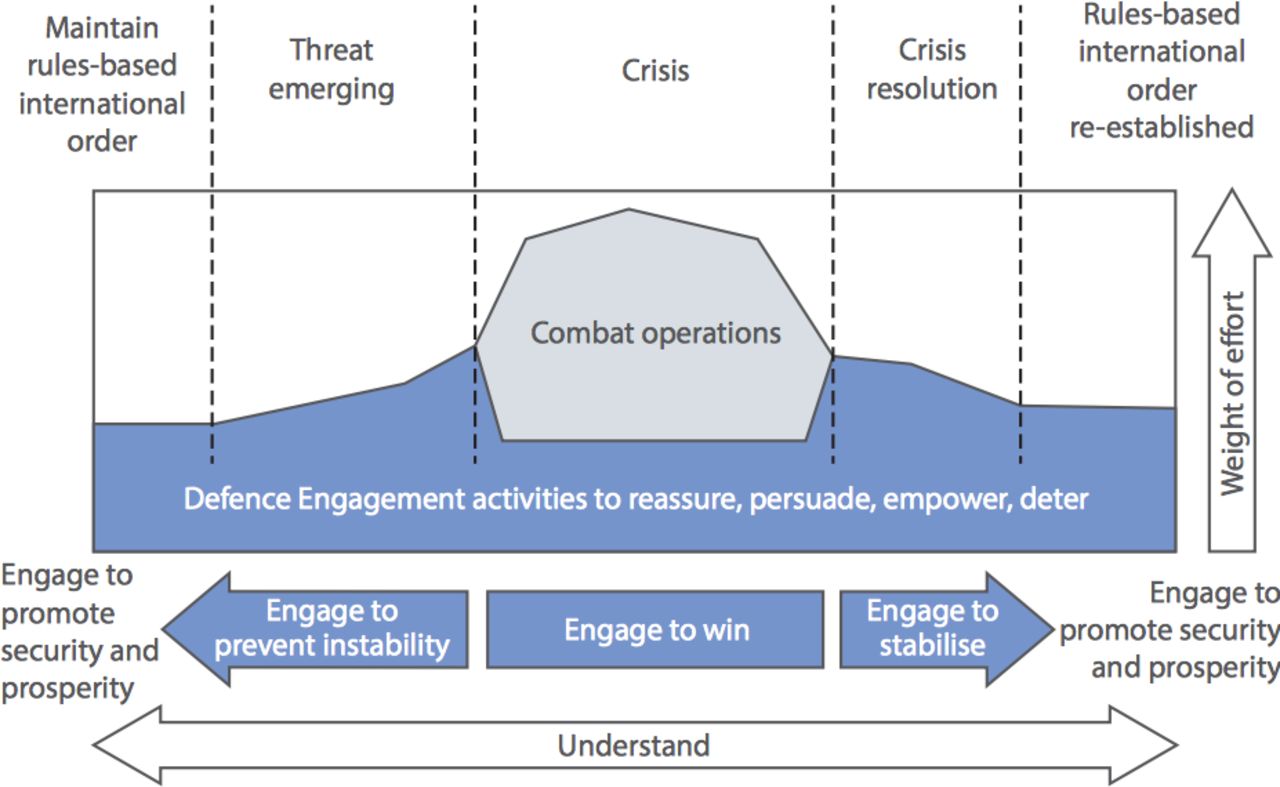
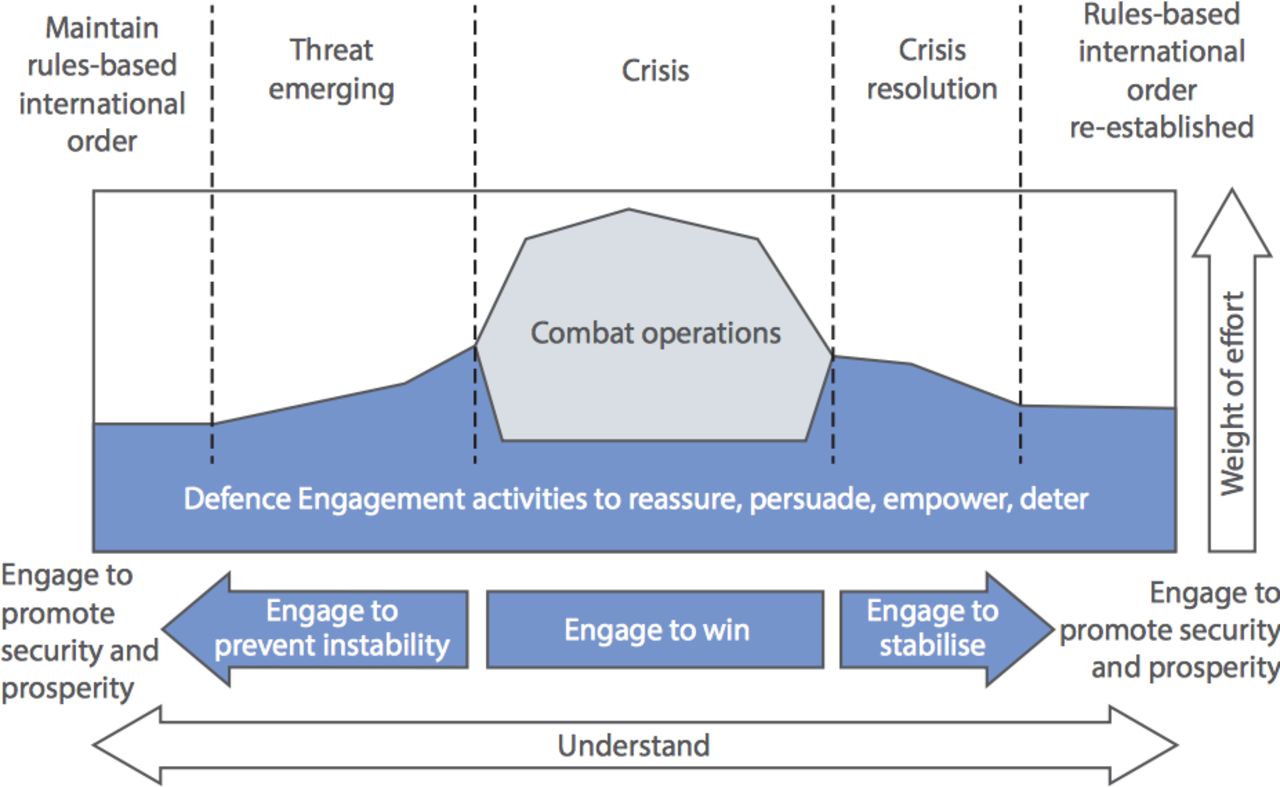
DE activity must use an integrated approach with other governmental departments, such as the Department for International Development and the Foreign and Commonwealth Office, as well as non-governmental organisations.9 This must be deliberate and proactive, and actively involve foreign partners in pursuit of mutual national and security interests. Evaluation of outcomes is critical, and the Enhanced Security Cooperation Activity Plan Application for Defence Engagement database is the framework for capturing and evaluating DE success or otherwise.9 A graphic illustration of the utility of DE is shown in figure 1.
{kind=link}
Defence engagement throughout the spectrum of international security stages. Reproduced from the Ministry of Defence Joint Doctrine Note 1/15.9
Defence Healthcare Engagement
Improvements in the overall health of its people are a profound force for stabilisation within any nation. Health systems have been said to require six ‘building blocks’: governance, finance, health services, information systems, medicines and technologies, and workforce.10 ISF interaction with a nation’s health system has conventionally been during and after conflict or after natural disasters. Four types of involvement have been described, with generally positive and/or negative effects11:
directly protecting or destroying health programmes or assets (positive/negative effect)
providing direct medical care to host nationals (positive/negative effect)
directly importing health problems into a nation (negative effect)
leveraging logistic capability to assist restoration of host national health system after a crisis (positive effect).11
Defence Healthcare Engagement (DHE) is subtly different from the established model of the impact of ISF on a host nation’s medical infrastructure. DHE activity was used by the UK during Op HERRICK in Afghanistan, where the DMS provided the majority of mentors to help strengthen the 215 Corps Afghan National Army surgical capability. DHE emphasises the building of relationships between peers and offers a model of coworking that enables sharing of best practice and empowerment of previously disadvantaged groups (such as female health workers). DHE is now seen as a core competence that the DMS must hone as part of wider DE capacity building.12 DHE must be ethically grounded,13 coherent and consistent with the wider government aims and objectives; it must also offer value for money. DMS concepts and doctrine should develop to reflect our change in understanding of our role in this field. We must ensure that training and education include general and mission-specific skills and understanding. This will equip and inspire DMS members to provide effective DHE, both generally for contingency as well as for specific military tasks.
The Strategic Defence and Security Review (SDSR) 2015 established an Armed Forces DE career stream, highlighting the importance of this work for defence.3 Developing expertise in DHE is an opportunity for the DMS to develop world-leading military medical expertise in a global field of growing interest and importance.14 The DMS must ensure best practice is developed and maintained through research and innovation. This includes investment in education and training, highlighting both cultural and linguistic awareness. As the Surgeon General’s Research Priorities evolve over time, increased importance should be given to DHE. We must develop high-quality research into how to conduct DHE effectively from needs assessments, training requirements, high efficacy interventions, ethics and cross-cultural working. Such research is crucial to uphold the ethical principle of primum non nocere (first do no harm) and avoid examples of unintended harm from well-intentioned external medical interventions.11 The DMS should ensure individual development through supported placements with international partners. We must be ready to develop consultancy and mentoring skills, as well as support other UK health sector partners for provision of healthcare, including humanitarian assistance and disaster relief. Specific activities conducted and coordinated in pursuit of DHE might include joint medical training exercises and public health initiatives with overseas partners, empowering overseas laboratories to provide surveillance of biological threats and infectious disease research and humanitarian and disaster relief response.15 Currently, the DMS strategic direction for DHE is overseen by the Assistant Head International, within the Medical Operational Capability of the Surgeon General’s Headquarters (HQ SG). SDSR 15 also established a Centre for Defence Health Engagement within HQ SG.13
Conclusion
As General Houghton said as the Chief of the Defence Staff in 2014, “We need to employ the Armed Forces in such a way that not only do they ameliorate the risk of conflict through protection and deterrence, but they also enhance security through building stability overseas and through capacity building activities which contribute to the prevention of conflict.” 16 Assistance to fragile states via health services is non-contentious, accessible and can enable engagement when other defence actors may not be able to readily do so. DHE can therefore help reduce internal unrest, suppress the allure of violent extremism and reduce drivers for mass migration. The DMS is already widely engaged in supporting and delivering DHE. It is well placed to develop world-leading military medical expertise in the field and must exploit opportunities to increase expertise through development of DHE career streams, high-quality research and DHE-specific training and operations.
Footnotes
Contributors JW and DB contributed equally to this work.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.