Article Text

Abstract
Introduction Evidence from civilian athletes raises the question of whether reproductive dysfunction may be seen in female soldiers as a result of military training. Such reproductive dysfunction consists of impaired ovulation with or without long-term subfertility.
Methods A critical review of pertinent evidence following an extensive literature search.
Results The evidence points towards reduced energy availability as the most likely explanation for exercise-induced reproductive dysfunction. Evidence also suggests that reproductive dysfunction is mediated by activation of the hypothalamic–pituitary–adrenal axis and suppression of the hypothalamic–pituitary–gonadal axis, with elevated ghrelin and reduced leptin likely to play an important role. The observed reproductive dysfunction exists as part of a female athletic triad, together with osteopenia and disordered eating. If this phenomenon was shown to exist with UK military training, this would be of significant concern. We hypothesise that the nature of military training and possibly field exercises may contribute to greater risk of reproductive dysfunction among female military trainees compared with exercising civilian controls. We discuss the features of military training and its participants, such as energy availability, age at recruitment, body phenotype, type of physical training, psychogenic stressors, altered sleep pattern and elemental exposure as contributors to reproductive dysfunction.
Conclusions We identify lines of future research to more fully characterise reproductive dysfunction in military women and suggest possible interventions that, if indicated, could improve their future well-being.
- SPORTS MEDICINE
Statistics from Altmetric.com
Key messages
Evidence suggests that reproductive dysfunction could be prevalent among female military trainees.
The pathology associated with such reproductive dysfunction is associated with reduced energy intake and could predispose women to injury.
Evidence from civilian athletes points to reduced energy availability as the key cause. Other factors specific to military training may also be likely to contribute.
Further research could be beneficial in assessing the scale of reproductive dysfunction in UK military women and understanding its aetiology.
There are a number of interventions that, if necessary, could theoretically reduce or even prevent significant reproductive dysfunction and its associated pathologies.
Introduction
Understanding of the relationship between exercise and reproduction has significantly evolved in recent years. ‘Athletic amenorrhoea’ has been observed in civilian athletes for many decades,1 ,2 while more recently studies have demonstrated a high prevalence of amenorrhoea in basic military training.3 ,4 Unlike athletics, military training is not intended to optimise performance in a specific sport and is more task-orientated. For example, exposure to extremes of temperature, psychological stressors and prolonged, heavy load carriage are important for military output and may carry physical risks (eg, stress fracture) that civilian athletic training might not.5 ,6 This review focuses predominantly on basic military training, which generally lasts several months. Most basic military trainees are adolescents in their late teens, presenting additional challenges to reproductive homeostasis.4 ,7
Consideration of reproductive dysfunction in the military is important not only due to the potential for sustained subfertility in individuals but more widely as a surrogate of non-reproductive pathologies that might impact operational effectiveness. Potential reproductive dysfunction, when understood, might be prevented or at least the risk reduced.
The purpose of this paper is to explore what is currently known about the scale and aetiology of reproductive dysfunction in military training and the impact of associated conditions. As a preface to this, methods used to measure female reproductive function are described, and hypothalamic adaptations to exercise and the role of brain energy availability are discussed. Other associated pathologies are described, and military-specific risk factors are also considered. The case for further research and potential strategies for prevention is outlined.
Methods
Articles published from 1939 to 2016 were identified using PubMed, Ovid Medline and Google Scholar for combinations of the following search terms (truncated): military, exercise, sport, physical activity, endocrine, reproductive, menstrual, ovulation. Bibliographies of relevant articles were reviewed for relevant publications, and subsequent citations (identified through Google Scholar) were also included.
Reproductive dysfunction is defined here as any endocrine imbalance that could impair normal ovulatory menstrual cycles. Military training is defined as the necessary means for initiation into combat roles (‘basic training’) or to maintain generic soldiering skills (‘career-long training’) and places significant demands on the trainee physically and psychologically.5 ,6
Measuring reproductive health
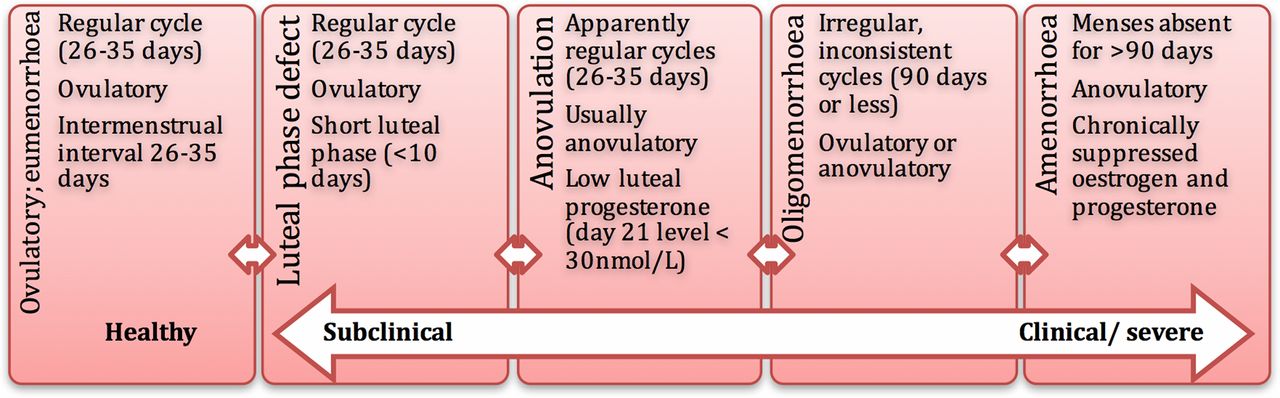
Dysfunction of reproductive homeostasis is complex. The terms used to describe it are explained in Table 1.8 Regular eumenorrhoeic cycles do not confirm ovulation and are by no means a guarantee of normal reproductive function.9 An anovulatory cycle may be short, normal or long, but no oocyte is released. In military studies, menstrual function has been assessed using questionnaires,4 ,10–12 as in civilian athlete studies.13 ,14 Such questionnaires generally involve an assessment of menstrual onset, duration and frequency constructed by the investigators, defining clinical menstrual disorders as outlined in Table 1. No study stated if the questionnaires used to determine menstrual regularity in athletes were validated. Questionnaires can be misleading due to cycle duration variability seen typically in athletes, and the observation of menstrual regularity does not signify normal ovulation.15 ,16
Repeated ultrasound examination with serum hormone assay are the most accurate means of demonstrating the development and disappearance of an ovarian follicle. While the former is too invasive to have gained widespread use as a research tool,18 a sustained, elevated progesterone in the luteal phase is often accepted as evidence that ovulation has taken place.19 The luteal phase may be shortened or absent, even within a normal length menstrual cycle, when a predetermined midluteal progesterone cut-off is not reached (a ‘luteal phase defect’ (LPD), Table 1).18 Due to difficulty demonstrating the midluteal point in athletes with variable cycle lengths, serial samples are needed, which can be challenging in large numbers. Measuring urinary pregnanediol glucuronide (PDG), a metabolite of progesterone, offers greater convenience than blood sampling. While not routinely available in clinical practice, in research it is normally the measurement of choice.18 ,20
Assessing the prevalence of menstrual disorders in military training
The spectrum of reproductive function and dysfunction is illustrated in Figure 1. The studies describing the prevalence of reproductive dysfunction associated with military training are summarised in Table 2.4 ,10–12 ,21 ,22 A wide range of prevalence is reported and the definitions used differ, making meaningful interpretation difficult. For example, Friedl et al and Lauder et al identify different amenorrhoeic timeframes, whereas Schneider assesses a continuum of irregularity. The studies appear to be subject to selection bias; for example, Lauder et al 23 reported that reserve officer cadets were too busy to undertake a survey and were thus excluded from further analysis. Soldiers receiving a mail survey might be more likely to have responded if they had undergone menstrual disturbance.10 Recall bias can also hamper results since menstrual disturbances are reported more frequently with short-term rather than long-term recall (which was used in all other studies). None of the studies describe the actual questions asked, so it is unclear if some of the questions were ‘leading’.11 Such problems arising with surveys are not addressed, for example, by measuring serial urine PDG.
Comparison of relevant studies assessing menstrual disturbance in military trainees

Spectrum of reproductive function and dysfunction observed in athletes, adapted from review by Mallinson, De Souza.8 Menstrual health exists at one end of a continuum (represented by the arrow), ranging from subtle, subclinical adaptations such as shortening of the luteal phase, to severe clinical amenorrhoea.
Given the paucity of data on the prevalence of reproductive dysfunction in female military personnel, we consider the civilian athletic literature. In a systematic review of all athletic disciplines, Gibbs et al 14 report the prevalence of menstrual dysfunction to be 1–60% (34 studies, n=5607).14 Such a wide variation in the prevalence of menstrual disturbance could be accounted for by the specific population (eg, factors such as selection bias and under-reporting) or methodological variations. However, it is clear that the prevalence of reproductive dysfunction among a training population is significantly greater than in the general population, where the prevalence of amenorrhoea ranges from 2% to 5%.24 ,25
Hormonal contraception
A significant challenge to estimating the prevalence of reproductive dysfunction is presented by hormonal contraceptives (Table 2). The use of hormonal contraceptives can be particularly high in soldiers, and in a recent review has been shown to range from 16% to 34% for oral contraceptives, 4% to 11% for injectable medroxyprogesterone, 3% to 9% for the hormonal patch 2% implants and 0% to 3% for intrauterine devices. The use of all forms of hormonal contraceptive is higher in soldiers when deployed.26
Hypothalamic adaptations to exercise
The female hypothalamic–pituitary–gonadal axis in exercise
The response of the female hypothalamic–pituitary–gonadal (HPG) axis to exercise and stress can more aptly be described as a functional adaptation than a disease process, and indeed the term ‘functional hypothalamic amenorrhoea’ (FHA) is often used (Table 1).8 ,18
The pattern of HPG adaptation seen varies by activity type and may be influenced by whether the physical characteristics of athletes are lean or non-lean (Table 1). In a systematic review, the prevalence of menstrual disturbance was higher in lean compared with non-lean sports (1–28% vs 0–17%, five studies, n=1032, no p value given).14 However, the physical characteristics required for military roles are less dichotomous, involving a combination of muscle strength and endurance, power and aerobic fitness.
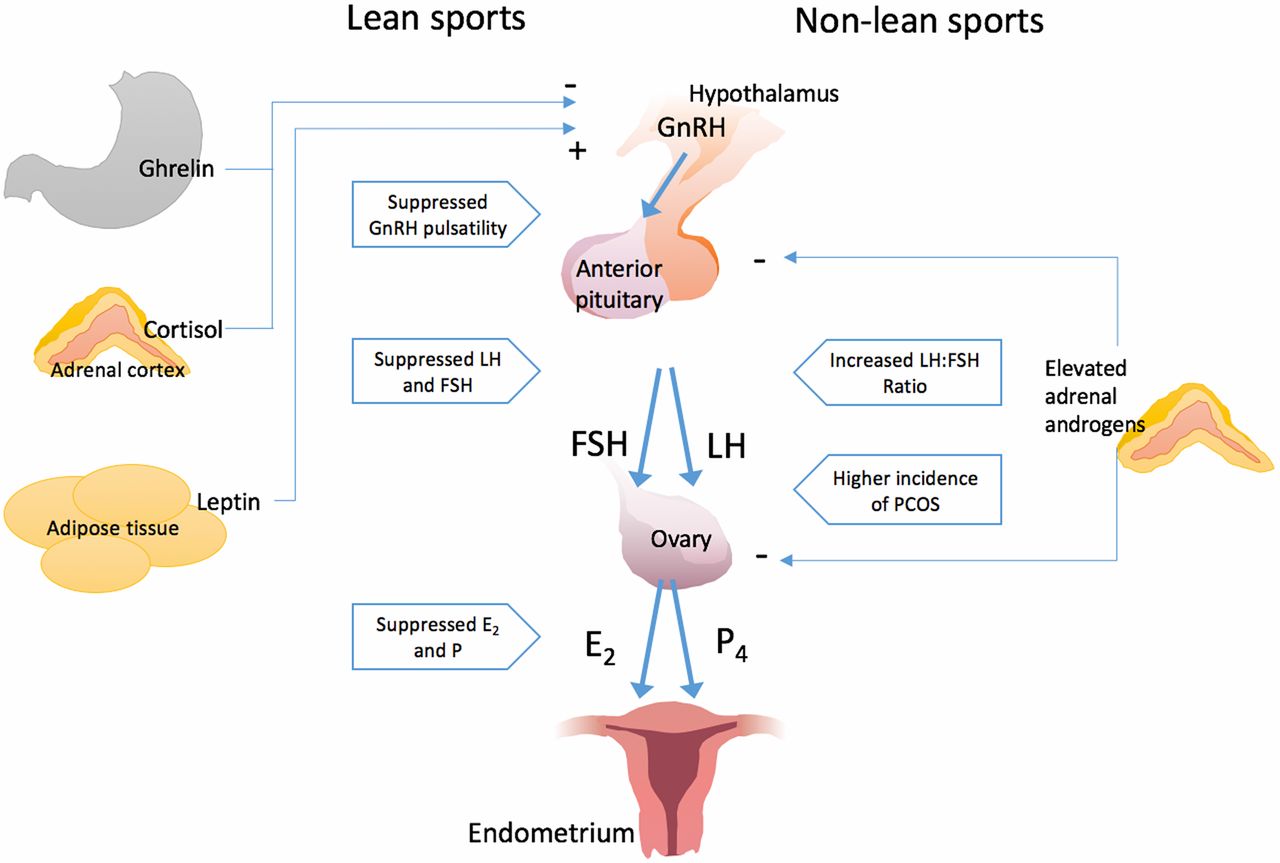
The purported adaptations of the HPG axis to exercise in lean and non-lean athletes are summarised in Figure 2. Suppression of the entire HPG axis in athletes from lean sports contrasts with hyperandrogenism and increased luteinising hormone (LH):follicle-stimulating hormone (FSH) ratio seen in athletes from non-lean sports. In the latter, it is not clear if hyperandrogenism is a consequence of the training or a result of self-selection. It appears that the effect of training on reproductive function in non-lean sports is less extensively studied.2 ,27

Simplified comparison of hormonal interactions with the hypothalamic–pituitary–gonad axis in athletes undertaking lean and non-lean sports.112–114 In athletes undertaking lean sports, reproductive dysfunction is characterised by elevated cortisol and ghrelin and reduced leptin. Suppression of normal pulsatile gonadotropin-releasing hormone (GnRH) release reduces pituitary follicle-stimulating hormone (FSH) and luteinising hormone (LH) release, altering ovarian follicle development, which reduces E2. Failure of ovulation results in low P. This prolongs the follicular phase leading to ineffective, shortened or absent luteal phases. In non-lean sports, the LH:FSH ratio tends to be increased, androgen levels are elevated and there is a propensity to polycystic ovarian syndrome (PCOS). High levels of androgens may lead to a blunted LH surge and direct impairment of follicular development. E2, Estradiol; P4, Progesterone; FSH, follicle stimulating hormone; LH, luteinising hormone; GnRH, Gonadotrophin releasing hormone; PCOS polycystic ovarian syndrome.
Interplay between energy availability, stress and reproductive dysfunction in exercising women
Three distinct hypotheses have emerged to explain the reproductive dysfunction observed in athletes. The body composition hypothesis was based on the observed correlation that menstrual function is lost below a threshold of fat mass, as is observed in women with anorexia nervosa.28 However, subsequent studies observed a range of body size and composition in both eumenorrhoeic and amenorrhoeic athletes.29–31 The ‘exercise stress hypothesis’, that activation of the hypothalamic–pituitary–adrenal (HPA) axis leads to amenorrhoea,1 was based on the observation that exercise is associated with elevated cortisol levels.17 This was thought to explain the observations of Nagata et al,32 who documented amenorrhoea in most Japanese nursing students during their highly stressful term, which resolved during the summer holidays. However, studies failed to control for the energy cost of exercise and the way the exercise was implemented experimentally.17 ,33–36
The most prominent hypothesis is that of reduced energy availability (defined in Table 1), emerging from the work of Winterer et al 37 in the 1980s, who proposed mammals partition energy hierarchically across six processes in the following order: cellular maintenance, thermoregulation, locomotion, growth, reproduction and storage. Where fuel is spent on one process, such as locomotion, it is unavailable for another, reproduction.38 It is postulated that inadequate energy availability to reproductive centres in the hypothalamus leads to HPG axis disruption.30
Loucks et al 17 performed a series of short studies comparing sedentary and active eumenorrhoeic women, in whom energy intake was manipulated to limit energy availability. Over five consecutive days of exercise, limiting energy intake resulted in suppressed LH pulsatility, while exercise without dietary restriction had significantly less effect. The question remained: does energy availability exert this effect per se or is another component of exercise responsible? Work by Williams et al 39 delineated these factors; in rhesus monkeys with exercise-induced amenorrhoea, dietary supplementation restored normal menstruation against controls. The same effect was shown in humans in laboratory studies, supporting the hypothesis that exercise per se has no effect on the hypothalamus beyond that of decreasing energy availability.40 ,41
A study in arduous US Army Rangers controlled for the metabolic impact of exercise in a field training environment. Restricted diets (5000 and 2000 kcal per day on alternate days) were given to Rangers undergoing arduous training, alongside heat, cold and psychological stressors (soldiers were exposed to four 2-week phases in desert, forest, mountain and swamp environments).42 LH and testosterone were suppressed. In a second cohort undergoing the same training 1 year later, who were fed an additional 400 kcal per day, LH and testosterone reached near-normal levels despite continued exposure to stressors. However, psychological stress was not measured, the key ‘stressor’ being described by the authors as dietary restriction itself. It is difficult to delineate psychological stress from energy deficiency in a field study without quantification of stress or contemporaneous placebo control.
Reproductive dysfunction seen in exercising women is most likely an adaptation to survive a period of energy deficit by prioritising energy supply for exercise over reproductive function.43–46 This is not in one sense a defect as it serves to conserve energy for the individual and can be reduced with sufficient energy intake.18 Reduced energy availability, notably below 30 kcal/kg lean body mass/day, has become the best explanation of exercise-induced reproductive disturbance, especially in lean athletic pursuits.17 ,45 ,47
Ghrelin, leptin and cortisol
It has been suggested that changes in the anorectic adipokine leptin and orexigenic (appetite stimulating) gut peptide ghrelin mediate reproductive dysfunction during negative energy balance.48 ,49 Leptin is released after eating while ghrelin is secreted during fasting. Their primary roles have traditionally been thought to be signalling of satiety and hunger.50 ,51 FHA is associated with disproportionately low levels of leptin and high levels of ghrelin.48 ,49 ,52 ,53 Welt et al 54 successfully used recombinant leptin to restore the menstrual cycle and levels of sex steroids and gonadotropins in women with FHA. These results have been replicated such that it seems that there is a critical leptin threshold below which FHA occurs.55
Despite refutation of the exercise stress hypothesis (ie, that activation of the HPA axis solely leads to reproductive dysfunction) in favour of the energy availability hypothesis,41 the observation remains that FHA is associated with elevated central and peripheral levels of cortisol.36 ,56 Vulliémoz et al 57 demonstrated this in female rhesus monkeys, in whom negative energy balance and reproductive dysfunction had been induced by ghrelin infusion. LH pulsatility was restored following an infusion of astressin B, a corticotrophin-releasing hormone antagonist. This suggests that normalising cortisol production could reduce the effect of energy availability on reproductive function.57
Subsequently, in a cross-sectional analysis of overnight hormone levels in adolescent amenorrhoeic endurance athletes, Ackerman et al 36 demonstrated cortisol levels were independently associated with reduced LH pulsatility after correcting for leptin, ghrelin and fat mass. These studies suggest that the action of gut peptides in the reduced energy availability state is mediated through activation of the HPA axis.
It follows that other means of HPA axis activation may also compound reproductive dysfunction, such as psychological stressors observed in military training.5 This is illustrated by the use of cognitive behavioural therapy to treat FHA successfully.58 Indeed, psychological stress (perceived as threat) can impair food intake.59 Since the introduction of functional neuroimaging, we know that the brain is one of the most metabolically active organs in the body. A combination of small synergistic stressors may cause significant reproductive dysfunction in an HPG axis already sensitised by energy deficiency over time.60 Thus, recent research findings integrate aspects of the energy availability, stress and body composition hypotheses (leptin is produced in proportion to fat cell mass), demonstrating that complex interactions between hormonal axes, nutrition and energy storage are responsible for reproductive dysfunction.
Female athletic triad
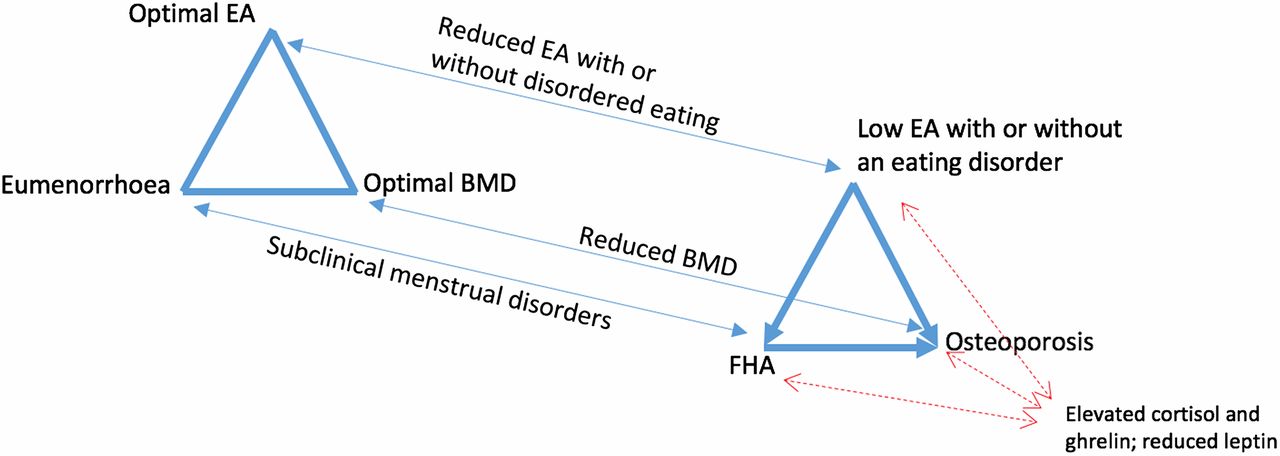
Much research into reproductive dysfunction has emphasised the female athletic triad (Triad).17 The Triad was defined in the 1990s by the presence of disordered eating (DE), functional amenorrhoea and subsequent premature osteoporosis,61 and was subsequently revised to encompass a spectrum of reproductive dysfunction, osteopenia and reduced energy availability (Figure 3).46 Cross-sectional studies in various exercising populations (including military trainees) demonstrated a low prevalence of two or more components concurrently.12 ,25 ,62 ,63 However, such studies were hampered by stringent inclusion criteria and variable definitions of the components (eg, self-reported menstrual regularity vs anovulation determined by serial hormonal measurement).

{kind=link}
{kind=link}
{kind=link}
The female athletic Triad. BMD, bone mineral density; EA, energy availability; FHA, functional hypothalamic amenorrhoea. Adapted from the American College of Sports Medicine position stand, 2007.46 EA, menstrual function and BMD exist in a clinical spectrum, along which athletes are distributed (thin arrows), An athlete moves either left or right along the spectrum according to exercise and diet practice. Energy availability modulates BMD indirectly via effects on menstrual function and ‘directly’ via changes in metabolic hormones, notably leptin and ghrelin (thick arrows). All three aspects are associated with changes in the HPA axis and gut hormones (red dashed arrows). BMD, bone mineral density; EA, energy availability; FHA, functional hypothalamic amenorrhoea.
The Triad includes DE, which refers to abnormal behaviours of limiting food intake to achieve or maintain a desired body image, as opposed to an eating disorder (ED), which may reflect these symptoms but refers to a distinct psychological disorder like bulimia nervosa or anorexia nervosa.64
The Triad also encompasses changes in bone mineral density (BMD), the clinical endpoint being osteoporosis. Reduced BMD may be frequently missed as it does not cause symptoms prior to fracture.8 ,25 However, revised definitions may extend to stress fractures, a common overuse injury in military trainees, especially in women.65–67 Reproductive dysfunction may possibly increase the risk of stress fractures in female military trainees, but the precise aetiology of stress fractures remains unclear.
Lauder et al's12 cross-sectional analysis assessed Triad prevalence in cadets at West Point Military Academy, USA. Only 3% of cadets demonstrated osteopenia, although the study was limited in its design, since only cadets with menstrual irregularity or at risk of DE underwent BMD assessment, and those on hormonal contraceptives were excluded. However, all cadets were screened for ED. Of significant concern was that 8% of participants met the criteria for an ED, while 26% were deemed to be at risk of one, which is comparable with studies in civilian athletes.14
The International Olympic Committee recently proposed that, beyond the Triad, relative energy deficiency in sports causes broader physiological impairment, including but not limited to metabolic rate, menstrual function, bone health, immunity, protein synthesis and cardiovascular health in men and women.68
Other aetiological factors in military women
Dietary insufficiency
The aforementioned studies by Loucks et al and Williams et al demonstrated that the suppression of LH pulsatility following dietary restriction could be reversed when the restriction was lifted.17 ,40 ,69 The degree of energy deficit was recently shown to alter the frequency but not severity of menstrual disturbance in a small cohort undergoing supervised laboratory-based exercise.70 The importance of micronutrient content as well as caloric content was suggested from a pragmatically designed study by Andrews et al,71 who reported an inverse association between LPD and increased fibre, isoflavane and Mediterranean diet score.
Unintentional dietary restriction is a common component of military training. Dietary restriction may also be intentionally imposed, as noted by Hoyt and Friedl72 in their review of field studies in US and Norwegian Rangers, US Marines and others. Their own study was unusual in that they recruited female as well as male soldiers, who endured 7 days of prolonged physical activity, starvation and sleep deprivation, during Ranger training in Norway.73 Their findings demonstrated increased usage of fat mass for energy reserve in women compared with men; women lost less weight than men but burned proportionately more fat. The authors did not assess menstrual dysfunction, ghrelin or leptin, and further research is indicated (Table 3).72 Energy deficit was also demonstrated in soldiers in barracks, using 24-hour recall in 324 soldiers of 101st Airborne division by Beals et al. 74 Just 15% of males and 13% of females admitted eating the recommended amount of carbohydrate, with no significant differences between groups. However as the authors acknowledge, their non-automated, single-interview 24-hour recall method is likely to have contributed to under-reporting.75
Recommendations for further research on reproductive dysfunction in female military trainees
Not all dietary restriction experienced by military women is imposed by the training regimen. In civilian athletes, DE purportedly contributes to reduced energy availability in association with physical training. It is perhaps surprising that DE, and even overt EDs, were apparently so prevalent in the aforementioned study of West Point cadets.12 However, such observations have been made across a wide spectrum of sports, including lean and non-lean activities; the prevalence in endurance, technical and ball game sports (24%, 17% and 16%, respectively) being significantly greater than controls (4.6%; p<0.001).97 DE is a significant problem in sports medicine, and it is suggested that coaches and physicians routinely look for early evidence in athletes.98
Age
The gynaecological age is taken as the number of years after menarche (mean age 12 years). Typically women achieve the highest rate of ovulatory cycles (94%) at gynaecological age 12 years, and as female athletes advance beyond this age, the effect of intense training on reproductive function may be attenuated.18 ,69 Many studies demonstrating LPD following reduced energy availability recruit women in their early to mid 20s, to remove gynaecological maturity as a confounding variable.95 However, most military recruits are younger than this,7 and a recent, comprehensive review indicates substantially increased vulnerability to reproductive dysfunction in athletes, conferred by gynaecological age <15 years.99
Adolescence is an important time for bone mineral accrual.100 While the majority of bone mass is achieved by age 19, some cadets may have not achieved peak bone mass by the time of training,99 and any losses may have an impact on subsequent peak bone mass.14 ,99
Younger age might also accentuate any impact the psychological element of military training has on reproductive function. Sports that expose adolescents to high levels of psychological stress are associated with hypercortisolaemia and menstrual disruption,99 while the developing emotional maturity of adolescence may also confer susceptibility to anxiety about body image and DE.101 Women might be particularly affected.100 ,101
Type of physical training
Military training has traditionally focused on aerobic fitness, although military roles, particularly those of ground close combat, require a combination of strength, power, endurance and aerobic fitness. Most published studies relate to training for lean sports, and there is a paucity of literature describing the effect of strength and power training on female reproductive function.2 Training for non-lean sports is associated with increased muscle mass rather than low body mass, and athletes tend to exhibit hyperandrogenism and modest elevations in LH:FSH ratio (Figure 2).2 ,14 ,95 In their military cohort, Lauder et al 12 speculate non-lean, high-impact training (eg, load-carriage) may have significantly increased BMD had their sample size been bigger.
Military training aims to improve submaximal performance for a sustained, non-predefined duration.6 It may involve abrupt onset sprinting carrying a load, without a warm-up. Such abrupt exercise onset has been shown to increase propensity to menstrual disturbance, while gradually introduced exercise had dramatically less effect on reproduction.99 ,102 ,103
Other aspects of training
The psychological challenges of military training include anticipatory stress, time management pressure, conflict between teamwork and leadership roles, and performance evaluation.6 A combination of physical and mental strain with sleep and food restriction led to marked reductions in LH:FSH and testosterone in male Norwegian soldiers, which improved following administration of gonadotropin-releasing hormone (GnRH) but not a high-caloric diet, suggesting higher suppression of the HPG axis. Temporarily elevated cortisol concentrations were followed by hypocortisolism in the recovery phase.6 ,104 ,105 While derived in men, these observations indicate that the stress of military training could adversely affect female reproductive function.
A study of female US Military personnel revealed the presence of menstrual disorders was strongly associated with increased likelihood of stressful life events compared with matched civilians.89 This included amenorrhoea (OR 2.20, 95% CI 1.08 to 4.50) and abnormal cycle length (OR 3.42, 95% CI 1.12 to 10.50). Women without exposure to a stressful life event were not at significantly altered risk. This study did not examine dietary, metabolic or biochemical parameters.
Other factors associated with military training, which confer additional risk for reproductive dysfunction, include sleep restriction, extreme elemental exposure and musculoskeletal injury.6 ,106 These should not be dichotomised from energy availability.99 All can be seen to disrupt the HPA axis and gut peptides, but there is little high-quality, prospective research considering the contributions of such factors to the Triad, especially in the military (Table 3).
Reproductive dysfunction in female athletes during intense exercise is preventable,107 suggesting that women should not be excluded per se from arduous training on the basis of their sex.5 ,17 ,108 Table 4 summarises potential mitigation strategies that, if indicated, might enhance the effectiveness of training and safeguard the long-term well-being of servicewomen.64 ,92 ,100
Potential future interventions to reduce reproductive dysfunction and its sequelae in military training
Conclusion
Arduous military training incorporates a multifaceted programme of physical and mental challenges. The energy availability hypothesis, while derived predominantly through small studies in civilian athletes, is putatively key to understanding the aetiology of reproductive dysfunction in female military trainees, influenced by the HPA axis and gut peptides. Hyperandrogenism observed in a subset of athletes may also play a part.
The evidence outlined here warrants further investigation to fully protect the health of female personnel operating in adverse conditions. It is important that military personnel are aware of the potential consequences of serving their country, especially when they are likely to do so before they have reached full physical maturity. The interventions suggested in Table 4 are hypothetical, as the status of female health within UK military training is not currently known. It is not yet clear if such interventions, which may be applicable to athletes, are relevant for military personnel due to the complex physical and mental stimuli of the military training and operational environment.
References
Footnotes
Contributors RG undertook the literature search, drafted the manuscript and drew the figures. DW, RR, RA and JG provided editorial input to the manuscript.
Competing interests The authors are engaged in planning a prospective study of female endocrine response to UK military training as part of and funded by the UK Defence Women in Ground Close Combat Research Programme.
Provenance and peer review Not commissioned; externally peer reviewed.