Article Text

Statistics from Altmetric.com
Regular exercise has proven to be a healthy habit that decreases risk factors and atherosclerosis; however, it increases the risk of ventricular arrhythmias and sudden death in individuals with pre-existing cardiac diseases. Generalised pre-participation screening programmes are being increasingly implemented; however, their cost effectiveness has not yet been clearly established. More recently, data suggest that athlete's heart, secondary to long term endurance sport practice, may increase the incidence of arrhythmias, particularly atrial fibrillation (AF), atrial flutter, sinus node dysfunction, and eventually right ventricular tachycardia. Given the fact that an increasing number of individuals engage in regular endurance sport practice, it is certainly of great interest to define which recommendations for sport practice should be implemented in an individual patient and determine how best to manage arrhythmias in sport practitioners.
Sudden death in athletes with previous cardiac conditions
Sudden death among young athletes is uncommon, ranging from 0.5 to 3 per 100 000 per year.1 The prevalence of the underlying diseases in these cases remains controversial. In the US series, the major contributor to sudden death was hypertrophic cardiomyopathy (HCM) (figure 1),2 whereas in the Veneto series (northern Italy), right ventricular dysplasia (RVD) was the most prevalent disease. These differences were attributed to population prevalence of heart disease (RVD being highly prevalent in Italy) or to a more complete pre-participation screening policy in Veneto. In recent Australian necropsy studies, the authors did not find structural heart disease in most individuals. Therefore, a primary electrical abnormality was considered to be the leading cause. Although the exact prevalence of each abnormality is still under debate, it is clear that strenuous exercise in young individuals may precipitate fatal arrhythmias and sudden death in a number of cardiac structural diseases such as HCM, congenital coronary abnormalities, RVD, Wolff–Parkinson–White syndrome, channelopathies, etc. While the cost effectiveness of a generalised pre-participation screening for amateur athletes remains under discussion, cardiac evaluation before beginning regular, competitive engagement in sports is becoming very common. Therefore, in the coming years, most easily diagnosed conditions, such as HCM or pre-excitation syndromes, will be diagnosed frequently. However, the risk will remain in patients with less evident conditions, such as channelopathies, RVD with minor or no ECG changes, coronary abnormalities, etc.

Distribution of cardiovascular causes of sudden death in 1435 young competitive athletes from the Minneapolis Heart Institute Foundation Registry. ARVD, arrhythmogenic right ventricular dysplasia; AS, aortic stenosis; CAD, coronary artery disease; DCM, dilated cardiomyopathy; HCM, hypertrophic cardiomyopathy; HD, heart disease; LAD, left anterior descending artery; LVH, left ventricular hypertrophy; MVP, mitral valve prolapse. Modified from Maron et al. Recommendations and considerations related to preparticipation screening for cardiovascular abnormalities in competitive athletes: 2007 update: a scientific statement from the American Heart Association Council on Nutrition, Physical Activity, and Metabolism: endorsed by the American College of Cardiology Foundation Circulation 2007;115:1643.
The prevalence of sudden death during exercise in older athletes or in individuals practising regular endurance training is less well studied. However, it is well known that exercise poses an increased risk for sudden death in older individuals with pre-existing diseases,3 with necropsy studies showing that the main cause is coronary artery disease. Whether sudden death would have been avoided or delayed if they had avoided intense endurance training cannot be known, but it seems evident that older individuals should be carefully evaluated before and during their engagement in intense endurance training, whether competitive or not.
Figure 2 shows the possible mechanisms that may lead to an increased susceptibility to arrhythmias in individuals without previous cardiac disease.

Possible mechanisms leading to an increased susceptibility to atrial and ventricular arrhythmias in patients without previous cardiac diseases.
Syncope during exercise as a warning for athletes at risk for sudden death
The leading clinical symptom preceding sudden death in many individuals is syncope. Any syncopal episode taking place during or soon after exercise merits an intensive and extremely careful evaluation. Reviewing the circumstances of the episode with the individual and those who witnessed it may help in evaluating the severity of the episode. It is also very important to record carefully the degree of athletic training and the working conditions of the athlete suffering the syncopal episode. Quite often, non-professional athletes underwent unreasonable training without supervision, after a strenuous workday, which certainly creates the milieu for vasovagal syncope due to exhaustion and overtraining. A sudden syncope, without warning and with seizures or prolonged loss of consciousness, implies a potential severity; however, neuromediated or vasovagal syncope may also present as prolonged asystole, with seizures and sudden loss of consciousness.
An ECG and a careful echocardiographic evaluation may rule out the most evident causes, such as Wolff–Parkinson–White syndrome or HCM. However, other conditions may not be easily diagnosed. The exercise test should always be performed. It may reveal myocardial ischaemia, or even a polymorphic ventricular tachycardia due to catecholaminergic ventricular tachycardia—an inherited condition with serious potential for fatal ventricular arrhythmias. Other powerful diagnostic tools should be used judiciously, based on clinical suspicion, but it should be clear that a normal echocardiogram only excludes major structural diseases, whereas more subtle abnormalities may go undiagnosed. Computed tomography angiography (CTA) scanning may uncover a congenital coronary abnormality, and magnetic resonance imaging (MRI) with gadolinium enhanced contrast may reveal an RVD or localised myocardial scars of unknown aetiology, which may be the substrate of severe ventricular arrhythmias. Finally, a complete electrophysiology (EP) study may help if a sustained ventricular tachycardia is induced. However, if the patient reaches the laboratory without any clear suspicion of a diagnosis, the diagnostic yield of an EP study is low. In most channelopathies, such as long QT, there is no increased inducibility. Flecainide or ajmaline infusion may uncover a Brugada syndrome, although ventricular arrhythmias have not been clearly related to exercise in this channelopathy. The possibility of a vasovagal or neurologic origin must also be considered, but only after carefully excluding cardiac causes with a potential for sudden death.
Endurance training and athlete's heart
Longstanding endurance training results in heart adaptation. Such changes, described as athlete's heart, include atrial and ventricular dilatation, left ventricular (LV) hypertrophy, increased heart mass, sinus bradycardia, first and second degree atrioventricular (AV) nodal block, negative T waves, and J point elevation. At the atrial level, Pellicia et al4 reported an incidence of left atrial dilatation of 20% among competitive athletes, However, the study was performed in young athletes at the moment of highest activity; long term follow-up studies on atrial changes are scarce.
Whether athlete's heart is merely adaptive or may have negative long term consequences is still being debated. LV hypertrophy secondary to endurance training may be extreme, although partially reversible upon sport cessation.5
Recent experimental data from our group shows that, on top of LV hypertrophy, endurance exercise may induce fibrosis in a rat model of chronic exercise, particularly at the atrial and right ventricular level. Therefore, it seems that endurance exercise may induce pathological changes in the heart, at least in an experimental model. A recent study by Lindsay and Dunn has shown an increase in humoral markers of fibrosis in veteran athletes as compared to normal sedentary subjects, suggesting that long term sport practice may provoke fibrosis as part of the hypertrophic process in veteran athletes.6 Alternatively, also based on experimental evidence, it has been proposed that exercise would only contribute to uncovering a genetic predisposition. For example, it has been shown that exercise only induced right ventricular changes in a series of rats with a mutation, whereas it did not provoke changes in normal rats.7 Long term follow-up data are needed to study further long term consequences of athlete's heart.
Sudden death in athletes
Annual incidence ranges from 0.5 to 3 per 100 000.
In the USA, the major contributor to sudden death in young athletes is hypertrophic cardiomyopathy, whereas right ventricular dysplasia is the leading cause in Italy.
Strenuous exercise may precipitate fatal arrhythmias in individuals with previous cardiac diseases.
The main cause of sudden death during exercise in older individuals is coronary artery disease.
Any syncopal episode occurring during or soon after exercise deserves intense and careful evaluation, since it may be caused by a malignant ventricular arrhythmia.
Exercise testing is essential in the diagnostic work-up of exercise related syncope, if other causes of syncope such as hypertrophic cardiomyopathy, aortic stenosis, right ventricular dysplasia, etc, have been excluded.
Atrial arrhythmias and endurance exercise
In recent years, an association has been demonstrated between endurance sport practice and AF or atrial flutter (table 1, figure 3). In 1998, Karjalainen et al were the first to publish a longitudinal prospective study establishing a relationship between endurance sport practice and AF in a series of orienteers (a form of cross country running).8 After 10 years of follow-up, AF incidence among orienteers was 5.3%, compared to 0.9% among the control subjects. Therefore, the incidence of AF was unusually high in a series of middle aged endurance sport practitioners without predisposing factors. The odds ratio (OR) for lone AF associated with vigorous exercise was 5.5 (95% confidence interval (CI) 1.3 to 24.4) in their study.
Studies demonstrating an increased risk for atrial fibrillation (AF) in individuals practising endurance sports

Atrial flutter and atrial fibrillation often co-exist in patients with lone atrial fibrillation who practise endurance sports. Panel A shows common atrial flutter that spontaneously changes into atrial fibrillation (panel B).
A retrospective analysis of our series of lone AF patients seen at the outpatient arrhythmia clinic showed that the proportion of regular sport practice among men with lone AF was much higher than among men from the general population (63% vs 15%).9 Regular endurance sport practice was defined as more than 3 h a week of endurance training at the moment of evaluation. The same population of lone AF patients was analysed in a case–control study with two age matched controls from the general population for each case. The analysis showed that current sport practice more than quintupled the risk of developing lone AF (OR 5.06, 95% CI 1.35 to 19). The association of current sport practice with lone AF was observed at more than 1500 lifetime hours of sport practice, suggesting the existence of a threshold point.10 Another study involved 183 individuals who ran the Barcelona marathon in 1992 and 290 sedentary healthy controls.11 Endurance sport practice was associated with a higher risk of incident lone AF in the multivariable age and blood pressure adjusted Cox regression models (hazard ratio 8.80, 95% CI 1.26 to 61.29).10 Recently, Baldesberger et al12 published a study performed in a cohort of 64 former Swiss professional cyclists. These athletes were compared with a control group of 62 male golfers. Individuals were matched for age, weight, hypertension and cardiac medication. The mean age at examination was 66±7 years. Former cyclists showed a lower heart rate and a higher incidence of AF or atrial flutter (10% vs 0%, p <0.028) and non-sustained ventricular tachycardia. These data suggest that the incidence of AF in athletes further increases with ageing, as with any kind of AF.
Very recently, Aizer et al reported that regular vigorous exercise was associated with an increased risk for AF, in a cohort of 16 921 healthy men, enrolled in the Physician's Health Study.13 These results further confirm previous observations seen in small case–control studies.
Mechanisms of AF and flutter in endurance sports
Several mechanisms have been proposed to explain the increased incidence of AF in athletes.14 It is well accepted that arrhythmias depend on triggers, substrates and modulators, and these factors may be present in relation to physical activity. Atrial ectopy, particularly pulmonary vein ectopy, has been shown to be the trigger in most episodes of paroxysmal AF. Several reports suggest that ectopy is increased as a consequence of physical activity. On the other hand, increase in vagal tone may act as a modulator, increasing the vulnerability of the atrium to AF.
Coumel studied the influence of autonomic innervations in the appearance of AF and atrial flutter. He first described vagal AF as a type of AF with a clear male predominance, with the crisis taking place during the night or in a postprandial state, particularly after dinner.15 The author concluded that AF occurred in a vagal context, but an unidentified substrate probably existed. However, he did not establish a relationship between these episodes of AF and sport practice. Experimental data show that increased vagal tone shortens atrial refractory period and increases AF dispersion, creating the conditions for re-entry. In clinical practice, vagal AF is considered to be a rare presentation of AF. This is probably due to the lack of systematic enquiry with patients.
In the GIRAFA study of patients with lone AF, vagal AF was the rule rather than the exception (about 70% of consecutive lone AF patients had vagal AF).16 Therefore, the increased vagal tone induced by endurance sport practice may indeed facilitate the appearance of AF. Finally, long term endurance sport practice may induce structural changes in the atrium (enlargement, fibrosis) that may create a favourable substrate for the disease. In fact, Frustaci et al found structural changes in a series of 12 patients with paroxysmal, recurrent, drug refractory lone AF.17 The authors described inflammatory lymphomononuclear infiltrates, compatible with myocarditis, and patchy fibrosis in a significant number of atrial biopsies.
A recent review of the literature by Swanson18 shows that excessive endurance exercise and overtraining can lead to chronic systemic inflammation and there is a relationship between AF and C reactive protein. The data from the GIRAFA study16 showing that patients with lone AF had a larger atrium compared to controls suggests that subtle structural changes at the atrial level may account for the appearance of AF. On the other hand, patients with AF had larger LV mass, even after normalising for body surface area. This further supports the suggestion that exercise also has some repercussions for the ventricles, but without differences in diastolic function index as compared to controls. Although diastolic dysfunction has been proposed as the mechanistic background for atrial enlargement, it seems that volume and pressure overload act directly in the atrium, even before acting at the ventricular level.
Clinical characteristics of sport related AF
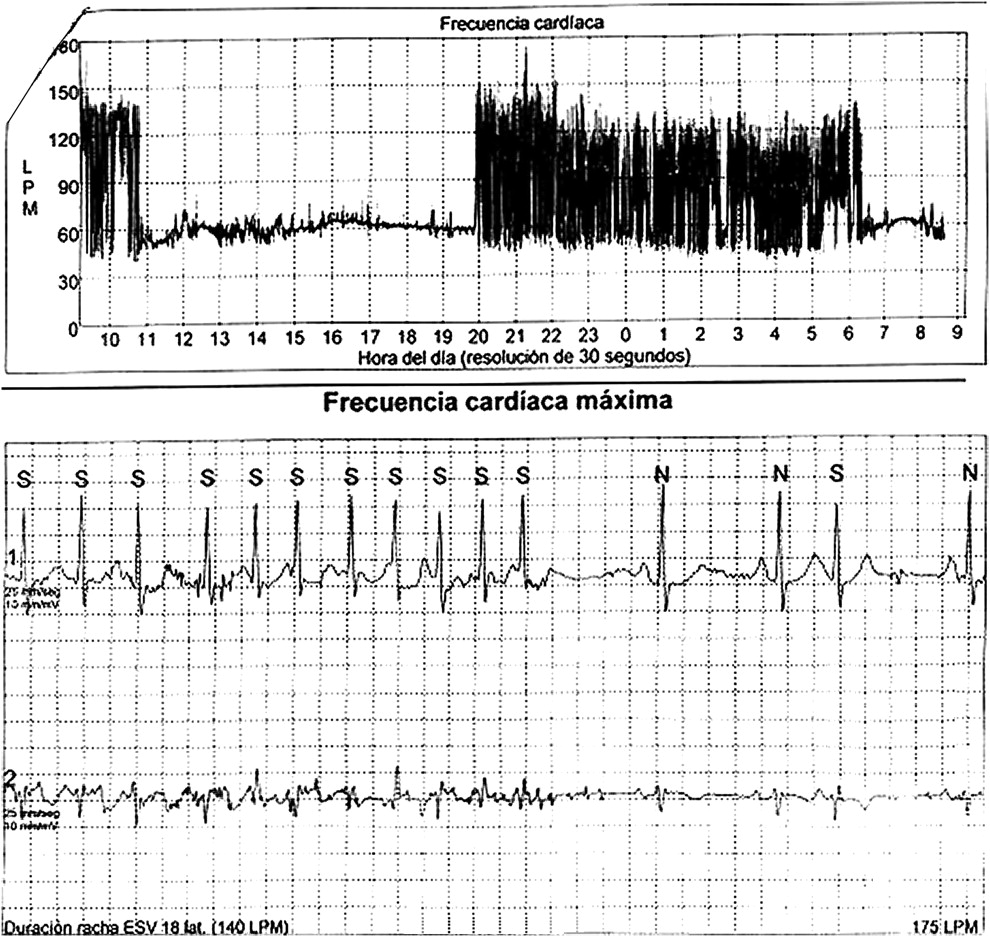
The typical clinical profile of sport related AF is a middle aged man (in his 40s or 50s) who has been involved in regular endurance sport practice since his youth and is still active. The AF is usually paroxysmal with crisis, initially occurs very occasionally and is self limited, and progressively increases in frequency and duration. Characteristically, AF crises occur at night or after meals (figure 4), and seldom occur during exercise. This makes the patient reluctant to accept a relationship between the arrhythmia and sport practice, particularly since his physical condition is usually very good. Usually the crises become more frequent and prolonged over the years and AF becomes persistent. The AF crisis frequently co-exists with common flutter.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Vagal atrial fibrillation (AF) often starts after dinner or at night and remains throughout the night until the patient wakes up. The Holter recording shows a prolonged AF episode that started after dinner at 8 pm.
Therapeutic measures
Data on the reversibility of arrhythmia upon sport cessation are scarce. Our personal observations, although not systematic, suggest that limiting physical activity seems to reduce significantly the number of crises, particularly in those with recent onset and when the atrium is not very dilated. While waiting for clinical studies, it seems reasonable to advise a significant reduction in endurance sport practice in these patients.
Whether drugs to prevent cardiac hypertrophy (angiotensin converting enzyme inhibitors, angiotensin receptor inhibitors or β-blockers) play a long term role remains to be elucidated. In terms of arrhythmia prevention, patients with recurrent episodes have been treated with flecainide and diltiazem, preventing 1:1 atrial flutter secondary to flecainide with good results. Some of them had undergone AF ablation, with a success rate similar to patients not involved in endurance sport practice. In patients with predominant atrial flutter, ablation of the flutter is frequently associated with a higher incidence of AF recurrences, as pointed out by Heidbuchel et al.19
Bradycardia and AV conduction disturbances in endurance sport practitioners
Sinus bradycardia and first and second degree AV block (Wenckebach type) are considered to be merely a physiological adaptation to sports that requires no special attention. On the other hand, second degree AV block Mobitz II, advanced or third degree AV block are considered pathological conditions that require a pacemaker implant. However, reversibility of these conditions upon exercise restriction or cessation has not been investigated. Furthermore, data on long term follow-up of athletes are scarce. Recent data suggest that longstanding endurance training, particularly cycling, may predispose to bradyarrhythmias in the long run. Baldesberger et al found sinus node dysfunction, defined as bradycardia of <40 beats/min, in 10% of a series of professional cyclists seen 20 years after riding the Swiss Tour, as compared to 2% of age matched golf players.12 The authors suggest that endurance training in itself may provoke changes that in the long run became irreversible.
Ventricular arrhythmias and sport practice
Sport practitioners seem to have an increase in ventricular premature beats. On the other hand, the number of ventricular premature beats dramatically decreases upon exercise restriction.20 This condition has been considered a benign arrhythmia without pathological consequences. However, Heidbuchel et al described a subset of athletes, mainly cyclists, referred for evaluation of ventricular arrhythmias and alerted us that, in that particular series, most arrhythmias came from the right ventricle.21 The presence of previous syncope, as well as inducibility to sustained ventricular arrhythmias at the EP testing, poses an increased risk for sudden death. The authors raised the hypothesis that endurance training in itself may induce a kind of ‘acquired’ RVD, due to chronic volume overload. In fact, many patients showed subtle changes in the right ventricle that cannot be considered a fully developed type of RVD.22 While awaiting a more definitive answer, particular care should be taken in the evaluation of patients with documented ventricular arrhythmias and endurance practice, particularly if the patients suffered syncope. EP study may select a subgroup of patients with an increased risk for sudden death and a potential need for an implantable cardioverter-defibrillator (ICD).
Athlete's heart and arrhythmias
Athlete's heart may cause some degree of atrial and ventricular dilatation, increased left ventricular mass, first and second degree atrioventricular nodal block, negative T waves and J point elevation that are often considered physiologic adaptation to exercise.
Regular long term endurance sport training may increase the risk for atrial flutter and atrial fibrillation.
Atrial fibrillation in athletes is initially paroxysmal, and most episodes are vagally mediated (taking place at night, or at rest, after meals).
It has been suggested that in some individuals, intensive and long term endurance sport practice may create a substrate for right ventricular arrhythmias.
Experimental data suggest that endurance practice may increase fibrosis, that can result in a substrate for atrial and right ventricular arrhythmias.
Sport activities in patients with a defibrillator
Because of the increasing number of ICDs being implanted in young and physically active individuals, there is an increasing controversy over whether these individuals should be allowed to practise sports, and with what intensity. A large multicentre study has been developed to record data in such individuals and offer recommendations.
Endurance training and highly demanding cardiovascular activity may pose a risk in these individuals in two different ways. First, exercise may induce severe ventricular arrhythmias that do not always respond to defibrillation, as they may occur in HCM, catecholaminergic ventricular tachycardia, long QT, etc. On the other hand, exercise can provoke inappropriate defibrillator therapies that, in addition to worsening quality of life and inducing psychological stress, may also induce ventricular arrhythmias.23
Exercise often implies repetitive movement of limbs. Lead fractures are more often seen in young patients, due to high activity related to movement. Therefore, certain physical activities may superimpose a risk of system malfunction.23
Conclusions
Regular exercise is a healthy habit that decreases the risk of coronary artery disease, and even the risk of AF in elderly patients, by controlling risk factors. On the other hand, exercise increases the risk of sudden death in patients with pre-existing cardiac diseases. Furthermore, recent data suggest that athlete's heart may create the substrate for atrial and ventricular arrhythmias. Therefore, judicious degrees of physical activity should be recommended, adapted to the patient's age, work activities, etc. Uncontrolled and intense endurance practice at a certain age may have long term deleterious effects, although data obtained in large epidemiological studies are needed to prove this observation definitively.
You can get CPD/CME credits for Education in Heart
Education in Heart articles are accredited by both the UK Royal College of Physicians (London) and the European Board for Accreditation in Cardiology—you need to answer the accompanying multiple choice questions (MCQs). To access the questions, click on BMJ Learning: Take this module on BMJ Learning from the content box at the top right and bottom left of the online article. For more information please go to: http://heart.bmj.com/misc/education.dtl
RCP credits: Log your activity in your CPD diary online (http://www.rcplondon.ac.uk/members/CPDdiary/index.asp)—pass mark is 80%.
EBAC credits: Print out and retain the BMJ Learning certificate once you have completed the MCQs—pass mark is 60%. EBAC/ EACCME Credits can now be converted to AMA PRA Category 1 CME Credits and are recognised by all National Accreditation Authorities in Europe (http://www.ebac-cme.org/newsite/?hit=men02).
Please note: The MCQs are hosted on BMJ Learning—the best available learning website for medical professionals from the BMJ Group. If prompted, subscribers must sign into Heart with their journal's username and password. All users must also complete a one-time registration on BMJ Learning and subsequently log in (with a BMJ Learning username and password) on every visit.
References
- ↵
This study reviews the potential beneficial effect of a generalised pre-participation screening programme.
- ↵
Maron et al report the cause of sudden death in young competitive athletes, based on registry data.
- ↵
A seminal study proving that physical exercise may act as a trigger for myocardial infarction.
- ↵
This study analysed the prevalence of left atrial remodelling in young competitive athletes. As many as 20% fulfilled criteria for atrial dilatation.
- ↵
In this study, Pelliccia et al proved that left ventricular hypertrophy secondary to intensive training in athletes may be partially reversible by limiting physical activity.
- ↵
These investigators found a higher value of fibrosis markers in the blood of veteran endurance athletes. Whether this relates to increased ventricular fibrosis remains to be elucidated.
- ↵
Kirchhof et al proved that exercise may uncover a pre-existing genetic defect that was not manifest in mice that did not undergo exercise.
- ↵
Kaarjalainen et al found for the first time an increased prevalence of AF among orienteers (endurance cross-country runners), in a 10 year follow-up study.
- ↵
This study found that endurance sport practice was much more prevalent among patients with lone AF compared to the general population.
- ↵
Elosua et al found that long term endurance sport practice increases the risk of AF. The two most powerful predictors were >1500 h of endurance training and being involved in endurance training at study entrance.
- ↵
This long term follow-up study showed an increased risk of AF in marathon runners as compared to sedentary individuals recruited from the general population.
- ↵
A long term follow-up study that proved an increased incidence of AF and flutter in former professional cyclists as compared to golf players.
- ↵
- ↵
A review of the present knowledge establishing the relationship between endurance training and AF.
- ↵
Coumel described for the first time the so-called ‘vagal atrial fibrillation’, giving a detailed clinical description. However, he did not establish any association with endurance training.
- ↵
GIRAFA was a confirmatory study in patients seen at the emergency room with lone AF. Endurance training as well as taller stature and atrial size increased AF risk.
- ↵
This study found histological changes in biopsies obtained in patients with lone AF. Due to the difficulty in obtaining tissue samples in such patients, data in the literature are scarce.
- ↵
An in depth review of the literature that suggests interesting connections between overtraining and inflammation that may be a contributory effect for AF in athletes.
- ↵
Heidbuchel et al found an increased incidence of AF after successful flutter ablation among endurance athletes.
- ↵
This study proved that deconditioning may significantly decrease the ventricular arrhythmia load in athletes with frequent premature beats and non-sustained ventricular tachycardias.
- ↵
This study revealed a high prevalence of right ventricular involvement with potentially serious ventricular arrhythmias and sudden death in a cohort of endurance athletes evaluated for ventricular arrhythmias.
- ↵
Ector et al found structural changes in the right ventricle of endurance athletes evaluated for ventricular arrhythmias, suggesting a causal relation between endurance exercise and structural remodelling.
- ↵
Maron and Zipes gave their expert opinion on the need to restrict physical activity in patients with ventricular arrhythmias treated with an implantable defibrillator.
Supplementary materials
Web Only Data 96/5/398
Files in this Data Supplement:
Footnotes
Competing interests In compliance with EBAC/EACCME guidelines, all authors participating in Education in Heart have disclosed potential conflicts of interest that might cause a bias in the article. The author has no competing interests.
Provenance and peer review Commissioned; not externally peer reviewed.