Article Text

Statistics from Altmetric.com
The article, ‘A pilot study of an Enhanced Mental Health Assessment during routine and discharge medicals in the British Armed Forces’,1 published in this edition of the JR Army Med Corps, produced some interesting results regarding alcohol consumption in the armed forces, which we would like to discuss in more detail.
The UK military has a historical relationship with alcohol.2 One recent study found that the ‘prevalence of alcohol-related harm and alcohol dependence within the UK Armed Forces is greater than in the general population’.3 This study and several others have supported the belief that military personnel consume more alcohol than civilians when using comparable populations.4 ,5 Alcohol consumption is part of the UK military culture and may foster social cohesion when consumed in moderation.6 However, the health implications of excessive alcohol consumption are significant. Iversen et al noted that alcohol misuse was often comorbid with neurotic problems in the UK military7 while Verrall found that when consuming alcohol at a risky level, there could be adverse physical, mental and psychological health outcomes associated with combat exposure.2 In addition, the media mainly focus on post-traumatic stress disorder as an adverse mental health outcome from military service, whereas the reality is that the most frequent mental health problems for veterans are alcohol use disorders, depression and adjustment disorders.8
Our pilot study1 used a questionnaire during routine and discharge medicals at four military medical centres and specifically included three questions from the Alcohol Use Disorder Identification Test Consumption (AUDIT-C),9 a validated alcohol misuse screening tool where a total score of 5 or more indicates higher risk drinking; it is however noteworthy that validation data of the AUDIT-C within a military population have not been published. The results from the pilot study revealed that 65% of service personnel had an AUDIT-C score >4, indicating ‘higher risk drinking’ (Figure 1).

Alcohol Use Disorder Identification Test (AUDIT-C) scores. Percentages of patients scoring 0–12. A score of 5 or higher (65%) indicates higher risk drinking.
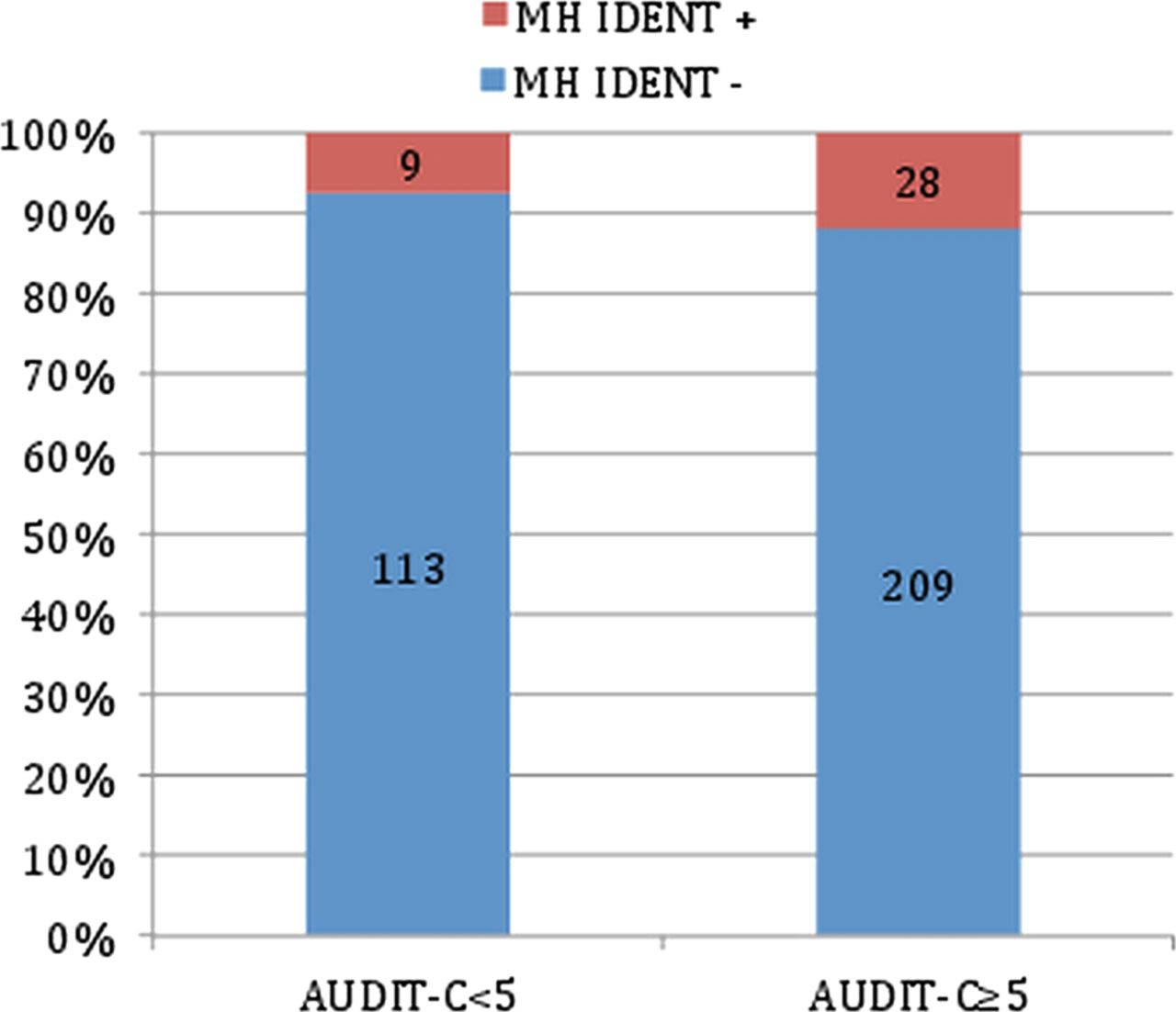
We analysed correlations among the AUDIT-C scores, frequency of drinking alcohol and identification of possible mental health problems using standard brief survey tools for depression, anxiety, post-traumatic stress disorder, sleep problems and irritability. We found that those personnel with more risky drinking habits were more likely to be identified as having possible mental health problems. Figure 2 demonstrates that personnel with an AUDIT-C score of ≥5 (n=237) were identified as having possible mental health problems more frequently (11.8% vs 7.4%) than those scoring 4 or less (n=122). In addition, we found that the 45 personnel who reported drinking alcohol more than four times per week were twice as likely to report positive scores on the brief mental health survey tools than those who did not (20% vs 10%).
{kind=link}
{kind=link}
Identification of potential mental health problems related to Alcohol Use Disorder Identification Test (AUDIT-C) scores.
As part of the Enhanced Mental Health Assessment (EMHA) process, all those identified as having potential mental health problems, including risky alcohol use, were offered assistance. As a minimum, these patients were offered health and lifestyle advice. The EMHA could therefore be viewed as a form of screening and brief interventions (SBI). SBI for alcohol misuse disorders have been shown to be effective in primary care in non-military populations.10 ,11 With the addition of a formalised brief intervention, the EMHA may offer an opportunity to improve the drinking habits and, as demonstrated in our paper,1 the mental health of the armed forces population in the UK.
So, what are the implications for clinicians?
A score of 5 of more on AUDIT-C suggests possible risky alcohol consumption and should lead to completion of the full 10 question AUDIT questionnaire (AUDIT-C comprises of three questions. AUDIT is a 10-part questionnaire). A score of 8 or more on AUDIT confirms hazardous alcohol consumption as very likely to be present. A score of 16 or more is highly suggestive of harmful alcohol use (ICD-10 code F10.1).
Hazardous alcohol consumption requires a brief intervention, which can be as simple as a few minutes of discussion about potential harm of alcohol use and/or provision of a patient information leaflet. Good medical practice would be to review several weeks later to ascertain whether the person has altered his/her behaviour. Harmful alcohol use warrants the same, as well as a full mental health assessment, as comorbid mental health conditions will be common. It is also important to consider any occupational risks of alcohol misuse. Once a full assessment has been carried out, the clinician must discuss with the patients what they would like to do about their alcohol misuse. A referral to Defence Community Mental Health should be considered in these cases.
Acknowledgments
We would like to thank Brigadier Cordell (DMS Head of Medical Strategy and Policy) for his support throughout this project. We would also like to thank Michael Rowe (Military Medical Librarian, Defence Medical Library Services) for his support with literature searches and background research, Amarjit Samra (Director of Research, JMC Medical Directorate) for invaluable advice on conducting research and Anna Brown (Operations Manager, JMC Medical Directorate) for support with data analysis.
Footnotes
-
Contributors MA drafted the manuscript. However, every author contributed to the writing of the manuscript, the data analysis and the charts.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; internally peer reviewed.