Article Text

Abstract
Objectives Historically, burns have formed a significant proportion of the casualties of war. The management of burns in recent conflict has been found to be a resource-heavy undertaking, though its impact on both personnel and resources in current conflicts is unclear. A case analysis has been carried out in order to quantify the logistical impact of the management of burns on Role 3 Medical Treatment Facility (MTF) infrastructure and to examine if and how the cause and management of burns have evolved in early 21st century conflict.
Methods All casualties treated for burns at a Role 3 MTF over one calendar year were identified and scanned copies of their notes obtained from the UK Joint Theatre Trauma Registry and retrospectively analysed.
Results 88 of the 1461 (6.0%) trauma patients presenting to the Role 3 MTF over the year were treated for burns of whom 52.3% were combat troops and 45.4% civilians. Half of the burns were caused by non-conflict related mechanisms; the two commonest mechanisms were flame burns in 38/88 mostly non-conflict related cases and blast in 30/88 cases most of which were conflict related.
Conclusions The management of burns at war is a complex process. It is further confounded by the management of civilians with non-conflict related burns, which places a predictable strain on Role 3 MTF resources: theatre time, nursing time, dressing resources and bed space. This must be planned for in current and future deployed operations.
Statistics from Altmetric.com
Key messages
-
Burns now account for 6% of injuries sustained at war.
-
The mechanism of burn injuries has evolved with thermal injuries now more frequently sustained from improvised explosive devices rather than within confined fighting vehicles.
-
Managing civilians with non-conflict burns has a recognisable logistical impact, which must be accounted for in future planning estimates.
Introduction
Historically, burns have formed a significant proportion of casualties of war, varying between 5% and 20%;1 ,2 between World War II (WWII) and the start of the Gulf War in 1991 burns were responsible for approximately 4% of combat mortality.3 ,4 Although 14% of UK casualties during the 1982 South Atlantic campaign were burns,5 ,6 recent US figures estimate the numbers of thermal injuries seen in Iraq and Afghanistan at 5%.7–10
Previously, a greater incidence of thermal injury was reported in troops working within the confines of air-, sea- and land-based fighting vehicles, compared with infantry troops, with figures of up to 47% reported in WWII US Army tank crews.1 ,3 ,4 As conflict has evolved, ground troops have been exposed to a changing pattern of injuries: penetrating injuries predominate and are currently more frequently sustained from improvised explosive devices (IEDs) than gunshot wounds11 and here they face an increasing risk of thermal injury.
In recent conflict, the management of burns at war has been found to be a complex undertaking, with the logistical burden of managing these patients in military facilities proportionally exceeding the number of patients with burns.7
A case note analysis has been conducted looking at all patients managed with burns in a North Atlantic Treaty Organisation (NATO) Role 3 Medical Treatment Facility (MTF) over one calendar year, with three aims: to examine how the cause and management of burns has evolved in early 21st century conflict; to quantify the logistical impact of the management of burns on Role 3 MTF infrastructure; and to assess the proportion of local national casualties treated with non-conflict related burn injuries.
Methods
Permissions were granted from the Joint Combat Casualty Research Team and the US Army Institute for Surgical Research in San Antonio, Texas. Scanned copies of hospital notes were obtained for all burns casualties treated at a Role 3 MTF in 2010 from Trauma Nurse Coordinators and the UK Joint Theatre Trauma Registry (JTTR). Overall casualty figures for the year were provided by the Academic Department of Military Emergency Medicine.
All patients presenting to the Role 3 MTF with a coding of burn injury between 1 January 2010 and 31 December 2010 were included in the analysis, regardless of status and mechanism. Patients sustaining burns who were treated elsewhere, such as Role 1 facilities, were not included. A retrospective analysis of the notes was carried out and a database created using FileMaker Pro. Descriptive statistics were performed and inter-group differences were examined for statistical significance using StatPlus:mac software, with p values <0.05 deemed to be statistically significant.
Results
In 2010, 1461 trauma cases were recorded on JTTR, 88 of whom (6.02%) were treated for burns at the Role 3 MTF, constituting 2.1% of total operating procedures and 8.0% of inpatient stay for the year. The 58 patients with burns and no other injuries accounted for 4.0% of all trauma cases, 1.5% of operating procedures and 6.4% of inpatient stay.
The 88 burns casualties were divided approximately equally between combat troops and civilians (Table 1) and the majority were male (76/88; 86.4%).
The combatant status of burn casualties treated over 1 year
Age was documented in 80 patients, with a mean age of 19.3 years (median 19.0, range 8 months–50 years); the eight remaining patients had no age documented but were all UK/US troops, and so must be at least 18-years-old, meaning that 31 patients (35.2%), all civilians, were under the age of 18 years of age. The distribution of burn casualties varied between 2 and 11 per month (Figure 1) and they had a median time from point of injury to presentation at the MTF of 2.25 h (IQR 1.2–12, range 0.1–504 h) (Table 2). There was no significant difference in time to presentation between military and civilian casualties.
Median time in hours from point of burn injury to presentation at the Role 3 Medical Treatment Facility
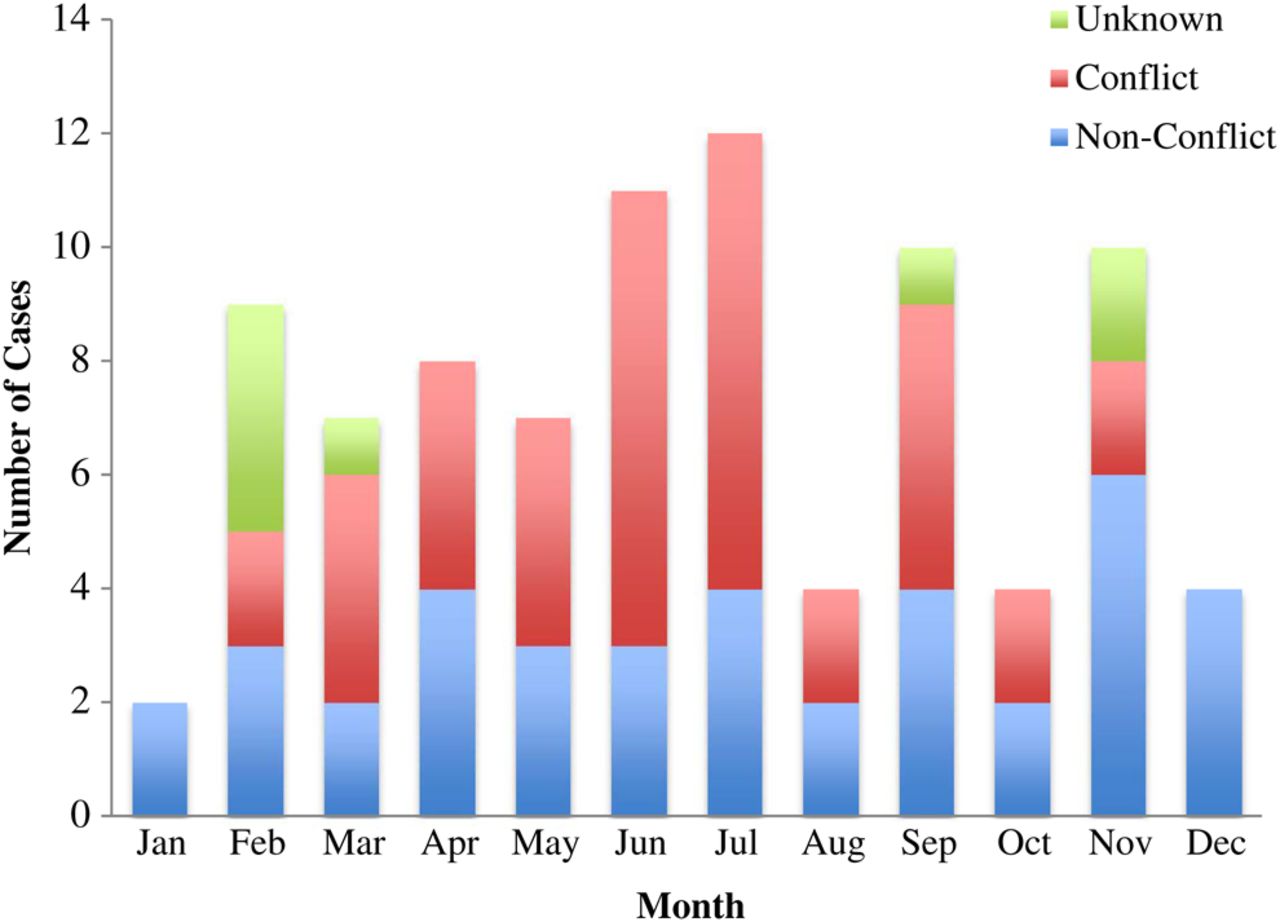
The distribution of casualties over the year by relationship of burn to the conflict.
The majority of patients, 52/88 (59.1%), were transported by air on Medical Emergency Response Team helicopters, US Pedro helicopters or non-specific ‘dust-off’ aircraft (Other Air) (Figure 2).
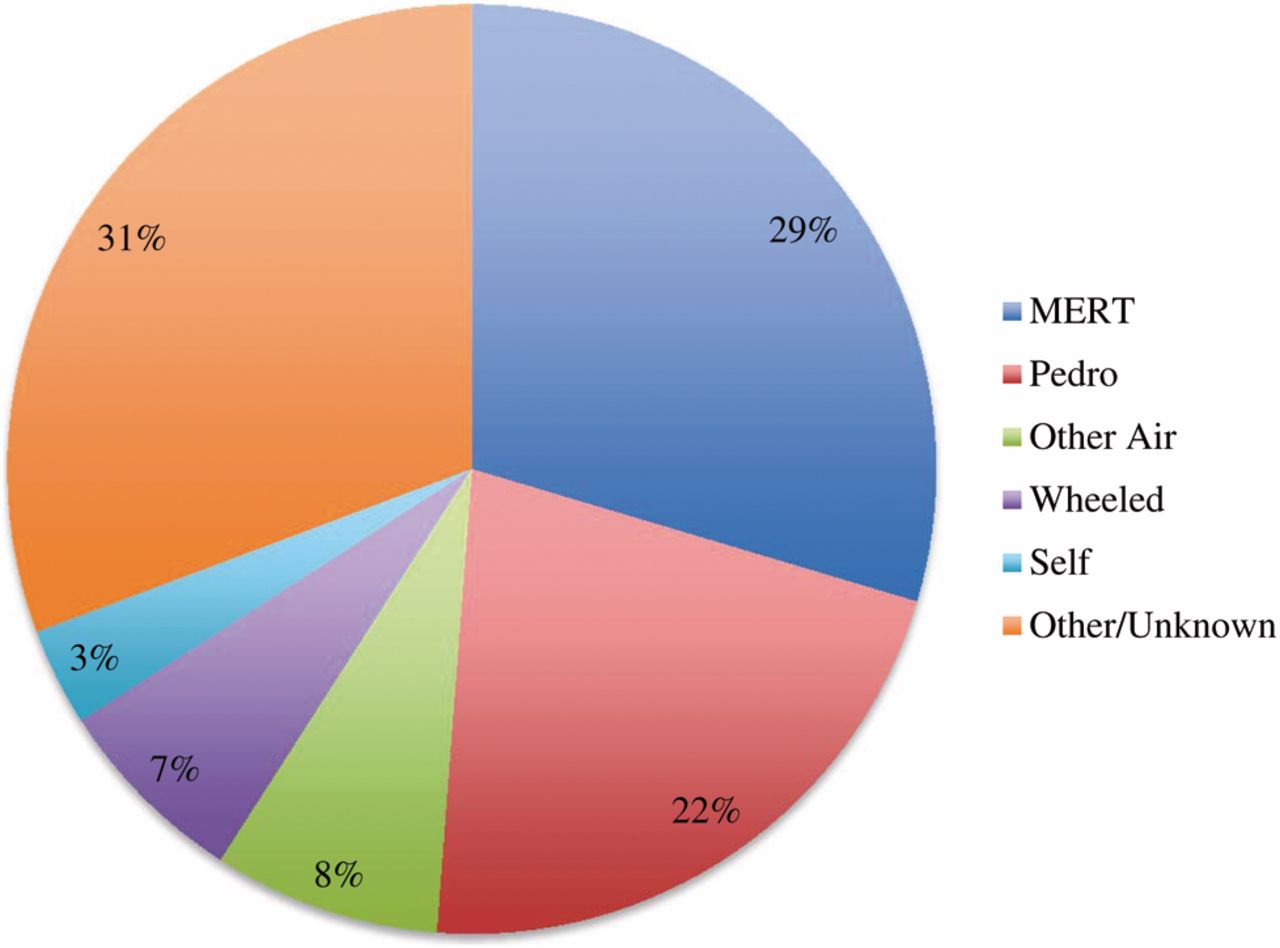
The method of presentation of burn casualties to the Role 3 Medical Treatment Facility.
Burn injury
The mechanisms of burn injury are shown in Figure 3; 36/88 were conflict related, with troops twice as commonly injured as civilians and non-conflict related in 44 cases, spread equally between combatants and civilians; the mechanism was unknown in eight cases.

The mechanisms of all burn injuries sustained presenting to the Role 3 Medical Treatment Facility over the year.
Flame burns were the most common, with 31/38 (81.6%) affecting civilians—the seven military flame burns were all from helicopter crashes and were the only military burns out of a total of 46 that occurred in vehicles. In combat troops, 10/17 cases (58.8%) of non-conflict related flame burns resulted from waste burning, five of whom required repatriation. In civilian flame burns, house fires and accidents with fuel were the most common causes. Blast was the second most common mechanism and was conflict related in 29/30 cases (96.7%) from IEDs, grenade blast and indirect fire. Civilians sustained 6/10 (60%) scald burns, all non-conflict related.
More than half the cases had less than 15% body surface area (BSA) burns with 11 cases (12.5%) greater than 40% BSA burns, including five with 100% BSA burns following helicopter crashes (Figure 4). There was no statistically significant difference in % BSA between conflict and non-conflict related burns (Table 3). Burn depth was difficult to classify, as many of the burns sustained were of mixed depth. They were predominantly sustained to the extremities in both conflict and non-conflict burns (Table 3).
The percentage body surface area (BSA) of burn injuries and distribution by body region according to conflict status (excluding eight cases of undocumented BSA)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
The distribution of burn extent in all casualties presenting with burns to the Role 3 Medical Treatment Facility over 1 year.
Twelve cases had confirmed signs of inhalation burns and were intubated, while a further six were intubated, either pre-emptively or due to the severity of other injuries without evidence of inhalation burns. Seven of the 12 (58.3%) patients with confirmed inhalation burns died. A total of 64 patients (72.7%) presented with burns as their only injury while 24 (27.2%) had other injuries, of which soft tissue fragmentation injury (15.9%), fractures (12.5%), lower limb amputation (7.9%) and upper limb amputation (4.5%) were the most common.
Inpatient and ICU stay
There was no significant difference between inpatient stay in conflict and non-conflict related burns in the 77 patients who were admitted; there was a difference in the length of inpatient stay between combat troops and civilians in non-conflict related burns (p=0.02) (Table 4).
Inpatient stay of patients with all burn injuries and non-conflict related burns according to combatant status
The presence of other injuries significantly increased the median length of inpatient stay compared with isolated burn injury (2 vs 1 day, p=0.04). Admission to the intensive care unit (ICU) was required in 31/88 (35.2%) patients, 61.3% of whom had an isolated burn injury. There was no significant difference in length of ICU stay between patients presenting with burns only or burns with other injuries or between any of the different groups (Table 5).
The intensive care stay of patients with burn injuries
The total operating time was significantly greater in patients with burns and other injuries when compared with patients with burns alone (p=0.04) (Table 6). Overall, 32 patients (36.4%) were transferred to the local healthcare system and 21 (23.8%) were returned to their units or discharged. In all, 19 (21.6%) were aeromedically evacuated and 13 (14.8%) died of wounds, seven of whom had burns with no other documented injuries. The outcome of three patients was not recorded.
The operating time (not including anaesthetic or recovery time) and number of procedures for patients with isolated burn injury and patients with burns and other injuries (excluding four patients with incomplete documentation)
Discussion
During the year approximately 6% of all trauma casualties presenting to the MTF had burn injuries, which is in line with recent US figures from Iraq and Afghanistan.7–10 The number of patients with burns may be under-reported, due to burn injuries being unrecorded because of significant other distracting injuries with a higher priority for immediate management.8 ,12 In addition, there are likely to be many burns managed outside of the Role 3 MTF, further contributing to under-reporting. In keeping with previously identified trends, the incidence of non-conflict casualties was higher than conflict related,13 with 50% of the former seen against 40.9% of the latter. Notably, a quarter of all burns cases were civilians presenting with non-conflict related burns.
Mechanism
In this study, as in others, a large number of non-conflict related flame burns in troops resulted from waste burning, previously found to be the most common cause of burns in troops.7 ,14 Our data shows that currently IED blast related burns outnumber waste burning injuries (21 vs 19). This may reflect either better education and personal protective equipment around waste burning or an increase in IED injuries reflecting the evolution of operations and threat. In line with evolving 21st century conflict, only 15% of burns were sustained in confined vehicles compared with 47% in WWII.1 ,3 ,4
Mechanisms of non-conflict related burns in civilians, such as house fires, scalds and fuel related accidents, were consistent with that expected from the breakdown in infrastructure in Afghanistan.
Pattern of injury
Historically, the incidence of burns in combat has been the highest in uncovered areas such as the hands and face.8 ,9 ,12 Current experience shows that burns to the peripheries and exposed areas continue to be common; however, the pattern of injury has changed. In conflict related burns, the head and neck are now the most commonly affected areas, which is in line with the increasing incidence of head and neck injury in 21st century conflict in general.15 Hands are no longer the most affected area, now involved in approximately a third of conflict related burns compared with 80% of cases in 2006.8 This may be attributable to an increase in the use of protective gloves, which Israeli data have shown to successfully reduce the incidence of hand burns.16 Lower limb burns, previously half as prevalent as upper limb burns, are now on an even par. This may be attributed to the evolving mechanism of injury, with many IEDs causing blast from the ground upwards when initiated.
In line with previous findings in terror related burns, 60% of blast burns patients had other injuries, all fragmentation related, leading to traumatic limb amputations in four cases.17 ,18 Burn casualties had other injuries in 28.4% of cases due to conflict related burns in all but one case, which is lower than expected.9 ,10 ,19 This may be due to a lack of documentation; for example, no other injuries were documented in the fatal cases from helicopter crashes, though they would have been expected.
Management implications
The resource implications of managing burn patients are related to the status of individual sustaining the burn. Most patients were admitted (87.5%), with two-thirds of inpatient stay used by civilians, nearly three-quarters of which was related to non-conflict burns. For all burns patients, two-thirds of operating time was used for civilian casualties, half of which was dedicated to the management of civilians with non-conflict related injuries.
Military
The management of burns in Allied forces has changed since the Falklands conflict, where troops sustaining burns frequently underwent excision and grafting of their burn, followed by a graft check at 7 days before evacuation to the UK.5 Over the year, no International Security Assistance Force (ISAF) troops underwent excision and grafting in Afghanistan, due to the high resource requirement and need for blood products,20 and the knowledge of the need for serial wound excision before definitive cover to minimise the incidence of wound infection.21
Due to a speedy and robust ISAF chain of evacuation, only two ISAF patients required more than a single operating theatre episode and only one spent more than 3 days at the MTF prior to aeromedical evacuation. This ideally takes place within 24–48 h of injury, during which time crucial burn resuscitation is ongoing.22–24 The predecessor to Critical Care Air Support Team aeromedical evacuation was the Burn Flight Team set up by US forces to evacuate critically ill burns patients in 1951 in Korea.25
Civilian
Due to a largely defunct Afghan healthcare system, unique issues were encountered in the management of civilians, which were not experienced in the management of ISAF personnel. Civilians spent significantly longer as inpatients than combat troops, with an associated impact on resources. There were ethical and professional implications of transferring patients to host nation facilities, for which no objective measure of scale or capability existed. Medical interventions at the MTF may be the only management received and so should be as definitive as possible,11 which must be borne in mind with regard to the complexity of intervention and potential lack of follow-up. Role 3 MTFs, usually scaled purely for resuscitation and stabilisation of casualties before repatriation, may now be expected to provide tertiary levels of inpatient care to local nationals. However, treating civilians at NATO MTFs also potentially risks dislocating local service provision, undermining reconstruction and development efforts and fostering military dependency.
Though not routinely scaled for or equipped to manage paediatric trauma, 31/88 burn patients were children, with associated paediatric-specific anaesthetic, resuscitative, surgical, nursing and instrumentation issues. Management of paediatric casualties should be planned and trained for pre-deployment.26
Medical Rules of Eligibility (MRE) state in general that emergency medical care should be provided to all non-ISAF personnel injured by conflict related activity, though not routinely outside this premise. Unfortunately, MRE cannot be detailed enough to provide guidance in all clinical scenarios, leaving room for interpretation, possible challenging ethical scenarios and potential logistical implications.
Conclusions
The management of burns at war is a complex process, further complicated by the management of non-conflict burns in civilians. It requires a well coordinated multidisciplinary team and correct allocation of resources in order to achieve the greatest good for the greatest number and ultimately to achieve the mission aim. Though the mechanism and pattern of burn injury have to some extent evolved in 21st century conflict, the findings largely reflect recent US data from Iraq and Afghanistan, with the management of patients with burn injuries continuing to have a recognisable logistical impact on resources at deployed Role 3 MTFs. The management of burns in civilian patients takes up a predictable amount of theatre time, nursing time, dressing resources and bed space, which must be planned for in current and future deployed operations.
Acknowledgments
The authors thank the following individuals and organisations for help in collecting, collating and identifying the appropriate data for this paper: Cdr Bosy USN, Cdr Folin USN, Maj Rajski USMC, Joint Combat Casualty Research Team (JCCRT), US Army Institute for Surgical Research, Academic Department of Military Emergency Medicine (ADMEM) and Defence Analytical Services and Advice (DASA).
References
Footnotes
-
Contributors JAJ, is responsible for primary authorship of the paper, including literature review and data analysis. ANP sought permissions from relevant authorities, before collecting and collating data in the field, setting the direction of the work and reviewing the progress throughout. He is responsible for overall content as guarantor.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement Due to the potentially sensitive nature of the unpublished data from the study, it cannot be made publicly available.